
Abstract
Background:
Struma ovarii (SO) is extremely rare, with less than 200 reported cases in the medical literature. SO is defined by the presence of an ovarian tumor containing thyroid tissue as the predominant cell type. Malignant transformation is rare and lethal cases of SO are even rarer. We report on a patient presenting with left ovarian cystic SO and lethal outcome.
Summary:
A 45-year-old woman was diagnosed with a follicular variant of papillary carcinoma on laparotomy and left salpingo-oophorectomy. She had persistently elevated serum thyroglobulin following total thyroidectomy + radioiodine and second-look surgery. Imaging scan analysis showed pelvic tumor recurrence and hypervascular liver metastases during follow-up as well as peritoneal carcinomatosis in the pelvis, right abdominal wall, and malignant ascites. The patient died from cachexia at 37 months after diagnosis.
Conclusions:
Such an aggressive malignant disease and lethal course of SO is rare. Total thyroidectomy is mandatory to exclude a primary thyroid neoplasm and for radioiodine therapy and follow-up. SO may spread to contralateral ovary, pelvic nodes, peritoneum, liver, lungs, and bones through hematogeneous spread, which is different from the dissemination pattern of papillary thyroid carcinomas. Imaging highlights the mixed behavior of this ovarian tumor.
Introduction
Patient
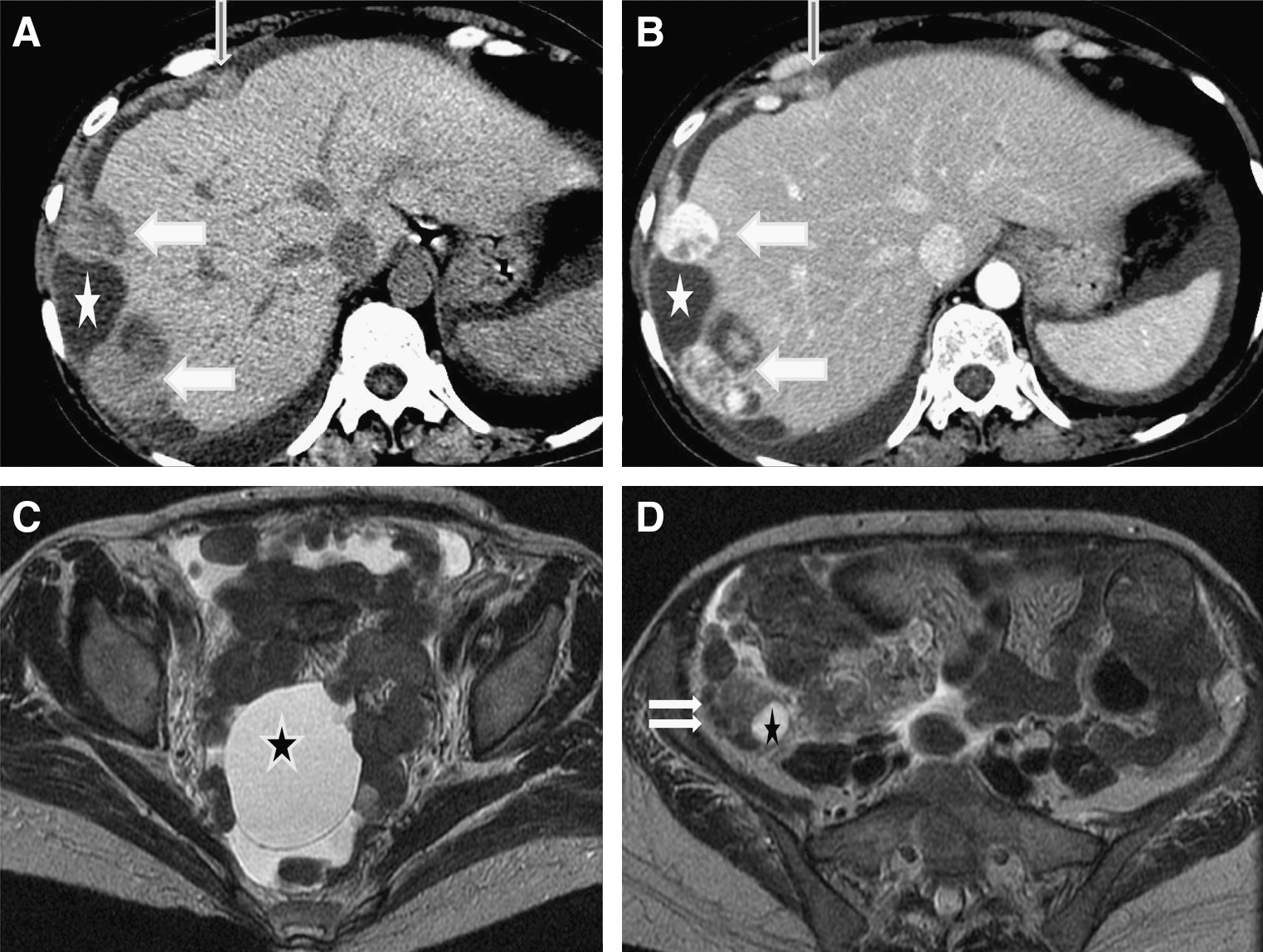
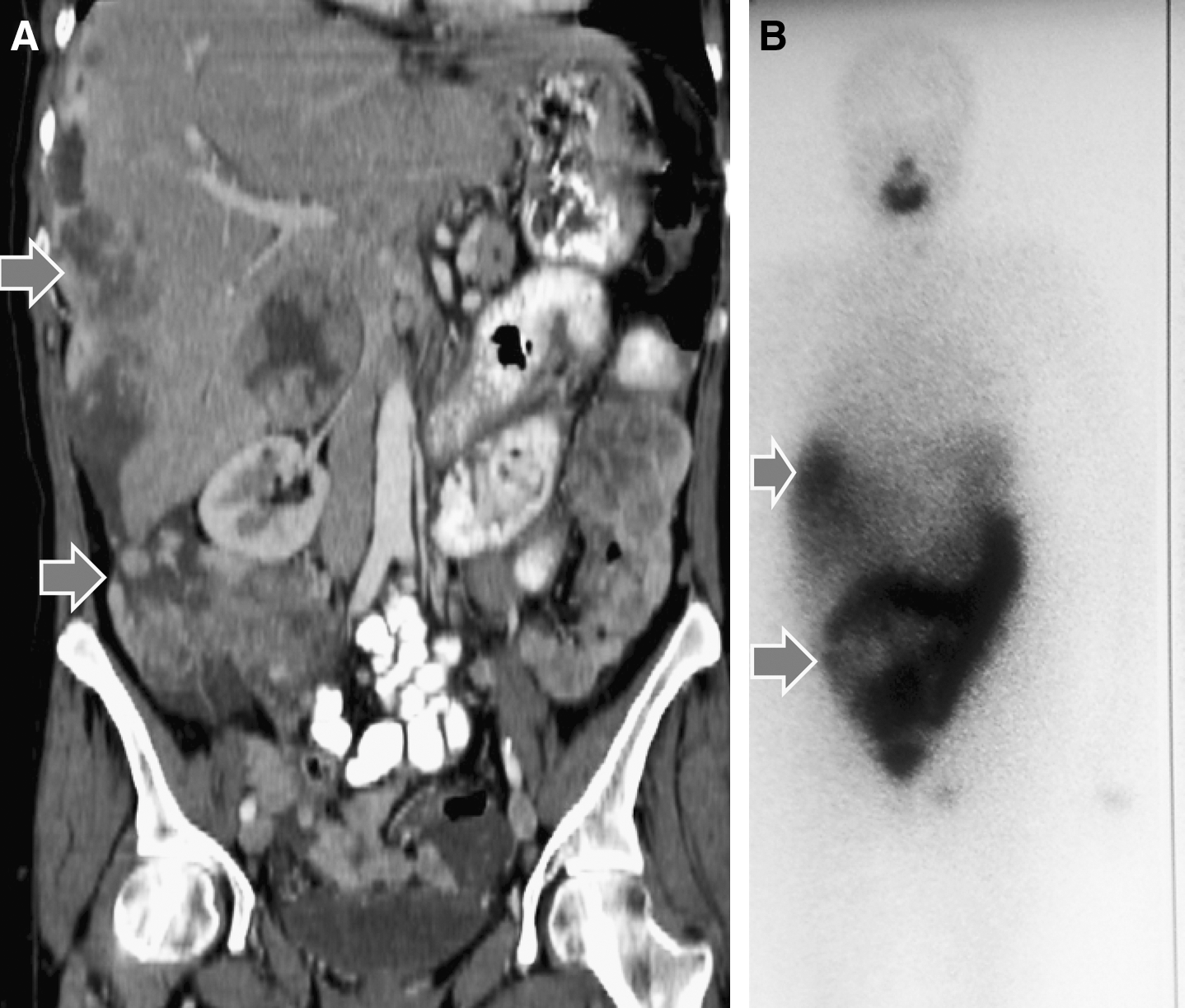
A 45-year-old woman presented with abdominal pain, anorexia, and recent weight loss of 14% of her usual weight (usual body–mass index of 24.1). The patient had a history of laparotomy and left salpingo-oophorectomy for an 11-cm ovarian cyst (Surgery 1) at 11 months earlier. Ca-125 level was within normal limits. Histology had revealed a follicular variant of papillary carcinoma in a left-sided SO. Second-look contralateral salpingo-oophorectomy, hysterectomy, omentectomy, retroperitoneal lymph node excision, and peritoneal cytology (Surgery 2) were negative for malignancy. Subsequent total thyroidectomy was delayed because the patient had been refusing thyroidectomy for 1 year. Histology of the thyroid ruled out primary malignancy. Postthyroidectomy serum thyroglobulin (Tg) was elevated (407 μg/mL; thyroid stimulating hormone (TSH)<0.03 mUI/L) but the patient had not regularly taken her suppressive hormonal therapy. At case presentation, computed tomography (CT) and magnetic resonance imaging (MRI) scan analysis showed a hypervascular and necrotic hepatic nodule (VI–VII liver segments) and a left pelvic mass. Subsequent laparoscopy (Surgery 3) revealed multiple nodules of peritoneal carcinomatosis in the pelvis, right abdominal wall, and malignant ascites with biopsy-proven metastases of the liver and pelvis (Fig. 1); serum Tg level was increased to 2,445 080 mg/ml. 131I whole-body scan (WBS) showed limited uptake in the neck and multifocal uptake in the abdomen (right liver) and pelvis. The WBS was followed by radioiodine therapy (131I, 7.4 GBq/200 mCi) and a further WBS disclosed iodine avidity, disappearance of bone metastases, and global stabilization of liver lesions. The patient underwent four courses of chemotherapy (cisplatin, doxorubicin) and two other therapeutic radioactive 131I infusions over a period of 27 months (5.4 GBq/147 mCi and 6 GBq/162 mCi). Serum Tg level doubled within 3 months at postchemotherapy control, CT/MRI showed tumor progression, and WBS still showed iodine hyperavidity. Despite the therapy, the patient developed locoregional disease progression (Fig. 2) and lung, adrenal, and bone metastases. The patient died from cachexia (body–mass index of 15.9) at 37 months after diagnosis.
(
(
Discussion
SO was first described by Von Kalden in 1895 (1). In a series of 1390 ovarian tumors, 12% were identified as teratomas and only 0.4% as SO (1,2). SO most commonly occurs in the fifth and sixth decades of life. The histological diagnosis relies on a monodermal ovarian teratoma, which contains more than 50% of mature thyroid tissue with large follicles containing abundant colloid. The diagnosis is often made incidentally on abdominal/pelvic ultrasound or during surgery. Focal increased pelvic uptake on WBS or elevated serum Tg have been reported during follow-up of differentiated thyroid cancer (2,3). Occasionally, there are symptoms of hyperthyroidism. Five percent to 10% of SO become malignant, the only absolute criterion for which is the presence of distant metastasis. Malignant transformation may be associated with V-raf marine sarcoma viral oncogene homolog B1 (BRAF) mutations (3). Malignant SO consists of follicular variant of papillary thyroid carcinoma (54%), papillary thyroid carcinoma (21%), mixed follicular/papillary carcinoma (12.5%), or follicular carcinoma (4). It can include elements of mucinous cystadenocarcinoma, Brenner tumor, carcinoid, or melanoma. To establish the diagnosis, one must rule out the following differential diagnoses: ovarian metastasis from a thyroid primary neoplasm, clear-cell adenocarcinoma, or tumor of oxyphilic appearance of the ovary (5,6). In the present case, increased serum Tg concentration, histology-proven peritoneal seeding, and radioactive iodine uptake in the liver and peritoneum on WBS were suggestive of the diagnosis (7). According to the literature, 88 malignant SO cases have been reported so far; the overall survival rate is 89% and 84%, respectively, at 10 and 25 years (8 –10). Most frequent clinical symptoms include an abdominal mass (78%) or acute pain (22%) (4). Aggressive disease course is rare (5 –7). Most tumors spread to the pelvic nodes, contralateral ovary, peritoneum, liver, lungs, and bones. Kim et al. recently described a case of peritoneal strumosis with favorable outcome (11). In contrast to their case, our patient did not respond well to radioactive iodine and had a very short survival. According to Robboy et al., adhesions, peritoneal fluid (>1 L), and ovarian serosal rent may explain the poor prognosis (10). This is the fifth lethal case reported in the literature (8,9). The patient recurred shortly after surgery, suffered from peritoneal carcinomatosis subsequent to anorexia, and died from cachexia (31% weight loss) at 37 months. Interestingly, CT and MRI scans disclosed the specific behavior of this well-differentiated tumor with intense uptake of radioactive iodine in metastases. Malignant ovarian tumors spread to the liver capsula and along the peritoneum folders, whereas hematogeneous spread (bones, lungs, adrenals) is typical of follicular thyroid cancer. At the end of her disease, she had a pelvic tumor, ascites, and pleural effusion, the so-called modified pseudo-Meigs syndrome triad (12).
On the basis of our experience with this patient and others in the literature, we recommend that thyroidectomy be performed quickly after pelvic surgery (13) to optimally eradicate thyroid remnants in the neck and pelvis by WBS. In addition, the serum TSH level should be rigorously maintained in the undetectable to very low range; new medications, including vascular endothelial growth factor inhibitors, should be investigated. Finally, the prevalence of BRAF and V-Ha-ras Harvey rat sarcoma viral oncogene homolog (HRAS) mutations in SO and their relationship to the prognosis and clinical course of SO should be investigated.
Footnotes
Acknowledgment
We thank Professor F. Bussiere for reviewing this article.
Disclosure Statement
All authors have nothing to disclose and claim that no competing financial interests exist.