
Abstract

The discovery of TRH confirmed the hypothesis proposed by Geoffrey Wingfield Harris (1913–1971) in the late 1940s that the anterior pituitary gland of mammals is regulated by factors secreted by hypothalamic neurons into the hypothalamo-hypophysial portal circulation (3). Guillemin's and Shally's groups labored for many years prior to 1969, making highly purified hypothalamic extracts from the pooled tissues of hundreds of thousands to millions of sheep and pig brains, and demonstrating that they contained “releasing activity” not only for TSH, but also for other anterior pituitary hormones. The discovery of the structure of TRH was a breakthrough, not only because of its validation of the neurohumoral hypothesis pioneered by Harris, but also because it permitted the synthesis of liberal amounts of the peptide, opening the door to novel insights into hypothalamic pituitary–thyroid (HPT) pathophysiology and extending the diagnostic armamentarium of endocrinologists.
Physicians and biologists now had a powerful tool to investigate the different levels of HPT axis control in pituitary and thyroid diseases and in various physiological states (4 –7). A procedure was developed whereby bolus intravenous administration of TRH was performed, leading to a prompt increase in plasma TSH, which peaked after 20 to 30 min and recovered to baseline at approximately 120 min. Investigations centered on this paradigm revealed the process (Fig. 1) through which thyroid function (level C) is controlled by pituitary TSH (level B), which in turn is influenced by hypothalamic TRH stimulation (level A); negative feedback is exerted at the level of both the pituitary and hypothalamus by circulating thyroid hormones. The concept that thyroid hormone has a direct effect on hypothalamic TRH production was a later development as were the studies showing the importance of TRH not only to stimulate TSH secretion, but also to enable the pituitary to produce appropriately glycosylated TSH with its full thyroid-simulating biopotency. In contrast, it was noted even before 1969 that administration of thyroid hormone blunted the thyrotroph response to TRH containing hypothalamic extracts (i.e. “direct pituitary feedback”).
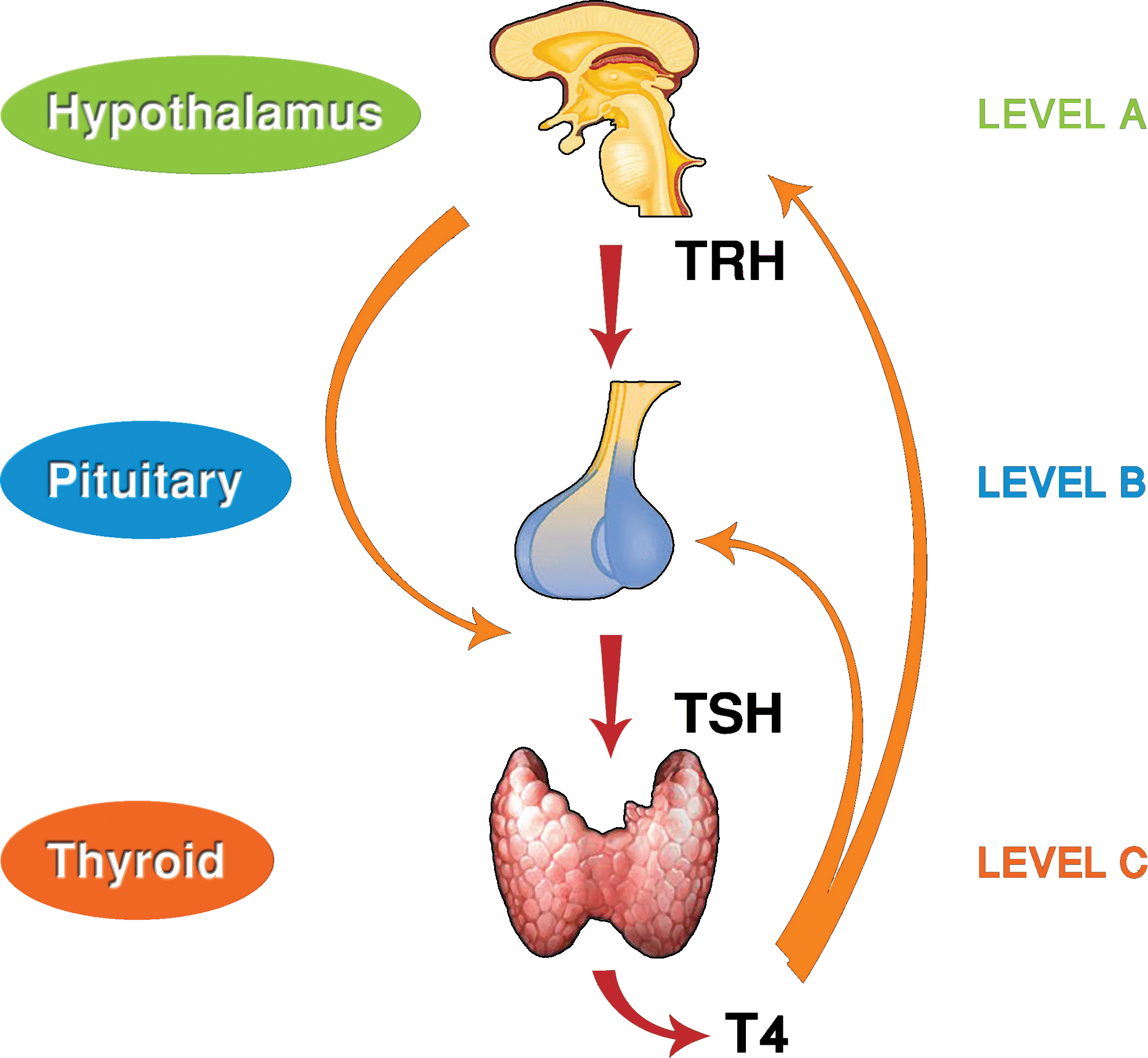
The thyrotropin-releasing hormone (TRH) test. TRH controls the secretion of thyrotropin (TSH) from the pituitary gland, which in turn stimulates the production and release of thyroid hormones, which subsequently exert a negative feedback on both pituitary and hypothalamus levels. T4, thyroxine. Color images available online at
The TRH test gave birth to a comprehensive understanding and thereby to an in-depth evaluation of the thyroid feedback mechanism, an interdependent fine-tuning process modulating the various levels of the HPT axis for stimulating the thyroid and maintaining euthyroidism. The extreme fragility of the internal equilibrium of this system, the fact that the subtlest of changes in too much or too little of the controlling variables were capable of distorting the balance puts one in mind of Heraclitus' “palintonos (counter-stretched) harmony, as in the bow and the lyre” (8).
TRH, at first the province of thyroidologists, became of interest to those working in other fields of endocrinology. The discovery that administration of the tripeptide stimulated prolactin secretion, while a blunt response was usually consistent with prolactinomas, as well as the fact that rapid increases of growth hormone secretion were noted in approximately half of patients with acromegaly, significantly amplified its actions and use in clinical medicine (9,10). Further, circulating β follicle-stimulating hormone and luteinizing hormone, and possibly the α subunits as well, increased following TRH administration in some patients with acromegaly, suggesting a plurihormonal pituitary tumor (11). While the introduction of the third- and fourth-generation assays of TSH measurement and the development of fine imaging techniques in the early 1990s have considerably restricted the use of the TRH test in the diagnosis of thyroid disease and pituitary adenomas, it nevertheless remains valid in evaluating patients with central hypothyroidism and inappropriate secretion of TSH or as an adjuvant tool in the diagnosis of some pituitary adenomas (12,13).
Notwithstanding its diminished use in clinical medicine, TRH is a prime target of modern day research. New data have emerged that have helped elucidate the mechanism by which hypothalamic-thyroid feedback is altered in patients with nonthyroidal illness (14). Research has revealed that besides orchestrating the control of pituitary–thyroid function via the hypophysial portal circulation, TRH exerts central effects on feeding behavior, thermogenesis, and autonomic regulation (15). It has also been recently reported that infection may inhibit hypophysiotropic TRH neurons via induction of local triiodothyronine production in tanycytes by enhancing type 2 iodothyronine deiodinase (D2) activity (16). Meanwhile, very recent studies have shown mutations of the TRH receptor gene to be a cause of central hypothyroidism (17 –19). Thus, even 40 years after the discovery of TRH, this pluripotent peptide continues to offer a vast and highly stimulating field of investigation with much more likely to be disclosed.
Footnotes
Disclosure Statement
The authors declare that there is no conflict of interest.