
Abstract
Background:
Although 99mTechnetium-sestamibi scintigraphy with single-photon emission computed tomography (SPECT) and, recently, hybrid SPECT/computed tomography (CT) have been claimed to be the preoperative methods of choice for parathyroid localization in patients with primary hyperparathyroidism (PHPT) and concomitant nodular goiter (NG), they have never been compared in this setting. We aimed at testing the hypothesis that SPECT/CT may be superior to SPECT for parathyroid localization in patients with PHPT and NG.
Methods:
Thirty-three patients with PHPT and NG (one or more nodular lesions based on cervical ultrasound) who underwent open parathyroidectomy during 2004–2009 were reviewed. All patients had preoperative 99mTc-sestamibi planar scintigraphy and SPECT (18 patients) or SPECT/CT (15 patients) after cervical ultrasound. Sensitivity, specificity, and positive predictive value (PPV) (for both correct neck side and quadrant identification) were calculated for the two procedures through comparison with intraoperative findings. In addition, operative times were assessed if the surgery was only for PHPT and not for the six patients who also had thyroidectomy.
Results:
The sensitivity of SPECT/CT for correctly identifying the neck side containing an abnormal parathyroid was 93.7% versus 80% for SPECT (p = 0.21, not significant [ns]). The specificity and PPV for this attribute were 92.9% and 93.7%, respectively, for SPECT/CT versus 87.5% and 88.9%, respectively, for SPECT (p = 0.75 and 0.8, ns). SPECT/CT showed higher sensitivity than SPECT (87.5% vs. 55.6%; p = 0.0001) and higher PPV (87.5% vs. 62.5%; p = 0.0022) for correctly identifying the neck quadrant affected by PHPT. The specificity for this was 95.5% for SPECT/CT versus 88.5% for SPECT (p = 0.26, ns). Mean operative time was shorter after SPECT/CT than after SPECT (38 vs. 56 minutes; p = 0.034). One of the patients having SPECT/CT had double adenomas, and two had ectopic parathyroid glands, all of which were recognized preoperatively by this technique. Two of the patients having SPECT had double adenomas, and two had ectopic glands, none of which were recognized preoperatively. No patient had persistent or recurrent PHPT.
Conclusions:
SPECT/CT is superior to SPECT for preoperative imaging of patients with PHPT and NG. We recommend the routine use of SPECT/CT for work-up of all such patients, particularly if minimally invasive parathyroid surgery is planned.
Introduction
Although an expert endocrine surgeon can cure PHPT without the aid of any preoperative imaging in most patients by performing bilateral neck exploration (10); this seems overly invasive, as a solitary parathyroid adenoma is the cause of PHPT in 80%–90% of patients. Surgical exploration of a wide area distorts the normal anatomy of the neck and, therefore, has a higher rate of complications (11) and poorer cosmetic results (12). Bilateral neck exploration is more and more being reserved for situations in which parathyroid hyperplasia is suspected or concomitant thyroid surgery is anticipated (13).
99mTc-sestamibi scintigraphy combined with single-photon emission computed tomography (SPECT) and, more recently, hybrid SPECT/computed tomography (CT) have been recommended as preoperative methods of choice for parathyroid localization in the presence of NG (9,14,15). However, a comparison of these techniques in such a particular setting has not been published so far. The current study was, therefore, undertaken with the aim of comparing the sensitivity, specificity, and PPV of SPECT and SPECT/CT in patients with PHPT due to parathyroid adenoma(s) and coexisting NG. This would help determine whether SPECT/CT is more useful than SPECT in guiding the surgeon during parathyroidectomy, particularly minimally invasive parathyroidectomy.
Methods
Between January 1, 2004 and July 31, 2009, 72 patients with biochemical evidence of PHPT underwent open parathyroidectomy in the 1st Department of General Surgery (Brescia Civic Hospital, Italy). Preoperative work-up included physical examination; standard laboratory parameters including thyroid function tests, neck US, and plain chest radiogram. Altogether, 33 patients (45.8%) were diagnosed with concomitant NG, based on the literature (3,4), by neck US, and fine-needle aspiration biopsy. The term nodular goiter was used to define any enlarged thyroid gland with one (uninodular goiter) or more (multinodular goiter) nodular lesions. The charts of these cases were reviewed for clinical history, biochemical profile, history of radiation exposure, prior nonparathyroid neck operation, preoperative nuclear imaging, operative findings, and surgical outcomes.
The study group consisted of 12 (36.4%) men and 21 (63.6%) women with a median age of 53 years (range 18–81 years). Before surgery, the median total serum calcium was 11.4 mg/dL (range 10.4–18.1 mg/dL), and the median serum parathyroid hormone (PTH) was 146 ng/L (range 86–577 ng/L) (Table 1). The most common symptoms present were fatigue (52%), musculoskeletal pain (36%), and nephrolithiasis (34%). No patient had a history of radiation exposure or previous neck surgical exploration. All patients underwent 99mTc-planar and SPECT or SPECT/CT parathyroid scintigraphy after neck US (performed by the radiologist using a 7.5 MHz linear array) 2–5 days before surgery. Until December 2006, SPECT was routinely performed in our tertiary care university hospital for preoperative work-up of patients with PHPT (18 cases in this study group); since January 2007, this was replaced with SPECT/CT (15 patients). The same radiologist examined the two groups of patients. Imaging data provided by SPECT and SPECT/CT were compared with the intraoperative and postoperative findings. For the purposes of this study, the locations of glands were recorded according to the quadrant of the neck in which they were found (i.e., left superior, left inferior, right superior, and right inferior). If the position was beyond the neck or not in anatomic vicinity of the thyroid bed or thyroid gland, it was considered ectopic.
The two study groups were well matched (p not significant [ns]).
SPECT, single-photon emission computed tomography; CT, computed tomography.
The sensitivity, specificity, and PPV of both procedures were calculated; and the impact of SPECT/CT introduction on lesion localization and surgical procedure (mono- or bi-lateral neck exploration) was assessed. In addition, the operative times of the parathyroidectomies from skin incision to skin closure were evaluated for the 27 patients (15 from the SPECT and 12 from the SPECT/CT group) who had parathyroidectomy alone and not for the 6 patients (3 from each study group) in whom thyroid resection as well as parathyroidetomy were performed. Patients were evaluated at 8 days and 6 months postoperatively. Transient or permanent recurrent laryngeal nerve palsies as well as any permanent hypoparathyroidism (defined as a requirement for calcitriol and calcium supplementation persisting for more than 6 months) were recorded. Biochemical cure was defined as normal fasting calcium and intact PTH level at more than 6 months (16).
Imaging
All the patients received a standard activity of 740 MBq (20 mCi) of 99mTc-sestamibi (DuPont Pharma, Wilmington, DE) (effective dose-equivalent [EDE] 6.7 millisievert) (17). For the SPECT group (18 patients), a dual-head camera (GE Millenium VG; MEDX, Inc., Arlington Heights, IL) equipped with a low-energy high-resolution collimator was used with the following acquisition protocol: early (10 minutes postinjection) and late (1-hour postinjection) planar scan (acquisition time 10 and 20 minutes respectively, 128 × 128 pixels matrix); SPECT imaging about 90 minutes after injection (64 × 64 pixels matrix, 120 frames, angular step 3°, and 20 seconds per frame).
For the SPECT/CT group (15 patients), a dual-head variable-angle gamma camera and a low-power X-ray CT transmission system mounted on the same gantry (Infinia Hawkeye SPECT/CT system; GE Healthcare, Chalfont St. Giles, United Kingdom) were used.
The acquisition of planar and SPECT imaging was the same; moreover, a low-dose CT (140 kv, 2.5 mA, with 10 mm sections reconstructed in a 256 × 256 matrix) without contrast media was registered immediately after SPECT without moving the patient.
Finally, all patients received 74 MBq (2 mCi) of 99mTc-pertechnetate (EDE 1 mSv) (17) after the delayed image, and a 15-minute image of the thyroid gland was obtained and used for 99mTc-sestamibi/pertechnetate subtraction scintigraphy.
Operative procedure
All procedures were carried out by two experienced endocrine surgeons on patients under general endotracheal anesthesia. Through a small transverse cervical incision, parathyroid exploration was initially conducted on the side suggested by preoperative imaging. Bilateral neck exploration was not planned unless there was a preoperative indication based on diagnosis and treatment of thyroid disease (see below). Intraoperative quick PTH values were obtained for all patients. Frozen section was routinely used to confirm the presence of parathyroid tissue and the weight of excised parathyroid tissue.
Concomitant thyroid procedures were guided by thyroid pathology as identified preoperatively and/or intraoperatively. Thyroid nodules per se were not an indication for surgery, and only in 6 of the 33 patients with nodular disease (ND) was thyroid surgery performed either for mechanical or cosmetic reasons or because of suspected or documented malignancy (through preoperative fine-needle aspiration). Overall, hemi-thyroidectomy was performed in four patients and total thyroidectomy in two patients.
Statistical analysis
Based on a comparison between nuclear imaging reports and operative and histopathologic findings, true-positive, true-negative, false-positive, and false-negative results were recorded for each of the four quadrants of the neck and for each side of the neck for all of the 33 patients studied. Every individual was assumed to have four glands, unless the contrary was shown during surgery. The sensitivity, specificity, and PPV values of each imaging method for localizing hyperfunctioning parathyroid glands were calculated. The diagnostic units of study were the side and quadrant of the neck. We assessed the reliability of each procedure first in localizing the correct side of the neck (i.e., lateralization) and then the precise quadrant involved. Chi-square or Fisher's exact test, when appropriate, was used to compare categorical variables. The Mann–Whitney U-test was used to analyze differences in continuous variables (presented as median and range) between the two groups of patients. The level for statistical significance was set at p < 0.05. All tests were two sided. Statistical analysis was performed with statistical software for biomedical research (McCalc® Software for Windows; version 9.2.0.0).
Results
Of the 33 patients in this study, 24 (72.7%) patients underwent a planned monolateral neck exploration, 12 (80%) from the SPECT/CT group and 12 (66.7%) from the SPECT group. Two conversions to a standard bilateral cervical exploration were due to the presence of unanticipated multiglandular disease (MGD) (double adenomas), both in the SPECT study group; conversely, one case of double adenoma was correctly identified during preoperative work-up in the SPECT/CT group, and that patient underwent planned bilateral neck dissection. Three conversions were due to incorrect preoperative lateralization of the adenoma (because of false-positive thyroid nodules): two in the SPECT versus one in the SPECT/CT group; three further bilateral neck dissections were due to a concomitant thyroid disease that required total thyroidectomy in two cases (in the SPECT group) and contra-lateral hemi-thyroidectomy in one case (in the SPECT/CT group).
99mTc-sestamibi/pertechnetate subtraction scintigraphy correctly identified 26 of 36 histologically confirmed adenomas (72.2%) (including the three cases of MGD). Three adenomas could not be visualized, owing to their small size in all cases. Three false-positive results could be attributed to follicular thyroid adenomas. Interestingly, all cases of ectopic glands and MGD were missed by planar investigation.
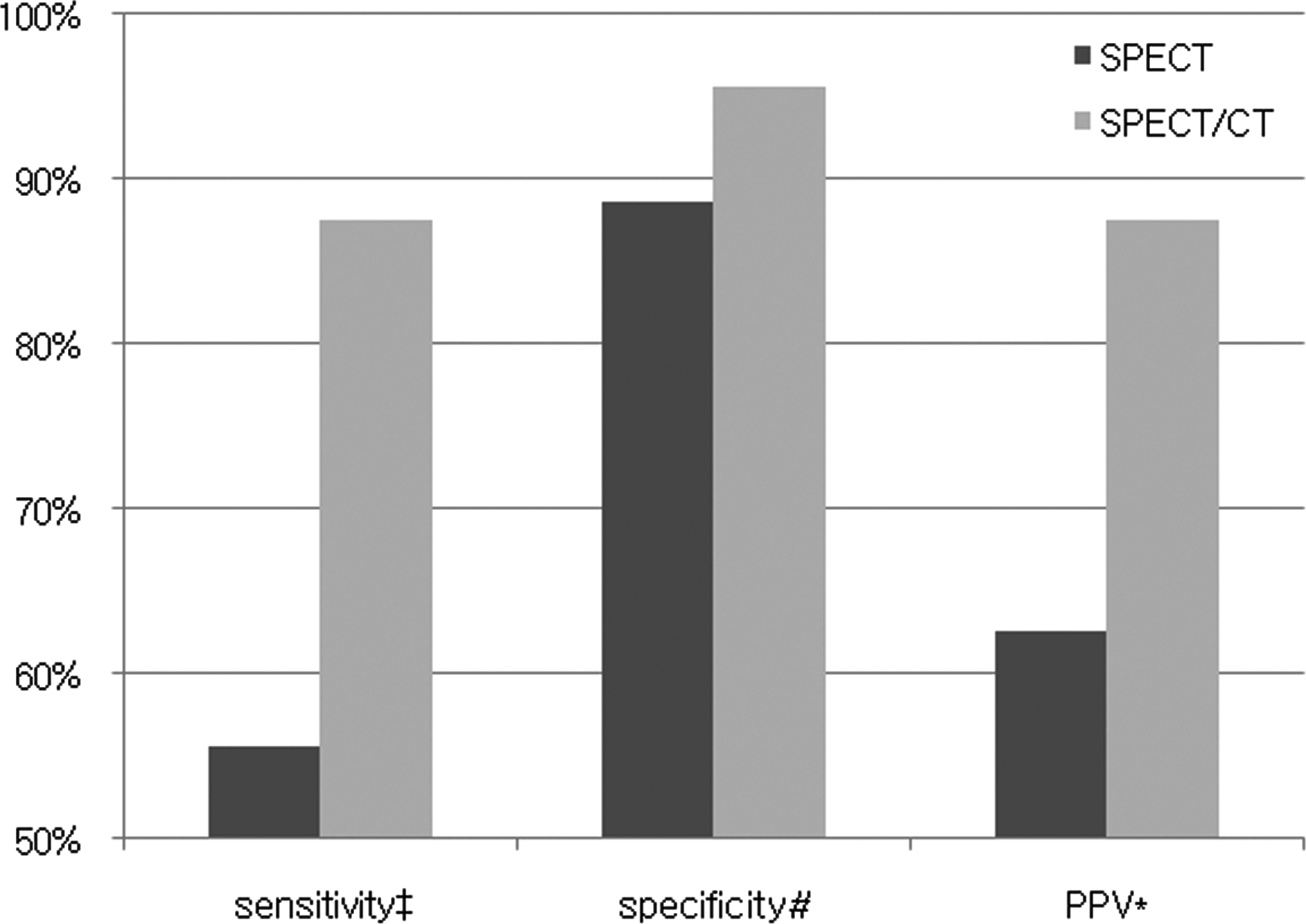
Intraoperative findings were compared with preoperative imaging (SPECT vs. SPECT/CT) for localization analysis in all patients. With regard to the right neck side localization, all but one patient in the SPECT/CT group had their parathyroid adenoma correctly lateralized versus 14/18 cases (77.8%) in the SPECT group (including two cases of double adenomas). Comparative analysis of parameters pertaining to the capability of lateralization of the adenoma found the following results: Sensitivity was 93.7% for SPECT/CT versus 80% for SPECT (p = 0.21); specificity was 92.9% for SPECT/CT versus 87.5% for SPECT (p = 0.75); and PPV was 93.7% for SPECT/CT versus 88.9% for SPECT (p = 0.8) (Fig. 1). The same analysis disclosed the following results for the correct neck quadrant identification: Sensitivity was 87.5% for SPECT/CT versus 55.6% for SPECT (p = 0.0001); specificity was 95.5% for SPECT/CT versus 88.5% for SPECT (p = 0.26); and PPV was 87.5% for SPECT/CT versus 62.5% for SPECT (p = 0.0022) (Fig. 2).

Comparative analysis between 99mTechnetium-sestamibi SPECT and hybrid SPECT/CT in terms of capability of locating the hyperfunctioning glands to the correct side of the neck. ‡ p = 0.21; # p = 0.75; *p = 0.8. SPECT, single-photon emission computed tomography; CT, computed tomography; PPV, positive predictive value.
Comparative analysis between 99mTechnetium-sestamibi SPECT and hybrid SPECT/CT in terms of capability of locating the hyperfunctioning glands to the correct quadrant of the neck. ‡ p = 0.0001; # p = 0.26; *p = 0.0022.
As for the relationship between imaging and operative time, we observed a slight, although significant, reduction of this parameter after SPECT/CT: In this group, the mean duration of surgery was 38 minutes (median: 33.5 minutes; range 25–100) as compared with 56 minutes (median: 40.5 minutes; range 28–114) recorded in the SPECT group (p = 0.034) (Fig. 3). We found four (12.1%) ectopic adenomas, two in each group. In the SPECT/CT group, 1 gland was found in the retroesophageal prevertebral plane and another in the retrotracheal plane. In both cases, SPECT/CT correctly identified the relation of the adenoma with the trachea, esophagus, and spine and optimized the surgical procedure. Both ectopic glands occurring in the SPECT group were in the thyrothymic ligament. SPECT successfully assigned the glands to the correct neck side but failed to recognize their aberrant position, thus entailing a time-consuming surgical exploration.

Comparison of operative time between the 99mTechnetium-sestamibi SPECT group and the hybrid SPECT/CT group: Box-and-whisker plots. The bars represent the mean operative time. In the Box-and-whisker plot, the central box represents the values from the lower to upper quartile (25–75 percentile). The middle line represents the median. The vertical line extends from the minimum to the maximum value, excluding far out values (values larger than the upper quartile plus three times the interquartile range), which are displayed as separate points.
Final pathological interpretation of glands removed was always consistent with adenoma. The median adenoma weight was 1.6 g (range 0.4–4.6 g). We did not find any significant relationship between gland size on the ability of either SPECT/CT or SPECT imaging to detect the adenoma, although the smallest adenoma (0.4 g) was missed with SPECT evaluation.
None of the patients were hypercalcemic at their 6-month follow-up evaluation. We observed three cases (9.1%) of transient postsurgical hypoparathyroidism. One of these (6.7%) was in the SPECT/CT group, and two (11.1%) were in the SPECT group (p = 0.86). One patient (3%) in the SPECT group had a transient recurrent laryngeal nerve injury after surgery.
Discussion
Data reported in the literature on the role of 99mTc-SPECT in detection of parathyroid lesions with concomitant NG vary widely, thus precluding any possibility of uniform judgment. In several reports, it has proved to be a reliable tool for localization of parathyroid glands in this particular setting, allowing also for additional information on thyroid nodules (18 –21). In the study by Lorberboym et al. (18), SPECT imaging correctly identified 95% of the adenomas in 39 patients. This positive result can be explained by the depth information and 3-dimensional location provided by SPECT, therefore surpassing the limits of planar imaging in the case of adenomas located behind the thyroid gland. Further, in the same report, the SPECT correctly identified malignant nodules in four out of five patients, being cold on 99mTc-pertechnetate imaging but showing avid uptake of 99mTc-sestamibi. However, despite these promising data, other reports claimed that even with SPECT the preoperative evaluation can be negative, mainly due to the interference of 99mTc-sestamibi avid thyroid lesions. In two recent studies, approximately 12%–18% of patients with PHPT had negative SPECT imaging, and up to 30% of patients with scan-negative findings were found to have MGD (22,23). In a large series of 338 patients, Civelek et al. (24) stated that SPECT failed to correctly lateralize 32 parathyroid lesions due to associated thyroid disease. Although these lesions were correctly localized on scintigrams, they were considered as false positive for the detection of parathyroid adenomas.
These findings prompted us to investigate whether the hybrid SPECT/CT may be more useful than SPECT in accurately guiding the surgeon during parathyroidectomy in patients with PHPT and concomitant NG. Comparative analysis disclosed a trend in favor of SPECT/CT, although not statistically significant, as having higher sensitivity for adenoma lateralization (almost 14% difference compared with SPECT). High values of specificity and PPV in this assessment, close to 90%, were, however, revealed for both procedures. As for localizing the correct neck quadrant where the adenoma was located, SPECT/CT appeared to have an advantage over conventional SPECT. This was true at least in terms of sensitivity (more than 30% difference) and PPV (25% difference).
It is important to note that the use of SPECT/CT instead of traditional SPECT entails limited additional expenditure (about 4% more cost) and low additive radiation dose, being the estimated EDE (per 70 kg individual) of 7.7 mSv after Hawkeye SPECT/CT, compared with 6.7 mSv after SPECT (10,17,25).
A comparison between SPECT/CT and SPECT not relating to the presence of concomitant NG has been carried out in several studies. These have yielded differing results. In a study of 48 patients, early SPECT in combination with dual-phase planar imaging identified 89% of surgically confirmed parathyroid adenomas, with or without CT fusion. The investigators concluded that CT fusion added no value to SPECT alone, except in locating ectopic parathyroid glands (14). In another investigation of 36 patients, in whom SPECT/CT was performed only on patients with negative or diagnostically uncertain planar imaging results, SPECT/CT contributed to localization and surgical planning in 39% of patients (26). In a more recent report, Lavely (27) found dual-phase SPECT/CT to be superior to dual-phase SPECT, achieving sensitivity, specificity, and diagnostic accuracy close to 72%, 99%, and 86%, respectively. Similar conclusions have been drawn by Neumann et al. (28) and Roach et al. (29), and even better results have been pointed out by Prommegger et al. (30), with SPECT/CT sensitivity being nearly 90% and specificity and accuracy being close to 100% in their report.
In the current study, we also reported a significant decrease (almost 20 minutes) in the operative time after the introduction of SPECT/CT. This event may well be regarded, at least partially, as the consequence of the learning curve between the two study periods. However, the close temporal proximity and especially the small number of procedures of the more recent group minimize, in our opinion, the extent of bias.
In addition, SPECT/CT appeared in this study to be useful in difficult clinical scenarios, such as ectopic adenomas, as previously outlined also by Radan and Gorenberg (31) and MGD. In fact, both cases of ectopic glands occurring in the SPECT/CT group were correctly anticipated in preoperative assessment, allowing for operative times near to the lower limit of the range (40 and 45 minutes, respectively). Conversely, SPECT revealed poor reliability in this condition, and both ectopic adenomas of this group were found after a time-consuming neck dissection. Altogether, ectopic adenomas were documented in the present study in 4 of the 33 patients, a percentage (12.1%) that is comparable with the 8% to 11% reported in the literature (32,33). As for the challenge posed by MGD, Wimmer et al. recently stated that SPECT/CT image fusion is a reliable method for diagnosing such conditions, being also superior to CT or 99mTc -SPECT alone (34). In our study, 3 out of 33 patients (9%) had MGD (double adenomas). Our analysis outlined the superiority of SPECT/CT in this particular setting (100% correct diagnosis), whereas both cases in the SPECT group required bilateral neck exploration due to failed preoperative recognition. Interestingly, even poorer results were reported by neck US, which missed all cases of ectopic glands and double adenomas.
The weight of the adenoma had no significant effect on the higher sensitivity and PPV of SPECT/CT in our study. This observation differs from the findings of Neumann et al. (28), who found that gland weight influenced the ability of SPECT/CT to detect the adenoma. A number of other studies are available on this argument with regard to SPECT, some sustaining a positive impact (18 –20,35,36) and others rejecting any influence (37). However, no comparative analysis of SPECT versus SPECT/CT has been addressed on this issue.
Conclusions
At present, the role of SPECT/CT in preoperative localization of parathyroid adenomas in cases with concomitant NG has not been firmly established, as controlled comparative studies are still lacking. In our study, although the trend toward superior lateralization observed for SPECT/CT did not reach statistical significance, our data clearly support the concept that SPECT/CT is the imaging procedure of choice in patients with PHPT and NG due to its higher sensitivity, specificity, and PPV for correct neck quadrant identification, resulting in better focus for the surgical exploration and shorter surgical times. In addition, even in the rare cases of ectopic parathyroid adenomas as well as in the presence of MGD, the SPECT/CT appeared to have an additive role. Therefore, unless contradicted by further studies, we think that SPECT/CT should be the primary preoperative imaging method when parathyroid adenoma coexists with NG, particularly if minimally invasive parathyroid surgery is planned. We do recommend larger studies on patients with PHPT and NG to confirm our findings, as the size of our series was relatively small.
Footnotes
Acknowledgments
The authors are grateful to the membership of the Department of Radiology and Nuclear Medicine (University of Brescia School of Medicine, Brescia, Italy) for contribution provided so far. They also thank Deborah Chiesa, M.D., for her valuable and continuous support.
Disclosure Statement
The authors have no conflict of interest that could be perceived as prejudicing the impartiality of the research reported. In particular, this study did not receive any support from the industry that makes or markets the studied compounds.