
Abstract
Background:
Ultrasonography (US) is increasingly being employed by endocrinologists and surgeons in the diagnosis and management of patients with thyroid nodules and thyroid cancer. Recent consensus guidelines from the American Thyroid Association highlight the importance of this modality by recommending that patients with thyroid nodules should undergo further evaluation with cervical US to stratify the risk of malignancy. Likewise, ultrasound is advocated for the preoperative and postoperative diagnosis of cervical lymph node metastases.
Summary:
This article will summarize the US characteristics that impart a suspicious appearance on thyroid nodules and cervical lymph nodes as well as those findings that are reassuring. Likewise, the indications for thyroid nodule and lymph node fine-needle aspiration will be reviewed. Finally, this article will briefly discuss adjunctive tools in US such as elastography, percutaneous ethanol ablation, and radiofrequency ablation.
Conclusions:
US may be used to help stratify the risk of malignancy in thyroid nodules and cervical lymph nodes. This tool further aids in the diagnosis of malignancy when used in conjunction with fine-needle aspiration. US plays an important role as both a diagnostic and therapeutic tool in the evaluation of patients with neck masses.
Introduction
US, an ideal imaging modality of the neck, can be easily performed in an outpatient clinic setting. In contrast to computed tomography (CT) and magnetic resonance imaging (MRI), US is a real-time test; static images are easily obtained, but the cine capability is where the true power of US lies. These dynamic images and the ability to view the neck in multiple planes by US allows for better visualization of anatomic relationships and subtle but important changes in morphology that would be missed with CT or MRI. Improved technology with high-frequency probes allows for resolution of structures to less than a millimeter in size. In addition to superior resolution, US is very affordable ($400) compared with CT ($800) or MRI ($1200). As a result, US has become the preferred imaging modality for evaluation of thyroid nodules and detection of recurrent disease in thyroid cancer patients. This article will outline the indications for use of US in patients with thyroid nodules and thyroid cancer. In addition, the US characteristics that impart a suspicious appearance to lesions will be reviewed. Finally, adjunctive tools to US, such as elastography and fine-needle aspiration (FNA), will also be examined.
Thyroid Nodules
US has greatly improved the sensitivity of detection of thyroid nodules. By palpation alone, the prevalence of thyroid nodules in the general population is ∼5% (11). Examination with US, however, reveals that thyroid nodules increase linearly with age, such that 10% of 25-year olds have them with the rate escalating to involve nearly 55% of women over the age of 70 (11). Historically, only 5% of nodules were malignant (12). Currently, however, the rate of malignancy may be as high as 14.9%, based on results of a study from one large center examining over 3400 thyroid nodules (13). One possible explanation for this rise is the application of US-guided FNA which allows for the sampling of previously nonpalpable nodules that may have otherwise never come to clinical attention (13). Because thyroid nodules are so prevalent in the general population and the minority are malignant, a method of distinguishing those that require additional diagnostic evaluation is critical to improve resource utilization. US may be used to further characterize thyroid nodules, providing an assessment of risk of malignancy and thereby narrowing down those nodules which require FNA. In fact, it is now recommended that all patients with a suspected thyroid nodule undergo US. It is also beneficial to perform a lateral neck US to identify any suspicious lymphadenopathy (LAD). Identification of a suspicious lymph node (LN) changes the pretest probability of malignancy in the nodule; FNA cytology may be obtained from the suspicious node in lieu of the nodule (14).
Numerous studies have investigated the sonographic features of nodules as predictors of malignancy (15 –21) (Table 1). Although independently not sufficient to diagnose or exclude malignancy, the presence or absence of these characteristics aids the clinician in deciding which nodules to biopsy. The sensitivity and specificity of each individual characteristic is variable from study to study, owing to high interobserver variability and differing techniques to diagnose malignancy (22 –24). No single US finding meets the ideal of a high sensitivity and a high positive predictive value for diagnosing thyroid cancer. The presence of multiple criteria, however, increases the specificity for malignancy (25) but does so at the cost of sensitivity.
US, ultrasonography.
Larger nodules are not more likely to harbor malignancy than smaller ones (25,26). Nonetheless, recent consensus guidelines suggest that only nodules over 1 cm should undergo routine fine needle aspiration (FNA) (American Thyroid Association [ATA] guidelines). This 1 cm cutoff has been chosen because it is thought that clinically significant cancers may be present in nodules above this size (14). However, subcentimeter nodules may also require further workup. For example, patients with a high risk history and a 5–8-mm nodule that has suspicious sonographic features also warrant FNA (14) (Table 2). A high risk history includes patients who have a family history of thyroid cancer, personal history of ionizing or external radiation exposure in childhood, prior history of hemithyroidectomy with discovery of thyroid cancer, or 18-fluorodeoxyglucose positron emission tomography (18FDG-PET) positive nodules. The ATA has defined suspicious sonographic findings as those nodules with microcalcifications, increased nodular vascularity, hypoechogenicity, and irregular, infiltrative margins (14) (Table 2).
A, strongly recommended based on good evidence; B, recommended based on fair evidence; C, recommended based on expert opinion.
Suspicious sonographic features are irregular and infiltrative borders, microcalcifications, increased intranodular vascularity, and hypoechogenicity.
A high-risk patient is one with a personal history of ionizing or external radiation during childhood, family history of thyroid cancer, prior hemithyroidectomy with discovery of thyroid cancer, FDG avidity on PET scan, calcitonin >100, or multiple endocrine neoplasia 2 (MEN2)/familial medullary thyroid carcinoma (FMTC)-associated rearranged during transfection (RET) proto-oncogene mutation.
FNA, fine-needle aspiration.
Patients with multiple nodules have the same likelihood of malignancy (∼14%) as those patients with a solitary nodule (25,26), a finding which contradicts traditional teaching that the risk of malignancy decreases with increasing numbers of nodules (27,28). It is currently recommended that US-guided FNA be performed on up to four nodules, preferentially sampling those with the most suspicious findings on US (14).
Calcifications in a thyroid nodule are the most reproducible ultrasonographic findings (29). Such deposits may appear as punctate echogenic foci (microcalcifications), a fine rim of calcium (eggshell calcification), or a coarse aggregate of calcification (macrocalcification). The presence of any type of calcification increases the likelihood of malignancy by two- to threefold (18), but coarse calcifications have also been correlated with long-standing benign nodules and Hashimoto's disease (30 –32). It is felt that these coarse deposits represent tissue degeneration and fibrosis (32). Likewise, eggshell calcifications may be seen in benign nodules; one study found that 37% of patients with eggshell calcifications had a benign nodule (33). Microcalcifications in a solid nodule, on the other hand, are more specific for papillary thyroid carcinoma (PTC) and likely represent psammoma bodies (infarcted papillae) (32). These punctate calcifications should not be confused with the comet-tail sign seen in cystic and colloid nodules; the latter are distinguished by the posterior acoustic enhancement seen with subtle movement of the US probe (34). The comet-tail sign is thought to be an artifact caused by ultrasound wave reverberations from contact with colloid crystals, and such a finding has a >85% chance of being benign (see Fig. 1) (32,34). Unfortunately, relatively few thyroid nodules have calcifications (∼30%) (26) and so their absence does not rule out malignancy; additional diagnostic investigation is necessary.
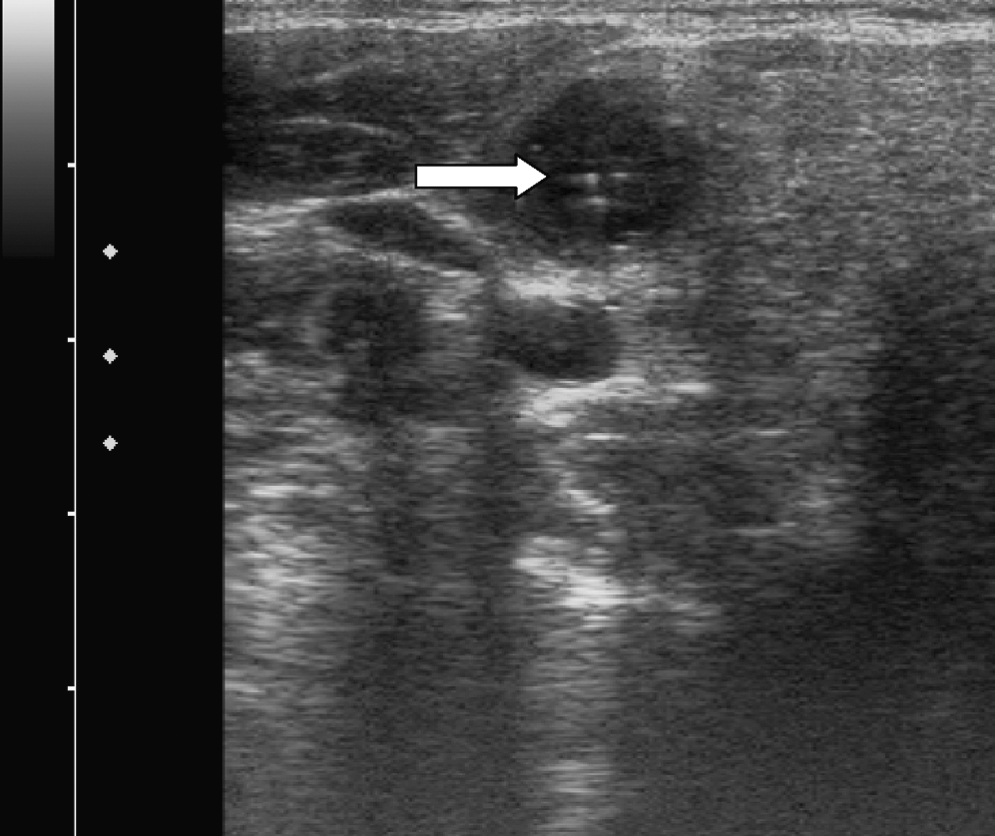
Comet-tail sign in a colloid nodule (arrow).
The pattern of vascular flow has been used by some as an additional tool to identify suspicious thyroid nodules (15,26,35). Such studies have found that a pattern of increased Doppler flow throughout the nodule is associated with a higher risk of malignancy. As seen in Table 1, the range of sensitivity and specificity for this test is very broad, likely owing to high interobserver variability. Gain settings on the Doppler flow can be changed such that any nodule can appear highly vascular, further minimizing the utility of this particular test.
The shape of a nodule may also be considered when estimating its risk of malignancy (16,18,36). Height greater than width when imaging a nodule in the transverse direction has been correlated with increased risk of malignancy (16,18,36). The natural growth planes—horizontal in a supine patient—correspond to the width of the nodule; growth across that plane, with increased nodular height, suggests a more aggressive tumor (37). However, the sensitivity and specificity of this finding are variable, and larger studies are needed to further validate this characteristic.
Certain US findings can be reassuring to clinicians when evaluating a thyroid nodule. A “honeycomb” or “spongiform” appearance, multiple tiny cystic structures separated by thin septations in more than 50% of the nodule, is highly specific for benignity (18,32,38). Consequently, spongiform nodules ≤2 cm may be followed with serial US rather than performing an FNA (14) (Table 3). Another reassuring US feature is cystic content; several studies have found that there is an inverse relationship between the cystic content of a nodule and the risk of malignancy (25,38). In fact, simple cysts (no solid component) that are less than 2 cm in largest diameter do not require FNA for diagnostic purposes but may be performed to relieve compressive symptoms. Although finding a purely cystic nodule is highly specific for benignity, it has a very low sensitivity, as less than 1–2% of nodules meet this criterion (25). Finally, the presence of a solitary or multiple <1-cm cysts is likely the result of benign nodular hyperplasia (38). These nodules may have a central comet-tail sign, which is typically an indication of abundant colloid within the cyst (38).
Quantifying the risk of malignancy in an individual nodule based on the overall sonographic appearance can be challenging, even in the hands of an experienced sonographer. A recent study (39), however, utilized 12 nodule features on US to calculate a numerical risk of malignancy for any given nodule. In this study, a mathematical equation was created from a retrospective logistic regression analysis of US findings in over 1600 patients who had undergone US-guided FNA biopsy. This equation predicted the probability of malignancy based on US findings and developed categories ranging from lowest to highest likelihood of malignancy. The US features used to develop the equation included the presence of a goiter, size of the nodule, height greater than width, nodule margins, echogenicity, echotexture, nodule composition (cystic vs. solid), presence of calcifications, and presence of suspicious lymphadenopathy. Although the results have not been prospectively verified, tools such as this equation may help guide clinicians to determine which nodules require further intervention with FNA and which nodules may be simply followed with repeat US.
Another new diagnostic tool to predict the risk of malignancy in an individual nodule is ultrasound elastography (40 –42). This technique provides a measure of tissue stiffness by applying a standardized external force and calculating the degree of distortion of the US beam (41). Based on the principle that a firm nodule by palpation has a higher likelihood of malignancy, elastography is a more objective way to assess nodule consistency. It should be noted that this technique cannot be used on nodules whose contents are >20% cystic, those with coarse calcifications, nodules less than 8 mm, or coalescent nodules (41). Likewise, ultrasound elastography is limited by the need for specialized equipment, is time consuming, and is labor intensive (43). However, a newer derivation of this technique—the combined autocorrelation method—has circumvented time constraints and maintains a high level of sensitivity (97%) and specificity (100%) for detecting malignancy (41). These highly favorable findings should be observed with caution, though, as the number of patients included was small and bias may have been introduced by only including patients who were scheduled for surgery in the analysis. Additional prospective studies are needed to confirm these results.
Follow-Up of Benign Nodules
Thyroid nodules determined to be benign by cytology should be followed with repeat examination because the risk of a false-negative FNA may be as high as 4% (44) and even higher in nodules over 4 cm (45). US is the recommended modality for serial follow-up because palpation is not as sensitive for detecting changes in size of nodules and because not all nodules are palpable (46). A repeat US examination at 6–18 months after FNA should be performed to detect significant changes in nodule size (14). Although not all nodules that grow are malignant, it is an indication for a repeat FNA (47). Significant change in size of a nodule is defined as a greater than 20% increase in at least two nodule dimensions of solid nodules with a minimal increase of 2 mm (14). Such repeat measurements of thyroid nodules over time are complicated by high interobserver variability. In fact, one careful study revealed that the minimal change in nodule volume that could be reproducibly measured was 49% (22). For this reason, the ATA guidelines also recommend a repeat FNA of nodules with a greater than 49% change in volume (14). If a nodule has not grown more than the above stated criteria, the interval before the next US follow-up may be extended to 3–5 years (14).
Lymph Nodes
Lymph node metastases are present in the majority of thyroid cancer patients. In fact, with measurement of the thyrotropin receptor and thyroglobulin (Tg) by polymerase chain reaction amplification of FNA washouts, nearly 90% of patients had microscopic metastases in one study (48). By imaging, however, 20–50% of patients are found to have lymph node metastases (49,50). It is these nodes which are ultrasonographically detectable that are of greater clinical importance to the patient; one study showed that patients with nodes found on US before surgery had a worse relapse-free survival than patients with microscopic metastases found during prophylactic surgery (51). The ATA currently recommends routine neck US to screen for lymph node metastases in patients awaiting thyroidectomy for a diagnosis of thyroid cancer (14). This is an important component of the initial workup for two reasons. First, the findings on these sonograms alter the surgical approach in up to 40% of patients (52). And second, repeat operations may be avoided for recurrent/persistent disease at a later date (53).
The overall sensitivity and specificity of US for detecting LN metastases is difficult to evaluate unless routine prophylactic neck dissections are performed; the few available studies have widely variable rates (Table 3) (52,54 –56). Benign lymph nodes may not be visualized by US, but are more readily identified when they are enlarged and reactive (57). The typical appearance of a reactive node is distinctive based on the fusiform (oval) shape and presence of a hyperechogenic stripe (hilum) along the center (32). The hilar stripe is indicative of intranodal fatty tissue and entry of vasculature into the healthy node and the lymphatic outflow from the node (32). Neoplastic infiltration typically occurs initially within the outer cortex of the node, where the lymphatics feed the node; as a result, disappearance of the hilum may be the earliest indication of malignant transformation of a lymph node (32). Further, this peripheral infiltration of the node leads to a conversion in the shape of the node from oval to a rounded appearance (57,58). Both of these characteristics—the absence of the hilum and the shape of the lymph node—are useful indices to gauge whether a node is malignant by US (57,58) (Table 3). It should be noted, however, that a benign node may appear suspicious when only viewed in the transverse view, depending on the node's orientation in relation to the probe. As such, it is important to visualize nodes in both the transverse and longitudinal (sagittal) views to determine if there is lengthening of the node and whether a hilar stripe is present.
An objective way to assess the roundness of a lymph node is the Solbiati index (SI)—the long-to-short axis ratio (32). A ratio of greater than 2.0 is indicative of a benign node with an oval shape; less than 2 is consistent with a rounded, malignant node (32,57 –59). The sensitivity and specificity of the SI is widely variable across studies (Table 3), but it can be a very useful indicator in conjunction with other US characteristics (32,58,60,61). A derivation of this index is the shortest diameter cutoff; malignant nodes are more likely to measure >0.5 cm (58). Although not very sensitive (61%), the short axis >0.5 cm is very specific (96%) for malignancy (58). In contrast, the maximum diameter of a lymph node is generally not a helpful indicator of malignancy by itself (57,59). Traditional teaching dictates that nodes over 1 cm in greatest length are suspicious for malignancy, but reactive nodes are frequently seen to exceed this length (32,57,59). Reactive nodes typically maintain their fusiform shape, and therefore, the SI is helpful to distinguish enlarged, reactive nodes from malignant ones (57).
Benign reactive lymph nodes are usually hypoechoic (of similar echogenicity to surrounding musculature). Metastatic nodes with PTC, on the other hand, may be heterogeneous in echotexture or hyperechoic. The hyperechogenicity results from colloid deposition and malignant infiltration of the node (62). Heterogeneity may occur because of cystic portions within the node and/or calcifications. A cystic lymph node is highly specific for malignancy (Table 3) (32,58,60,63,64). More frequently seen in young adults and children, cystic degeneration is felt to be the result of more aggressive tumors with extensive liquefaction necrosis and colloid production (64). Calcifications in a lymph node are also highly specific for thyroid cancer; they may be seen with PTC and medullary thyroid carcinoma (58,60). In patients with PTC the calcifications are peripherally located, punctate hyperechogenicities and are thought to represent psammoma bodies (58,60). Calcifications in nodes of metastatic medullary thyroid carcinoma are less commonly seen, but have been described as peripherally located and coarse (65). These hyperechogenic foci are formed from calcium deposits surrounded by amyloid (65).
Another US characteristic which may help identify malignant nodes is the pattern of vascular flow. Typically, blood flows into the central hilum in benign nodes (66). As the node becomes infiltrated with malignant cells, the organized flow into the hilum is disrupted (66). Neovascularization results in chaotic flow throughout the node and into the periphery, along the capsule (59,66). Visualization of this atypical flow by color Doppler or power Doppler allows for identification of suspicious nodes to select for FNA (59). Power Doppler is more sensitive than color Doppler (67); this difference may account for some of the variability across studies when reporting the sensitivity and specificity of vascularity in diagnosing malignancy (58,60,68 –71).
The location of lymph nodes is also an important consideration when attempting to identify malignancy. The most widely accepted terminology for describing node location is based on easily recognizable anatomical landmarks (see Fig. 2). The central neck is the region most frequently involved with malignancy (level VI) (72). However, preoperative US misses nearly 50% of malignant nodes in this area because the thyroid obscures adequate visualization (73). On routine prophylactic central neck dissection, 30–40% of patients have malignant nodes (72,74). With removal of the thyroid, sensitivity of imaging the central neck improves significantly (60) and this becomes a critical area in the surveillance for recurrent thyroid cancer (14). Thyroid cancer involves levels III and IV on the side ipsilateral to the primary tumor nearly as often as the incidence of central neck metastases (72). Although thyroid cancer may spread to level II, it occurs much less frequently than the lower lateral and central neck (72). Instead, nodes in the submandibular region are more likely to be enlarged and reactive appearing. This is because the mouth has repeated microtraumas and subsequent enhanced inflammatory activity (57). Level V is only rarely involved with malignancy in PTC, typically in patients with extensive nodal metastases (72). Such patients are also at risk for mediastinal and hilar nodal involvement (72). For those with unilateral tumors, it is unusual (9–14%) to identify malignant nodes in the opposite lateral neck (72).
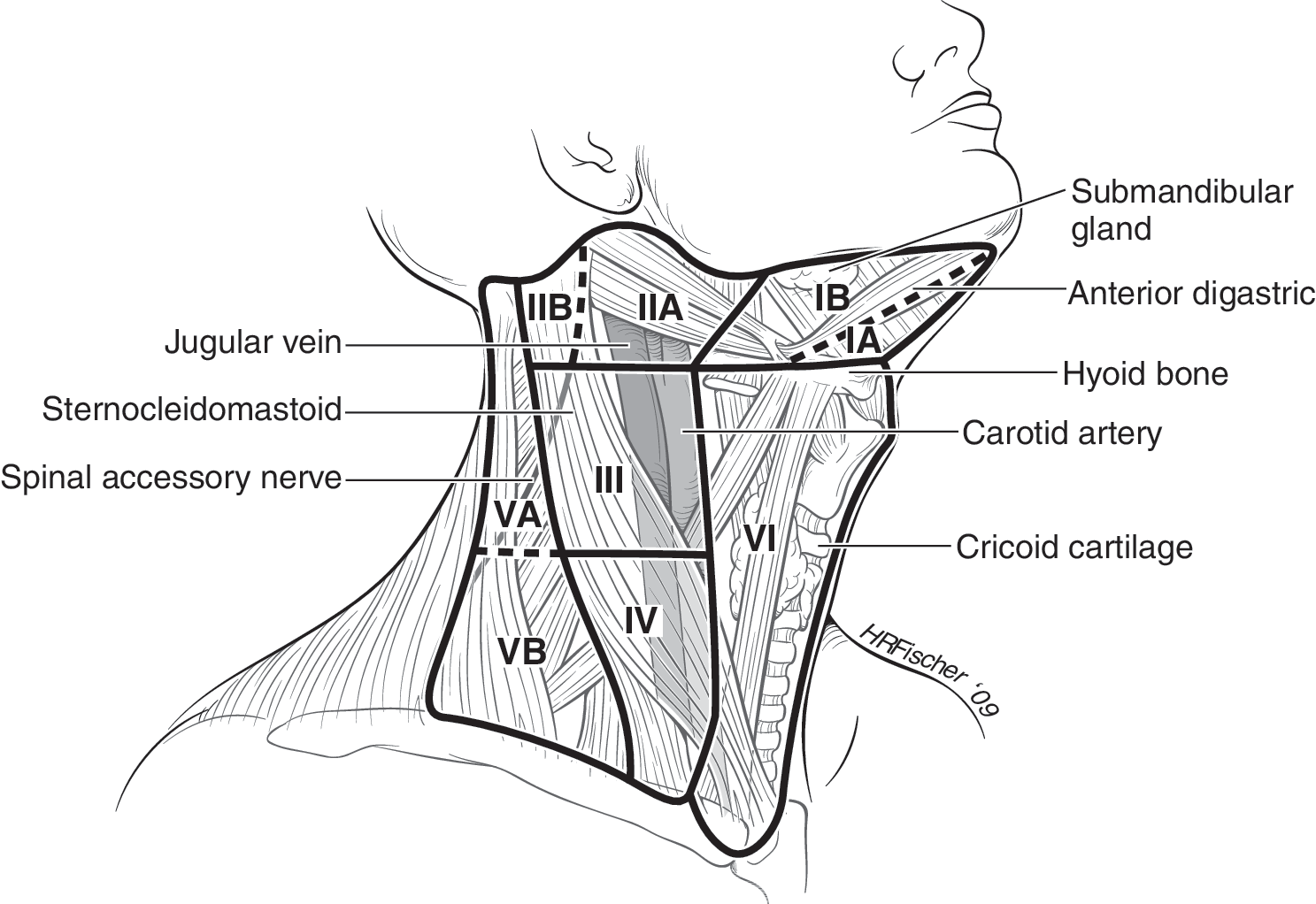
Lymph node compartments of the neck [reproduced from Cooper et al. (14) with permission].
Ultrasound elastography has also been evaluated for its ability to identify malignant lymph nodes (54,75). In a similar protocol that is employed for thyroid nodule investigation (see above), the US probe is used to compress the lymph node. The measure of tissue distortion is compared with the adjacent musculature (54,75); malignant nodes produce greater strain than the surrounding tissues. Although the technique is in the preliminary stages of investigation, two trials have shown promising results with sensitivity of 83–85% and specificity of 98–100% (54,75).
Thyroid Cancer Surveillance
Historically, surveillance for recurrent or persistent differentiated thyroid carcinoma included measurement of serum Tg and diagnostic whole body scans (DxWBS) (14). Careful study has revealed, however, that the DxWBS by itself has a very poor sensitivity (21%) (76). Instead, serum Tg in combination with a thorough cervical US has the highest sensitivity (96.3%) and negative predictive value (99.5%) of the available tests for detecting recurrent disease in low-risk patients (76). As a result, it is currently recommended that patients with low-risk differentiated thyroid cancer undergo US monitoring at 6–12 months after surgery and then periodically, depending on the patient's risk for recurrent disease and Tg status (14). In addition, serum Tg should be measured every 6–12 months at the same laboratory (14). Further, DxWBS does not need to be performed in low-risk patients with undetectable Tg, negative Tg antibodies, and negative US (14).
When suspicious LNs are identified by US, consensus guidelines recommend that FNA be performed under US guidance for lesions greater than 5–8 mm in the smallest diameter, if a positive result would change the management of the patient (14). Lymph nodes less than 5–8 mm in the largest diameter may be followed without biopsy, with the intention of intervention if there is lesion growth or impingement on vital structures.
False Positives on US
The ultrasonographer should be aware of other findings on US which can be mistakenly identified as recurrent thyroid cancer. In the postoperative thyroid bed, the esophagus becomes more visible. Characteristically found on the left immediately adjacent to the trachea, this structure can be easily recognized by asking the patient to swallow. Visualization of the bright white flash of air as it moves through the esophagus is the confirmatory, real-time test. A related finding which may be confused for recurrent PTC or a thyroid nodule in patients whose thyroid remains intact is a pharyngoesophageal diverticulum (77). A diverticulum should be suspected if the mass is mobile with swallowing or appears to be contiguous with the esophagus in the longitudinal (sagittal) view (77). Punctuate hyperlucencies within the mass may appear similar to calcifications or even have a comet-tail sign, but these are actually pockets of air within the diverticulum (77).
Other findings on US which may mimic a malignant lymph node include parathyroid adenoma (78), postoperative granuloma (79), and postoperative neuroma (80). A parathyroid adenoma may be seen anywhere along the carotid or in the superior mediastinum, but is usually seen in the thyroid bed. These hypoechoic masses are distinguished by their intense vascularity and the presence of a feeding artery at one end of the adenoma (81). Granulomas appear in response to sutures and other foreign bodies in the operative field and may be seen in the thyroid bed or in the lateral neck (79). Their appearance is generally that of a hypoechoic, ill-defined lesion with a central echogenic focus, which represents the suture or staple (79). Neuromas have a similar manifestation to granulomas and reactive lymph nodes, in that they are hypoechoic, solid, fusiform masses with a central hyperechoic area (80). They differ, however, because neuromas are typically superficial and palpable and may be painful (80). Also, neuromas are usually located along the second cervical nerve, posterior and lateral to the carotid artery (80). Unlike reactive lymph nodes, granulomas and neuromas are relatively avascular (79,80).
When imaging the upper mediastinum, thymus tissue may be identified, particularly in young patients. Cervical thymic tissue is quite unusual, though it has been described and should be included in the differential diagnosis of unusual neck masses (82). On US the thymus has a characteristic lacy appearance, which correlates with the fibrous septations and vasculature seen on pathologic sectioning of the tissue (82).
Ultrasound-Guided FNA
In spite of the numerous ultrasonographic findings that can alter the suspicion for malignancy, US-guided FNA remains the gold-standard for diagnostic evaluation of thyroid nodules and lymph nodes (14). Relatively easy to perform in the office, this procedure has a low risk of complications, with mild hematoma and localized pain as the most frequently encountered side effects. Performing the FNA under US guidance allows for visualization of the needle entering the nodule of interest and can direct the sampling into solid portions of complex nodules, thereby increasing the likelihood of obtaining an adequate sample (83). Likewise, US-guided FNA has a lower false negative rate when compared with the palpation-guided technique—1% versus 2.3%, respectively (83). The utility of FNA cytology is limited, however, in the presence of cystic lymph nodes; similarly, sampling error in a node with focal involvement also may lead to a false negative diagnosis (84). Measurement of Tg in the FNA washout is more sensitive and has a better negative predictive value than cytology alone (84). An additional benefit of measurement of Tg in the FNA washout is that it is not affected by the presence of Tg antibodies in the serum (85). Another exciting new extension of FNA is molecular testing of the aspirates to aid in the diagnosis of malignancy. Indeed, identification of gene mutations and measuring expression of cancer-associated mRNAs and microRNAs on FNA samples have been reported to improve the accuracy of FNA, and therefore have potential to reduce the number of surgeries performed for diagnostic purposes (86,87).
Percutaneous Ethanol Injection
Patients with recurrent disease in the neck who are not amenable to repeat treatment with radioiodine, surgery, or external beam radiotherapy may be candidates for percutaneous ethanol injection (PEI) (88,89). By injecting 95% ethanol under US guidance, this procedure causes ischemic necrosis and subsequent reduction of tumor volume (88). Although there is only limited follow-up and no data regarding the effect on survival in patients with PTC, preliminary results indicate that PEI can control limited disease burden (1–5 lymph nodes) (88,89). Although results are variable, up to a third of lymph nodes disappeared (89) and the mean reduction in tumor volume was 93.6% (88). The best effects were seen after two treatments (88,89). The procedure is generally well tolerated; the most frequent side effect was minor localized pain and transient hoarseness (88,89).
Radiofrequency Ablation
Another minimally invasive alternative to surgery and radioiodine is percutaneous radiofrequency ablation (RFA). Widely employed for hepatocellular carcinoma and liver metastases from other malignancies, RFA is being investigated for its effects on locoregional and distant metastases in differentiated thyroid cancer (90). Utilizing US guidance, the electrode tip is inserted into the lymph node and the current induces focal coagulative necrosis to destroy tissue up to 1 cm in diameter (90). Larger areas require multiple treatments (90). Local disease was controlled in 14 of 16 patients treated in one study; however, the effect of RFA on long-term survival is unknown (91). All of the patients experienced neck swelling and discomfort for 1–2 weeks after the treatment and one patient developed a vocal cord palsy (91).
Summary
US has assumed an essential role in the diagnosis of thyroid cancer, beginning with identification of suspicious nodules and lymph nodes to performing US-guided FNA. Recognition of its improved sensitivity and specificity over the traditional method of surveillance—diagnostic 131I scanning—has resulted in the acceptance of US as the standard of care for follow-up of patients with low-risk differentiated thyroid cancer (14). US may prove an invaluable resource for some patients with a small burden of recurrent disease that is not amenable to the traditional treatment protocols through utilization of PEI or RFA. Overall, its ease of use, high accuracy, and relatively inexpensive cost make US ideal for the development of additional applications for use in the management and diagnosis of thyroid cancer.
Footnotes
Disclosure statement
The author declares that no conflicts of interest exist.