
Abstract
Background:
New Caledonia and French Polynesia have among of the world highest thyroid cancer incidence rates. Studies have demonstrated a relationship between anthropometric parameters and the prevalence of cancer. In this study we evaluated further the relationship between body mass index (BMI) and other anthropometric parameters on the incidence of thyroid cancer in the New Caledonia and French Polynesia populations.
Methods:
We performed a pooled analysis of two case–control studies in New Caledonia and French Polynesia. We included a total of 554 cases (65 men and 489 women) of differentiated thyroid cancers and 776 population control subjects matched on sex, age, and study. Anthropometric factors (height, weight, BMI, body fat percentage [BF%], and body surface area [BSA]), at age 18 and before diagnosis, were analyzed by conditional logistic regression, adjusting for other independent risk factors.
Results:
A high proportion of cases (73%) were overweight (25–29.9 kg/m2) or obese (≥30 kg/m2) before diagnosis of thyroid cancer (against 57% of control subjects). An increased risk of thyroid cancer was observed with greater height, weight, BMI, BF%, and BSA. The association of thyroid cancer risk with height, weight, BMI, and BF% did not remain when adjustment was made for BSA. By comparison, the odds ratios for the highest versus the lowest quartile of BSA at age 18 were 3.97 (95% confidence interval, 2.57–6.15; p < 0.001) for women and 4.06 (95% confidence interval, 1.03–16.06; p = 0.04) for men. The association between thyroid cancer risk and each of anthropometric factors did not depend on tumor size or menopausal status before diagnosis.
Conclusion:
Among anthropometric factors, BSA plays a dominant role in thyroid cancer risk and explains the apparent role of BMI.
Introduction
In meta-analyses of 5 cohort studies involving women (2) and of 12 case–control studies (10), the risk of thyroid cancer increased with greater height, weight, and BMI. In men, similar results were obtained in the meta-analysis of cohort studies (2), but height was the only factor associated with thyroid cancer in the pooled analysis of case–control studies (10).
New Caledonia and French Polynesia are two French territories in the South Pacific with 240,000 and 280,000 inhabitants of mostly Melanesian and Maori origin, respectively. They are characterized by incidences of obesity and a thyroid cancer that are among the highest in the world. In French Polynesia in 2002, based on the World Health Organization classification that defines obesity to be present when the BMI is ≥30 kg/m2, 40% of the women and 38% of the men were obese (11). In New Caledonia from 1992 to 1994, based on relative weight index of 120% of ideal weight in which obesity was defined as a BMI of ≥25 kg/m2 for women and ≥27 kg/m2 for men, 57% of the women and 45% of the men were obese (12). Between 1985 and 1999, age-standardized incidence rates (world standard population) of differentiated thyroid cancer as high as 71.4 and 24.6 per 100,000 were observed among Melanesian women in New Caledonia (13) and native women of French Polynesia (14), respectively. In contrast, the incidence rates of thyroid cancer in developed countries ranged from ∼3 to 8 per 100,000 women (15).
Therefore, New Caledonia and French Polynesia provide a unique opportunity to investigate the relationship between the incidences of obesity and thyroid cancer.
There are at least two case–control studies of the incidences of obesity and thyroid cancer in New Caledonia and French Polynesia (16,17). Each of them independently reported an association between increased height, weight, BMI, and increased thyroid cancer risk. The number of men, however, was too small in each of these studies to provide stable results. In the present analysis, therefore, we pooled the data of these two studies to clarify the association between anthropometric parameters and thyroid cancer risk and to ascertain the relative importance of these parameters, especially that of BMI and BSA.
Materials and Methods
Study population
This study was approved by the Ethics Committees of French Polynesia and metropolitan France. Written informed consent was obtained from all participants to contact their physician. The study populations and the methods used for data collection have previously been reported (17,18). A total of 561 cases and 785 control subjects were included. In both studies the subjects and population control subjects were matched by sex and age, and provided questionnaire data during face-to-face interviews (Table 1). In Table 1, the characteristics of the thyroid cancer—histology, size of tumor, diagnosis period, and age at diagnosis—were obtained from pathology laboratories of French Polynesia and New Caledonia. Ethnicity and anthropometric parameters were obtained from face-to-face interviews.
After exclusion of seven cases and nine control subjects who were <18 years old at the time of cancer diagnosis or corresponding time for control subjects.
For 26 cases in French Polynesia, we have no information about tumor size.
Age at diagnosis for cases and corresponding age for control subjects.
BMI, body mass index; BSA, body surface area (Boyd).
Parameters
Cases and control subjects reported their height and weight at the age of 18 and before the diagnosis of thyroid cancer or at a corresponding date for the control subjects. Seven cases whose cancer was diagnosed before the age 18 and nine control subjects were excluded from the analysis because one of our objectives was to investigate the role of the weight increase between age 18 and the diagnosis of thyroid cancer. Therefore, a total of 554 cases (489 women and 65 men) and 776 control subjects (671 women and 105 men) were included in the analysis.
BMI was defined as weight (kg) divided by height (m) squared. Deurenberg et al.'s formula, where age is in years and S is the sex (S = 0 for women; S = 1 for men) was used to calculate body fat percentage (BF%) (19) and is presented below.
BSA, where W is the weight in g, H is the height in cm, and log is the decimal logarithm, was obtained using Boyd's formula (20), presented below.
We also used two other methods, where W is the weight in kg and H is the height in cm, to calculate BSA. These are presented below.
Mosteller's formula (21) is the most simple one for calculating BSA, the Dubois and Dubois (22) formula is most often used, and Boyd's formula (20) is the most accurate.
Anthropometric factors were categorized into quartiles based on the distribution among control subjects. Standard BMI categories were also used: <18.5 kg/m2 (underweight), 18.5–24.9 kg/m2 (reference), 25–29.9 kg/m2 (overweight), and ≥30 kg/m2 (obesity) (23).
Statistical analysis
Data were analyzed using conditional logistic regression (24) with SAS software, version 9.1 (SAS Institute, Cary, NC). Analyses were stratified by 5-year age classes, study, and sex, and therefore produced results similar to that which would be obtained with proportional hazard regression model (25). Some analyses were conducted separately for men and women, because risk factors may differ by sex. For women, additional analyses were conducted according to ethnicity (Melanesian, Polynesian, or others), size of cancer, number of children, and menopausal status using the age at diagnosis (≤50 or >50 years) as a proxy (26). Analyses according to the size of the thyroid carcinoma (≤10 or >10 mm) were conducted because the discovery of occult microcarcinomas (≤10 mm) may depend on thyroid cancer screening and could be enhanced in overweight persons.
All odds ratios (OR) were adjusted for ethnicity (Melanesians, Polynesians, or others), education level (never went to school, primary school, secondary school, or university degree), smoking (never, past, or current), head or neck exposure to medical X-ray irradiation before the age of 15 (yes or no), and, for women, the number of full-term pregnancies (continuous) (except in analysis by number of children), which were identified as risk factors in a previous analysis (16,26). All p-values presented are two-sided, and p < 0.05 was considered statistically significant. Tests for trend were performed by assigning the median value to each quartile, and then modeling this as a continuous variable using the Wald chi-square statistic.
Tests for interaction (24) were performed to assess if height, BMI, and BSA association with thyroid cancer risk was modified by characteristics such as sex, ethnicity, number of children (nulliparous, one to three children, or four or more children) and age at diagnosis (≤50 or >50 years). We also conducted analyses on BSA change between age 18 and diagnosis.
Multivariate analysis aiming to compare the role of height, weight, BMI, BF%, and BSA was performed using the reported values, and after taking into account colinearity by mean-centering the variables, the procedure being done separately for men and women. All these analysis were also repeated using the Pecan module of the computer software package Epicure (HiroSoft International Corporation, Seattle, WA), to verify our results when modeling the excess of OR as a linear function of the value of these parameters, rather than as a logistic one.
Results
Height, BMI, and BF%
Papillary carcinoma was the histological type in 83% of cases (Table 1).
Overall, more cases were overweight or obese before diagnosis of thyroid cancer (31% and 42%, respectively) than control subjects of corresponding age (29% and 28%). Tallness at age 18 and before diagnosis was associated with an increased risk of thyroid cancer in both men and women, whereas the association with BMI and BF% was significant only in women (Table 2). Similar results were observed when using World Health Organization BMI categories: overweight women at age 18 and before diagnosis had an increased risk of thyroid cancer (results not shown).
OR were adjusted for ethnicity (Melanesians, Polynesians, or others), educational level (never went to school, primary school, secondary school, or university degree), smoking (never, past or current), radiation to head or neck for diagnosis before 15 years old (yes or no), and also for the number of full-term pregnancies among women (continuous).
p for trend (two-sided) across categories is based on the median anthropometric variable within quartiles as a continuous variable and was calculated using the Wald chi-square statistic.
These categories also correspond to the following BF% quartiles in women: ≤21.1, 21.2–23.4, 23.5–25.9, and ≥26.0; and in men: ≤11.7, 11.8–14.1, 14.2–16.9, and ≥17.0.
Ca, number of cases; Co, number of control subjects; OR, odds ratio; CI, confidence interval; BF%, body fat percentage.
When detailing results in women according to ethnicity (Fig. 1), increased BMI and BF% at age 18 and before diagnosis was similarly associated with increased thyroid cancer risk in Melanesian and Polynesian women (p > 0.2 for difference between Melanesians and Polynesians at age 18 and before diagnosis), whereas the association with increased height was not significant in Melanesians. Results for the other ethnic group (Europeans and Asians) were similar.

Forest plot of ORa of thyroid cancer associated with anthropometric factors according to ethnicity among women. aOR were adjusted for educational level (never went to school, primary school, secondary school, or university degree), smoking (never, past or current), radiation to head or neck for diagnosis before 15 years old (yes or no), and the number of full-term pregnancies (continuous). p for trend (two-sided) across categories is based on the median anthropometric variable within quartiles as a continuous variable and was calculated using the Wald chi-square statistic. aThese categories also correspond to the following BF% quartiles: ≤21.1, 21.2–23.4, 23.5–25.9, and ≥26.0. BF%, body fat percentage; BMI, body mass index; BSA, body surface area (Boyd); OR, odds ratios.
Forty-six percent of women cases had a tumor size >10 mm. The associations between height, BMI, BF%, and the risk of thyroid cancer were similar in women who had a microcarcinoma (≤10 mm) and in other women (carcinoma size >10 mm) (results not shown).
Due to inclusion criteria in the study in French Polynesia (Table 1), 33% of women were >50 years old at time of cancer diagnosis or corresponding time for control subjects: this threshold was used as a proxy of the menopausal status. Among these women, 46% were Melanesians and 20% were Polynesians. We observed similar associations between anthropometric parameters and thyroid cancer risk in women 50 years old or less and in those older (results not shown).
Body surface area
High BSA at age 18 and before diagnosis was associated with an increased risk of thyroid cancer in both men and women (Table 2). A particularly strong relation was evidenced with the BSA at age 18; the risk for the highest quartile compared with the lowest for women was 3.97 (95% confidence interval [CI], 2.57–6.15; p for trend <0.001; [≥1.68 vs. ≤1.47 m2]) and for men was 4.06 (95% CI, 1.03–16.06; p for trend = 0.04; [≥1.87 vs. ≤1.66 m2]; p = 0.81 for difference between men and women) (Table 2 and Fig. 2).
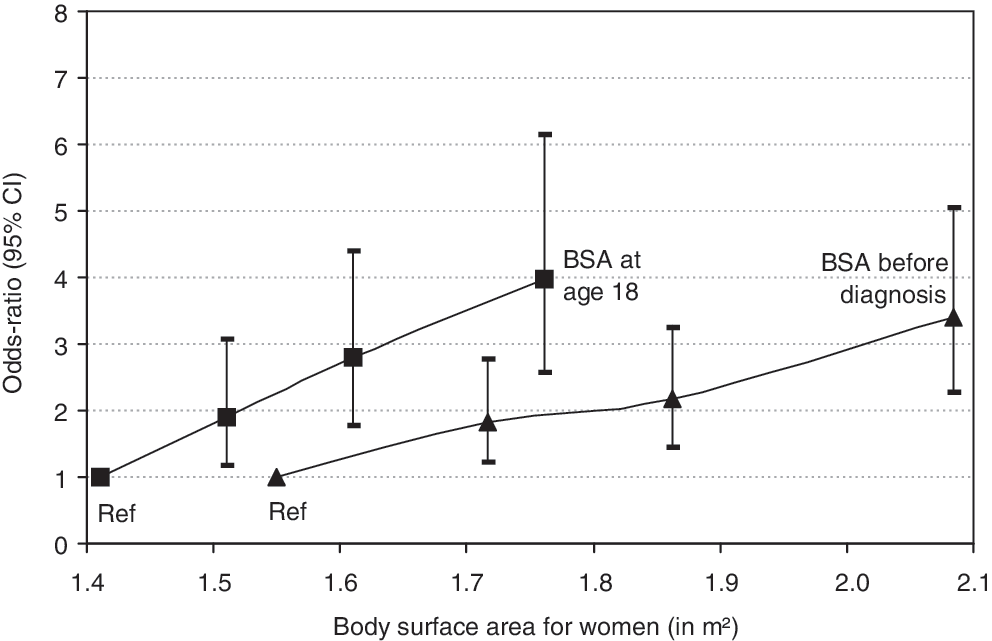
ORa of differentiated thyroid cancer according to quartiles of BSA at age 18 and before diagnosis for women. aOR were adjusted for ethnicity (Melanesians, Polynesians, or others), educational level (never went to school, primary school, secondary school, or university degree), smoking (never, past, or current), radiation to head or neck for diagnosis before 15 years old (yes or no), and the number of full-term pregnancies (continuous). CI, confidence interval.
When detailing results in women according to ethnicity (Fig. 1), increased BSA at age 18 and before diagnosis was similarly associated with increased thyroid cancer risk in Melanesian and Polynesian women (p ≥ 0.2 for difference between Melanesians and Polynesians at age 18 and before diagnosis). Results for the other ethnic group (Europeans and Asians) were similar, although the association at age 18 seemed stronger in this other ethnic group: the OR for the highest quartile (≥1.68 vs. ≤1.47 m2) were 2.35 (95% CI, 0.97–5.71) in Melanesian women, 3.71 (95% CI, 1.94–7.07) in Polynesian women, and 6.34 (95% CI, 2.44–16.47) in the other ethnic group.
The association between BSA and the risk of thyroid cancer did not depend on the tumor size nor on the menopausal status (results not shown).
The relation between BSA at age 18 and thyroid cancer risk did not vary according to the number of children. The OR for the highest quartile (≥1.68 vs. ≤1.47 m2) were, respectively, 3.56 (95% CI, 0.68–18.53; p for trend = 0.07), 3.73 (95% CI, 1.97–7.07; p for trend <0.001), and 3.28 (95% CI, 1.68–6.40; p for trend <0.001) for nulliparous women, women having one to three children, and women having four or more children. When considering BSA before diagnosis, these OR (≥1.97 vs. ≤1.63 m2) were, respectively, 7.06 (95% CI, 1.89–26.35), 3.26 (95% CI, 1.86–5.74), and 2.65 (95% CI, 1.35–5.18).
Because of dependence between BMI and BSA, which are both calculated from height and weight, we included anthropometric parameters only by pair (2 × 2) in the multivariate analysis. BMI remained significant when adjusting for height, and did not play any significant role when controlling for weight or BSA (Table 3). Conversely, BSA added significant information whichever other anthropometric parameters (height, weight, BMI, or BF%) were taken into account.
Adjusting for ethnicity (Melanesians, Polynesians, or others), educational level (never went to school, primary school, secondary school, or university degree), smoking (never, past or current), radiation to head or neck for diagnosis before 15 years old (yes or no), and the number of full-term pregnancies among women (continuous). All statistical tests were two-sided.
In another model where BSA at age 18 and BSA change between age 18 and age at diagnosis were included, both variables were associated with increased thyroid cancer risk. The OR per m2 increase of the BSA at 18 was 22 (95% CI, 9–52; p < 0.001) and the OR per m2 increase of the BSA change was 3.68 (95% CI, 1.96–6.94; p < 0.001). In the model with BSA change alone, there was a twofold increase in risk of thyroid cancer per 1 m2 increase of this variable (OR per m2, 1.90; 95% CI, 1.05–3.43; p = 0.03).
We observed that thyroid cancer occurred earlier if BSA at age 18 was higher, in both New Caledonia and French Polynesia (Fig. 3).

Mean age at diagnosis of differentiated thyroid cancer according to BSA at age 18. SE, standard error of mean.
The results remained similar when using the formula of Mosteller (21) or the one of Dubois and Dubois (22) rather than the one of Boyd (20). In particular, BSA remained the only significant anthropometric parameter in Table 3 (results not shown).
Lastly, the results of different analyses were unchanged after taking into account colinearity by mean-centering the variables. Similar results were observed when modeling the excess of OR as a linear function of the value of these parameters.
Discussion
In this pooled analysis of two case–control studies conducted in French Polynesia and in New Caledonia, which included 554 cases of thyroid cancer and 776 control subjects, we confirmed the association between the increased risk of differentiated thyroid cancer and overweight and tallness in women, and observed a similar association in men. In a multivariate analysis, we showed that, in both sexes, increased thyroid cancer risk was more strongly related to an increased BSA, in particular at age 18, rather than to increased weight, BMI, or BF%.
This analysis has important strengths including, for both studies, the population-based design with virtually exhaustive identification of thyroid cancer cases in isolated Pacific Islands, and a high participation rate among cases and population control subjects (16,17). Another important strength is the high frequency of overweight and obesity in Pacific islands populations: 57% of our control subjects were overweight or obese, this proportion being 73% among cases before diagnosis. Indeed, in both New Caledonia and French Polynesia, changes in lifestyle and nutritional transition are currently observed, moving from the traditional diet of starchy roots, fish, and fruits to the addition of imported foods that are high in fat and low in fiber (27).
This analysis also has some limitations. Self-reported heights and weights, particularly in previous periods of life, necessarily lead to imprecise measures. Self-reporting of height generally leads to an overestimation of height (28 –31). Although self-reported weight is usually well correlated with the actual weight, it is often underestimated (31 –33). In our data, however, these problems were likely to result in nondifferential misclassification. BF% formula could seem rough; nevertheless, the error in prediction is comparable with other methods such as skinfold thickness measurements or bioelectrical impedance (19). In both territories, subjects were not measured at the waist or hips. We could not investigate another anthropometric parameter like central adiposity (waist circumference and waist/hip ratio).
Overall, the positive association that we observed between high height, weight, and BMI, and the increased risk of differentiated thyroid cancer is in accordance with other studies (10,34 –37). A few studies have shown an association between BF% and the risk of cancer such as that of breast or prostate (38,39), but none of these studies have focused on thyroid cancer. In our study, the association with anthropometric measurements was similar for thyroid microcarcinomas, which are more often fortuitously discovered than larger thyroid carcinomas. It is important for the validity of our conclusions that, in our data, this association was probably not due to the diagnostic bias that would occur if overweight men or women were more likely to be diagnosed with a thyroid cancer than normal-weight persons.
A relationship between obesity and thyroid cancer may be explained by certain metabolic consequences of excess adipose tissue. In postmenopausal women (3), this relationship could be mediated by estrogens since adipose tissue is the primary source of circulating estrogen after menopause. However, we were not able to confirm this hypothesis in our pooled analysis, because we observed similar findings in women either below or above the age of 50 years, this age being used as a proxy of their menopausal status. Also, the association with high weight and/or BMI has been found of similar magnitude in older postmenopausal women and in younger ones both in the pooled analysis of 12 case–control studies (10) and in a large Norwegian cohort (40). Other hypotheses for the explanation of this are levels of sex steroids and bioavailable insulin-like growth factor-1, as well as insulin resistance, along with a chronic inflammatory state that are associated with obesity (1,4).
The main result of our pooled analysis is that, among all of the analyzed anthropometric factors, there is a dominant association between thyroid cancer risk and BSA. BSA and BMI both have height and weight as their variable components, but the way that they are transformed in their formulas differs. For example, for a given weight of 70 kg, if height increases from 170 to 180 cm, the percent change in BSA is 2% compared to −11% in BMI, and for a given height of 170 cm, if weight increases from 70 to 80 kg, the percent change in BSA is 7% compared to 14% in BMI. BSA is a better indicator of the circulating blood volume, oxygen consumption, and basal energy expenditure than BMI or weight. For these reasons, BSA rather than BMI is used to adjust drug doses (41). When adjusting for this parameter in the present study, increased height, weight, BMI, or BF% was no longer associated with the increased risk of thyroid cancer. According to our models, two persons who had the same BSA (e.g., 1.94 m2), one measuring 1.80 m and weighing 75 kg (i.e., BMI = 23 kg/m2, normal weight) and one measuring 1.40 m and weighing 96 kg (i.e., BMI = 49 kg/m2, obesity), have the same risk of thyroid cancer. A pooled analysis of 12 case–control studies (10), which is the biggest study today about anthropometric factors and thyroid cancer, showed a major role of weight gain in excess during adulthood, but did not investigate the role of BSA. In our study, we found that BSA at age 18, that is, tallness and/or childhood obesity, was the main risk factor for thyroid carcinoma and that the rise in BSA in adulthood increased this risk only moderately.
In the present study, the association between high BSA and increased thyroid cancer risk was not influenced by sex, age at cancer diagnosis, tumor size, or parity. It was not limited to the Melanesian or the Polynesian population, and its magnitude was similar in the ethnic group defined as “other” that mainly included Europeans and Asians.
BSA, rather than height, weight, or BMI, has been shown to be the best independent predictor of the thyroid volume in both sexes (5,8). Increased thyroid cancer risk associated with higher BSA could be explained, at least partially, by a larger thyroid volume. In case of larger thyroid volume, there would be an increased number of epithelial cells in the thyroid gland. We observed an association of increased thyroid cancer risk with increased BSA, supporting the hypothesis that the larger number of thyroid epithelial cells among those with a higher BSA could increase the probability of a malignant transformation (42,43). Our finding could lead to a new investigation of the association between obesity and the risk of some cancers that affect organs whose volumes increase with BSA or BMI, such as prostate cancer. Indeed, overweight at age 18 increases the risk of prostate cancer (44) and the prostate gland volume increases with increasing body size (9).
In conclusion, we observed that a higher BSA was strongly associated with increased thyroid cancer risk after controlling for BMI and other potential confounders. This association between BSA and thyroid cancer risk underlies the association observed with the other anthropometric parameters such as height, weight, and BMI evidenced in our pooled analysis and in other studies (2,10,34 –37). Further studies are needed on the role of BSA. However, obtaining a sufficient number of subjects for such studies may be difficult. It is notable that this association of thyroid cancer with BSA was stronger at age 18. Because a higher BSA is related to a larger thyroid gland volume and increased number of epithelial cells at risk for malignant transformation, the association between increased BSA and elevated thyroid cancer risk might be explained by this mechanism.
Footnotes
Acknowledgments
This study was supported by the Ligue Nationale Contre le Cancer and the Agence Nationale pour la Recherche, and the Fondation de France. The authors thank Frédérique Rachédi, Joseph Sebbag, Jean-Louis Boissin, Larrys Shan, Joseph Teuri, John Paoaafaite, Vaiana Chungue, Laure Yen Kai Sun, Frédérique Bost-Bezeaud, Patrice Petitdidier, and Carole Rubino for the study in French Polynesia, and Michèle Reynier, Dominique Baron-Dubourdieu, Yannick Rougier, Diane Cyr, Jean-Paul Grangeon, and Sylvie Barny for the study in New Caledonia.
Disclosure Statement
The authors declare that no competing financial interests exist.