
Abstract

We report the case of a woman with subclinical thyroid autoimmunity who developed overt hypothyroidism after treatment of Cushing's syndrome, presumably reflecting reactivation of the immune system following immune suppression due to hypercortisolism. The patient was a 33-year-old woman with a severe Cushing's syndrome due to a bilateral nodular hyperplasia. She had marked cushingoid features, especially hirsutism, a long-lasting amenorrhea, and a severe depression.
The patient underwent thyroid tests because of a familial history of thyroid autoimmunity. Findings were compatible with a euthyroid autoimmune thyroiditis, with normal serum thyroid hormones and thyrotropin (TSH) (free thyroxine [FT4]: 1.49 ng/dL, normal range [n.r.]: 0.7–1.7; free triiodothyronine [FT3]: 0.39 ng/dL, n.r.: 0.27–0.57; TSH: 2.25 mU/L, n.r.: 0.4–3.4), and detectable antithyroid autoantibodies (antithyroglobulin [TgAb]: 535 U/mL, normal value [n.v.]: <30; antithyroperoxidase [TPOAb]: 58.3 U/mL, n.v.: <10). At ultrasound, the thyroid volume was 6.2 mL with the hypoechoic pattern typical of autoimmune thyroid diseases (Fig. 1a).
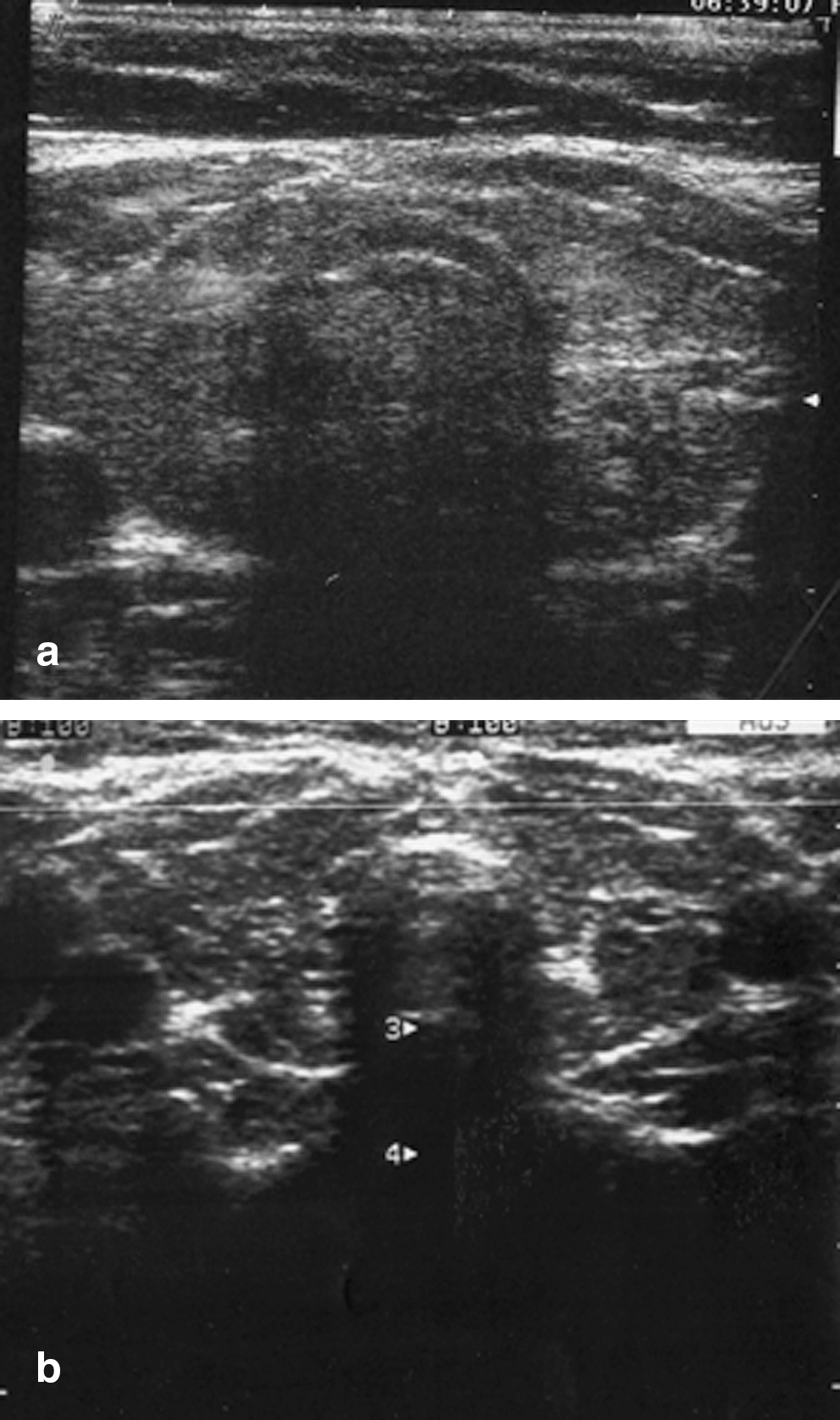
Thyroid ultrasonography before (
The patient was treated with bilateral adrenalectomy in November 2007 and then given hydrocortisone and fluorhydrocortison for adrenal deficiency. Two months later, hypercortisolism was under remission, both clinically and biochemically. Serum adrenal corticotropic hormone (ACTH) (21 pg/mL, n.r.: 10–52), K+ (3.8 mEq/L, n.r.: 3.5–5.1), and blood pressure (120/80 mmHg) were normal, suggesting a fair control of adrenal deficiency and a remission of hypercortisolism. Most Cushing's symptoms and features had improved, especially hirsutism and depression, but also moon face, facial flushing, buffalo hump, striae, and acne, which were all present before adrenalectomy. Menstrual cycles had reappeared. However, serum thyroid tests showed a severe hypothyroidism, with low FT4 (0.17 ng/dL) and FT3 (0.22 ng/dL), and high TSH (76 mU/L). Antithyroid autoantibodies had increased (TgAb: 1703 U/mL; TPOAb: 993 U/mL) and the thyroid hypoechoic pattern at ultrasound was more pronounced (Fig. 1b). The patient was given
Hypercortisolism exerts an inhibitory action on the immune function (1). Patients with hypercortisolism have a reduction of the lymphoid tissue mass and display a moderate lymphopenia, which can result in increased susceptibility to infections (2). Correction of hypercortisolism can be followed by the so called rebound phenomenon, namely, the rapid increase of the immune function, which may worsen a preexisting autoimmune disease or precipitate an autoimmune disease in predisposed subjects (1). A similar phenomenon can be observed following pregnancy. The immune system, suppressed during pregnancy, is reactivated after delivery, which can exacerbate a preexisting autoimmune condition or determine the ex novo appearance of autoimmunity. In our patient, very likely, reactivation of the immune system after adrenalectomy caused an exacerbation of the preexisting autoimmune thyroiditis, with development of severe hypothyroidism. On the other hand, there were no other explanations for the appearance of hypothyroidism. The patient had not received iodine loads (the last computed tomography scan had been performed 6 months before), and her urinary iodine levels were normal. As reported above, our patient had a severe Cushing's syndrome, which was cured within a relatively short period. Whether our considerations apply also to milder forms of Cushing's syndrome and in patients in whom longer periods are necessary to cure hypercortisolism remains to be established.
To our surprise, the literature on this matter seems quite scarce. Although other authors have reported a very few similar cases, to our knowledge there is only one study in which this issue was investigated in a population. Previous case reports refer to the exacerbation of Graves' disease and autoimmune pemphigus following adrenalectomy for Cushing's syndrome (3,4), with timing patterns similar to that we observed. In the population study available, Colao et al. (1) evaluated retrospectively the occurrence of autoimmune thyroid diseases in 20 patients with Cushing's disease after successful surgical treatment. They found an increased prevalence of antithyroid autoantibodies, up to 60% after the cure compared with 20% before the cure. In addition, they found that after Cushing's treatment 25% of patients had developed hypothyroidism, mainly subclinical, which occurred always in association with detectable antithyroid autoantibodies. Finally, serum antithyroid autoantibodies became detectable after treatment in 40% of the patients in whom they were undetectable before.
On the basis of our observation and on the previous studies (1,3,4), the possibility of the appearance or worsening of an autoimmune disease should be kept in mind when planning the treatment for Cushing's syndrome.
Disclosure Statement
The authors declare that no competing financial interests exist.