
Abstract

It is very rare that metastatic thyroid cancer presents thyrotoxicosis after total thyroidectomy. Possible mechanisms of its thyrotoxicosis are as follows: (a) the presence of anti-TSH receptor antibodies complicated with Graves' disease, (b) destructive thyroiditis caused by the growing tumor, (c) the increased conversion of exogenous levothyroxine (l-T4) to T3 by the tumor tissue (1), and (d) excessive thyroid hormone synthesis in the metastatic lesions. In the case of (d), approximately 70 cases have been reported in the literature, and almost all patients histologically showed thyroid follicular carcinoma with massive metastatic lesions. In such a situation, selective treatment is required to control thyroid function and prevent tumor growth. Here, we report a patient presenting with hyperfunctioning metastases of follicular thyroid carcinoma and show that severe hyperthyroidism can be improved with repeated low-dose radioiodine therapy.
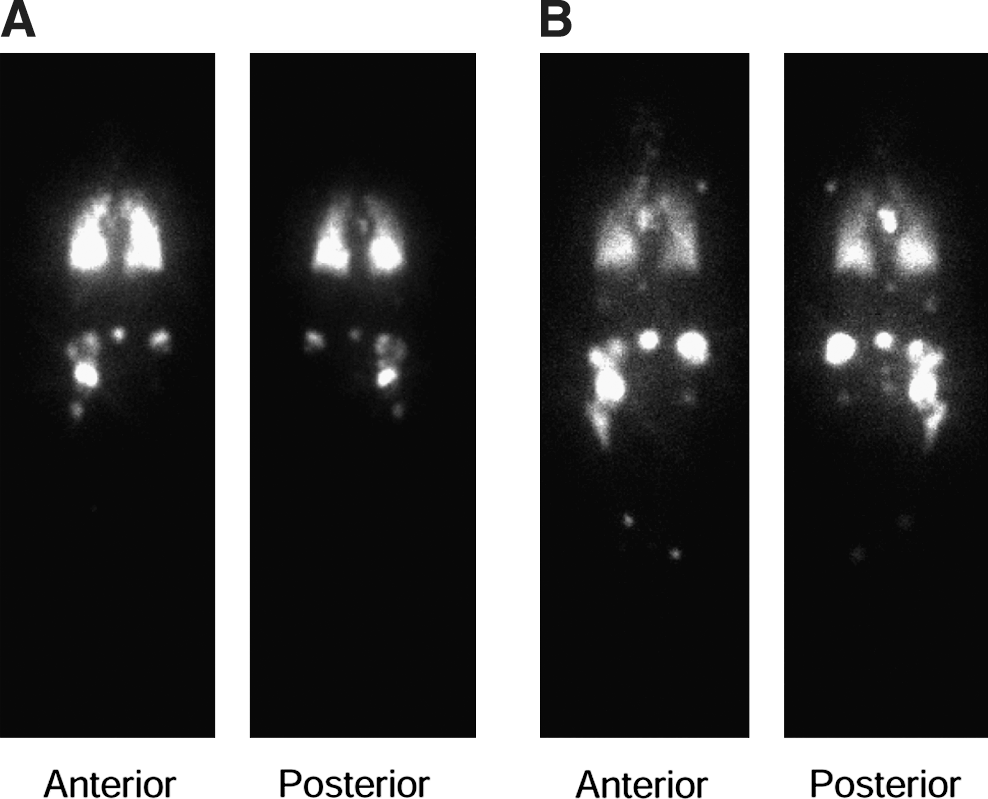
In July 2002, a 59-year-old woman developed gait disturbance due to hip pain. Positron emission tomography (PET)/computed tomography scan showed multiple mass lesions of the bones, including the humerus, rib, spine, pelvis, and femur, and in both lungs. A biopsy specimen of the rib lesion showed thyroid follicular carcinoma, and subsequently, total thyroidectomy was performed. Although the administration of therapeutic-dose radioiodine was desirable, it was impossible because of disability of living during hospitalization associated with gait disturbance. External radiation therapy was repeatedly carried out for multiple bone metastases thereafter. Thyroid function tests were normal (FT4: 1.2 ng/dL, TSH: 1.6 mIU/L) before surgery, and l-T4 replacement (100 μg daily) was started after total thyroidectomy. The withdrawal of l-T4 replacement for 2 weeks led to no elevation of thyroid hormone (FT4: 0.7 ng/dL, TSH: 3.8 mIU/L) in January 2005, but clinical features related to hyperthyroidism, including palpitation and tremor, developed in 2007. L-T4 replacement was tapered and stopped in March 2008. In September 2008, she visited our hospital for further examination. Thyroid function tests showed severe hyperthyroidism, but anti-TSH receptors were negative (Table 1). The serum thyroglobulin concentration was more than 8000 ng/mL. A 131I whole-body scan performed 72 hours after the administration of 13 mCi confirmed the low thyroid bed uptake of radioiodine, but demonstrated multiple foci of intense uptake in the bone lesions mentioned earlier and both lungs (Fig. 1A). Thereafter, additional radioiodine therapy with 13 mCi was given five times at intervals of 1–2 months (Table 1). The symptoms of hyperthyroidism gradually resolved, and her thyroid function markedly improved (FT4: 0.22 ng/dL, FT3: 5.94 pg/mL, TSH: <0.01 mIU/L), whereas the high thyroglobulin levels remained unchanged, after 10 months of initial radioiodine therapy. The 131I whole-body scan showed a moderate reduction of the lung metastases, but uptake in the multiple bone metastases relatively increased (Fig. 1B).
(
RI, radioiodine (131I); WBS, 131I whole-body scan.
Arrow (↑) indicates administration of 13 mCi.
In this patient, severe hyperthyroidism developed 5 years after confirming multiple metastases of follicular thyroid carcinoma, with high-level radioiodine uptake by metastatic lesions, but the absence of TSH receptor antibodies or low-level uptake in the thyroid bed, suggesting hyperfunctioning metastases. Appropriate treatment of severe hyperthyroidism is critical for the survival of such patients (2). For initial management to control thyroid function, it is recommended to administer antithyroid drugs and reduce the metastatic volume with some adjunctive therapies after total thyroidectomy (2,3). Radical treatment for hyperthyroidism and tumor growth is followed by maximum administration of therapeutic-dose radioiodine within safe limits to avoid radiation-induced pulmonary fibrosis. In our patient, external radiation therapy against bone metastases had no preventive effect on hyperthyroidism. Alternatively, we applied the fractionated administration of low-dose radioiodine and successfully controlled the thyroid function without antithyroid drugs. The sequential findings of a reduced uptake in the lungs but remaining accumulation in massive bone lesions by 131I whole-body scan suggest that some cell population in lung metastases is relevant for hyperfunctioning state and is sensitive to radioiodine therapy.
Survivors among cases with hyperfunctioning metastases showed a significant reduction of thyroid hormone levels after administration of therapeutic-dose radioiodine, whereas those who died showed little or no reduction (4). The fractionated administration of low-dose radioiodine may be one effective treatment to prevent lethal events, particularly for patients who are unable to receive high-dose radioiodine or must discontinue antithyroid drugs because of side effects.