
Abstract
Background:
Autoimmune thyroiditis (AIT) may be associated with other organ-specific autoimmune disorders, including autoimmune gastritis, but the prevalence of this association is not entirely quantified. The aim of this study was to investigate the prevalence of parietal cell antibodies (PCA) in a large cohort of consecutive patients with AIT.
Methods:
We retrospectively studied 2016 consecutive women and 258 men with AIT seen at our referral center in the period from 2004 to 2008. All patients were screened for the presence of PCA in the serum.
Results:
The prevalence of serum PCA in female patients was 29.7% and progressively increased from 13% in the first-second decade of life to peak at 42% in the ninth decade. During follow up, 21.1% of the PCA-positive patients converted to PCA-negative status. Mean (±standard deviation) basal PCA levels in this group were significantly lower (32 ± 28 U/mL) compared with those remaining PCA positive (129 ± 200 U/mL). A similar prevalence (29.8%) with a similar age-dependency was found in male patients.
Conclusions:
In conclusion, our study demonstrates a high, age-dependent prevalence of PCA in an unselected large population of patients with AIT.
Introduction
Traditionally, PCA have been detected on mouse-kidney stomach tissue sections using indirect immunofluorescence assays. Although these tests are generally highly sensitive and specific, interpretation of the immunofluorescent patterns is operator dependent and time consuming. Enzyme-linked immunosorbent assays (ELISA) directed to the specific antigen (purified gastric H+/K+ ATPase) of PCA have been validated as specific and sensitive alternatives to immunofluorescence method. When the two methods are compared, similar results are obtained (25,26).
The aim of our study was to determine the prevalence of PCA using an ELISA method in a large and consecutive series of female AIT patients at the time of their diagnosis and during follow up.
Patients and Methods
We studied a cohort of 2016 unselected consecutive women (mean age ± standard deviation [SD]: 53.2 ± 16 years; range 9–91) and 258 men (mean age ± SD: 53.2 ± 17.3 years; range 14–84) with AIT who were seen at our referral center for thyroid disease from 2004 to 2008. The diagnosis of AIT was based on typical thyroid ultrasonographic changes and presence of elevated serum TPO antibodies (AbTPO) and/or anti-TG antibodies (AbTG). All patients were screened for the presence of PCA in the serum.
Hormonal assays
Free triiodothyronine and free thyroxine were measured using a commercial chemiluminescent assay (Beckman Coulter, Inc. Fullerton, CA); thyrotropin was determined by chemiluminescent assay (EURO/DPC Limited Llanberies, Gwynedd, United Kingdom); AbTG and AbTPO were determined by chemiluminescent assay (EURO/DPC Limited Llanberies); and anti-Tg levels >45 U/mL and anti-TPO levels >35 U/mL were considered positive. PCA were determined in serum using a commercial immunoenzimatic-assay (Chemactil, Angri, Italy). The limit of detection of our method was 0.5 U/mL. For statistical analysis, values <0.5 U/mL were computed as 0.5 U/mL. The normal upper limit in our laboratory (mean + 2 SD of our control subjects) is 14 U/mL.
Autoantibodies anti-21-hydroxylase were determined in serum using a commercial radioimmunoassay (CIS Bio International, GIF-SUR-Yvette CEDEX, France). The limit of detection of our method was 0.16 U/mL. Serum levels greater than 1 U/mL were considered as positive.
Blood samples were taken between 8 and 10 a.m., after an overnight fast, separated by centrifugation (within 2 hours) and stored in 0.5 mL aliquots at −20°C until assayed. Thyroid volume was assessed by ultrasonography using a color Doppler apparatus (Technos MP; Esaote Biomedica, Florence, Italy) with a 7.5-MHz linear transducer. To obtain the thyroid volume, the three diameters of both lobes were measured, and the total volume was calculated according to the ellipsoid model (width × length × thickness × 0.52 for each lobe) (27).
Statistical analysis
Since thyroid hormones, thyroid autoantibodies, and PCA do not conform to a normal distribution, statistical analysis was always performed using nonparametric tests: Mann–Whitney U test for comparison of group, Fisher's exact test and chi-square test (χ 2) for difference in distribution of categorical data, and Spearman's rank for correlation tests.
Cut-off value was defined using receiver operating characteristic (ROC) curves computed by an appropriate software package Graph Pad Prism version 4.0 (Avenida de la Playa, La Jolla, CA). A p-value of <0.05 was considered statistically significant.
Results
Prevalence of PCA in AIT patients
Serum PCA levels in 2016 women with AIT ranged <0.5–4539 U/mL (mean ± SD: 37 ± 159 U/mL; median 46 U/mL). Increased levels of serum PCA (>14 U/mL) considered as positive were found in 600/2016 (29.7%) women with mean levels of 116 ± 277 U/mL. As shown in Figure 1, the frequency distribution of PCA-positive levels showed that 92.1% of the patients had PCA levels between 14 and 300 U/mL and only 7.9% had higher PCA levels. As expected, the frequency distribution of our female population showed the typical trend for AIT with a peak of prevalence between 40 and 60 years of age and a mean of 53 ± 16 years. The same age distribution was found in the PCA-negative women (mean age 51.7 ± 16.3 years), whereas PCA-positive women showed a slight shift toward older decades of life and had significantly higher mean age (56 ± 15 years; p < 0.0001) than PCA-negative patients (Fig. 2). As shown in Figure 3, the prevalence of positive PCA women increased from 13% in the first-second decade of life to 42% in the ninth decade.

Frequency distribution of serum parietal cell antibodies (PCA) levels in 600 PCA-positive patients.
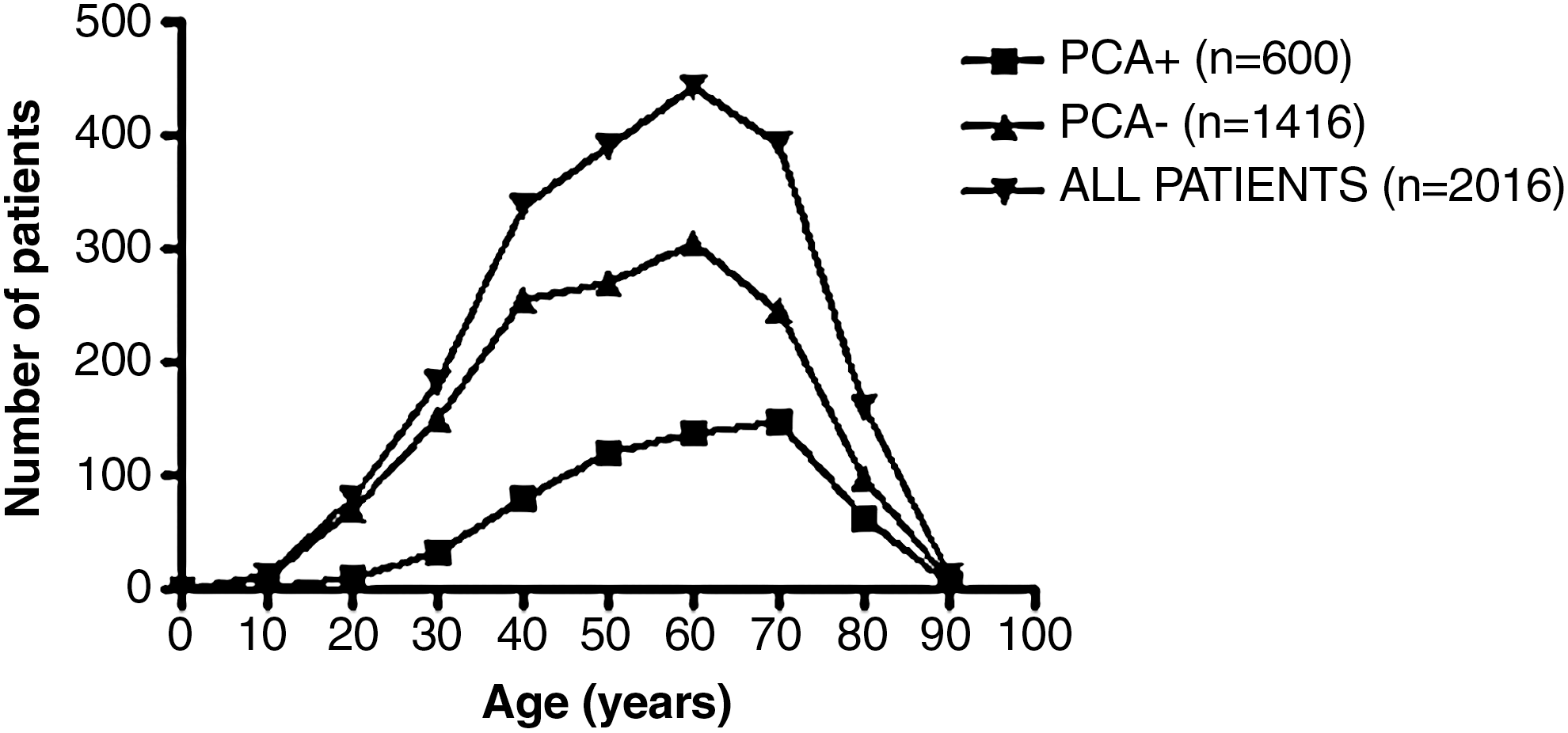
Age distribution of PCA + (▪), PCA − (▴), and all patients (▾) in our series.

Prevalence of PCA-positive patients (%) by decades of life.
Increased levels of serum PCA were found in 77/258 (29.8%) male patients with mean levels of 75 ± 57 U/mL. PCA-positive men showed the same age-dependent trend of PCA-positive women, with a progressive increase from 3% in the first-second decade of life to 27% in the sixth decade.
Serum PCA and thyroid parameters
Thyroid volume at ultrasound was significantly (p = 0.003) larger in PCA-negative patients (14.1 ± 13.7 mL) than in PCA-positive patients (13.3 ± 14.1 mL). Serum AbTPO levels (but not AbTG levels) were significantly (p = 0.015) higher in PCA-positive patients (633 ± 594 U/mL) compared with PCA-negative patients (562 ± 579 U/mL), and serum PCA levels were significantly correlated with AbTPO levels (p = 0.0103) (Fig. 4).
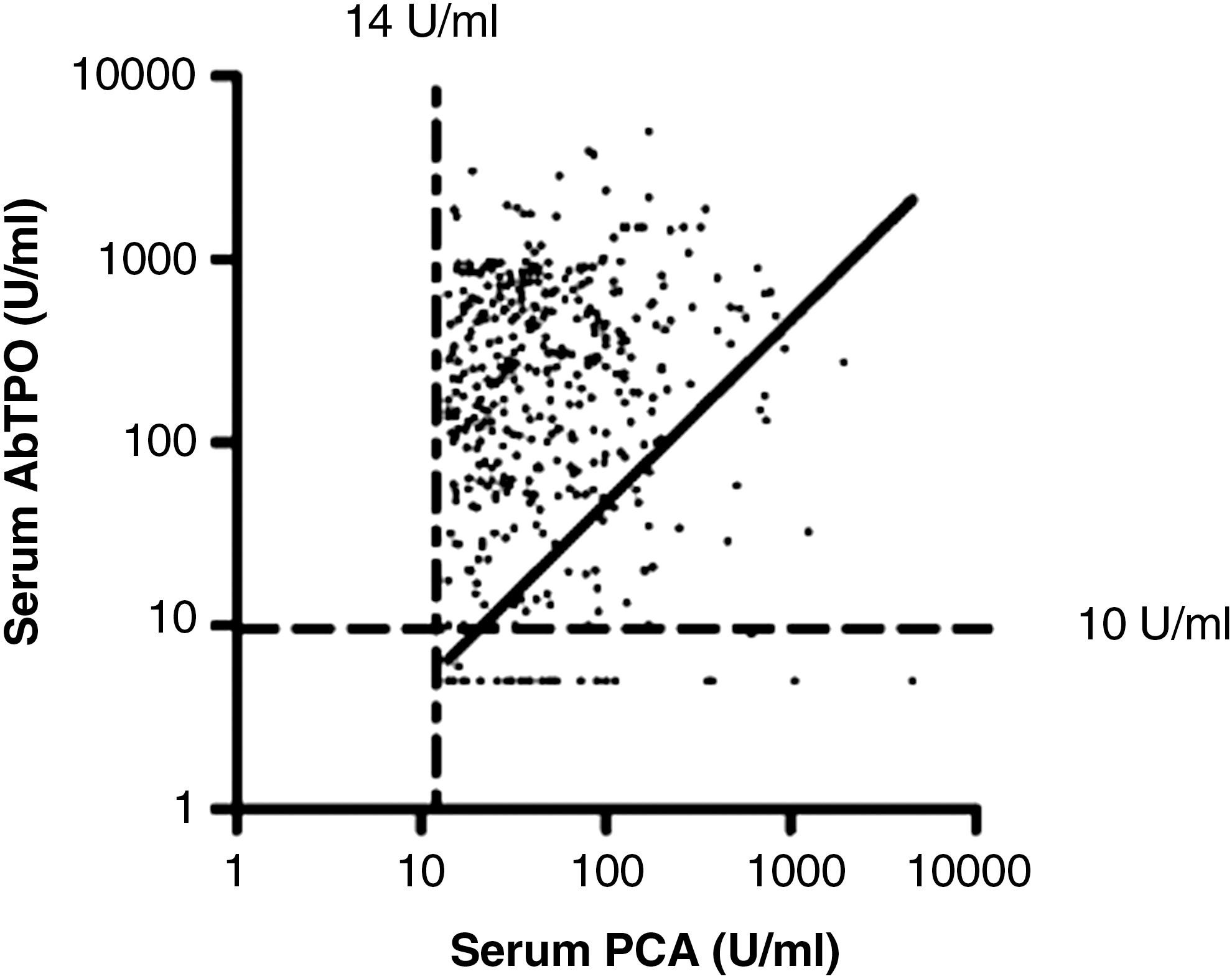
Correlation between serum PCA levels and thyroid peroxidase antibodies (AbTPO) levels in 600 PCA-positive patients. The dashed lines represent the upper normal limit of PCA and AbTPO levels.
At basal examination in our clinic, 671/1266 PCA-negative (53%) and 354/600 (59%) PCA-positive patients were clinically or subclinically hypothyroid with or without levothyroxine replacement therapy. The rate of hypothyroidism was significantly higher in the PCA-positive group (p = 0.01 by χ 2).
Serum PCA and anti 21-hydroxylase antibodies
Serum anti 21-hydroxylase antibodies levels were positive in 77/2016 female patients (3.8%) with similar positivity in PCA-positive patients (4.3%) and in PCA-negative patients (3.6%) (p = 0.43 by χ 2). Serum PCA levels were not correlated with anti-21-hydroxylase antibodies levels (p = 0.6). This analysis was not performed in male patients due to the lower number of subjects.
Follow-up data
In 364/600 (60.6%) PCA-positive patients and 559/1308 (42.7%) PCA-negative patients, we had follow-up data at 24 months. In 287/364 (78.9%) PCA-positive patients, serum PCA levels remained elevated during follow up. A conversion from PCA-positive to PCA-negative levels was found in 77/364 (21.1%). Mean PCA levels at the first observation were significantly higher (129 ± 200 U/mL) in confirmed PCA-positive patients compared with not confirmed PCA-positive patients (32 ± 28 U/mL) (p < 0.0001). By ROC curve analysis (Fig. 5), we found that PCA levels of 47 U/mL had the better sensitivity (89%) and specificity (62.9%) to maintain PCA positivity at subsequent controls, suggesting that only PCA levels >47 U/mL should be considered true positive, at least in our condition. Patients with PCA levels higher than 47 U/mL (high-titer PCA) and patients with PCA positivity lower than 47 U/mL (low-titer PCA) had similar mean age (57.5 ± 14.2 and 56.4 ± 15.5 years, respectively) and similar frequency distribution by age. Only a small minority of PCA-negative patients (25/559; 4.4%) converted from PCA-negative to PCA-positive status during follow up.
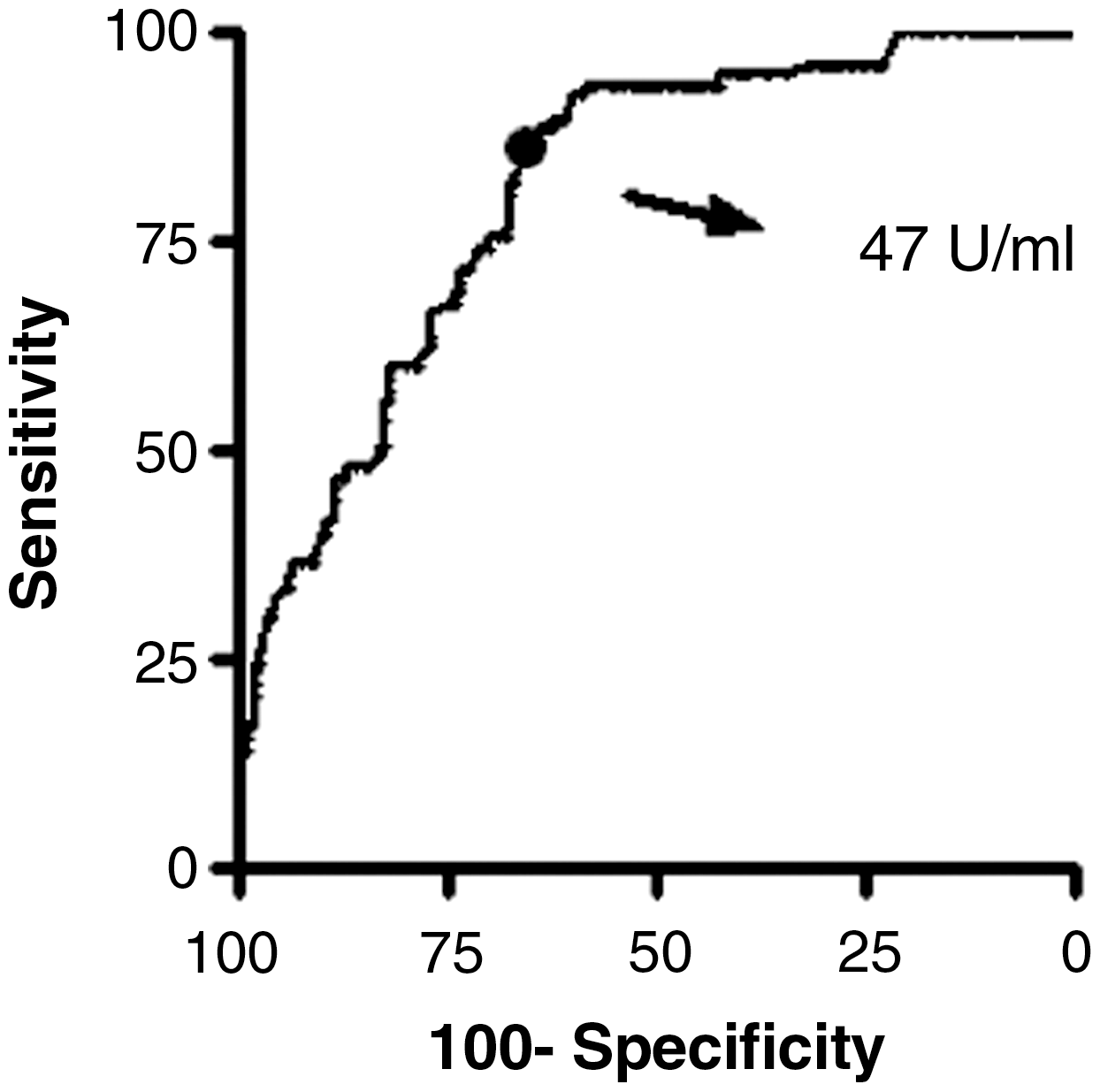
Receiver operating characteristic curve for basal PCA level, as a marker of future confirmed positivity. The arrow indicates the level with the best sensitivity and specificity.
Discussion
This study shows a prevalence of positive PCA of 29.7% in female patients and 29.8% in male patients with AIT, one of the highest reported up to now. One possible explanation for this finding is that other series mainly included younger subjects who have lower prevalence of positive PCA as was also noted in our series (1,2,23,28).
We observed an age-dependent progressive increase in PCA positivity among patients with AIT peaking at the ninth decade of life in women and at the sixth decade in men, in keeping with the general concept that the prevalence of autoimmunity progressively increases with age. This phenomenon has been reported in patients with type 1 diabetes mellitus (17,18,28,29) and even in normal subjects (30).
AIT may be associated with a number of organ-specific autoimmune diseases. In view of our 29.7% prevalence in patients with AIT and of that found in other series of patients with AIT or other autoimmune diseases (8,21 –23), it is possible to conclude that the association of AIT and autoimmune gastritis is the most frequent. A possible link explaining this association may be the presence of a common epitope shared by the gastric parietal cell antigen and the TPO antigen (31).
Apart from the interest of this epidemiological observation, there is also a clinical utility for detecting PCA autoantibodies. Monitoring biochemical parameters (such as gastrin, pepsinogen I/II ratio, and ghrelin) suggestive of gastric mucosa damage may, in fact, result in early detection and treatment of the complications (pernicious anemia and iron deficiency anemia) associated with autoimmune gastritis up to the prevention or early detection of gastric cancer.
An interesting observation in our study is that PCA-positive patients had lower thyroid volume, higher AbTPO levels (correlated with PCA levels), and higher rate of overt or subclinical hypothyroidism, suggesting the presence of a more severe form of thyroiditis.
Nearly 20% of our PCA-positive patients converted to PCA-negative status during follow up. The reasons for this is not evident, but the observation that this subgroup of patients was the one with the lowest positive levels of PCA (compared with positive patients not converting to PCA negative) may lead to speculation that such low positive levels of PCA are not significant and may be probably considered as normal, thus increasing the cut-off between PCA-positive and PCA-negative status.
As a matter of fact, the 47 U/mL cut-off found with ROC analysis is coincident with a previous study of our group (16) where we demonstrated that a 45 U/mL cut-off was the one distinguishing PCA-positive patients with proven organ damage from those without. Alternatively, we can speculate that in some patients the antigen presentation to the immune system is of short duration and is not sufficient to elicit a stable response by the competent immune cells.
In conclusion, our study demonstrates a high, age-dependent prevalence of PCA in a large population of female patients with AIT and suggests that PCA should be measured in any patient in whom AIT was diagnosed. The clinical utility of measuring these autoantibodies is to detect the appearance of gastric damage as soon as possible by monitoring biochemical markers of atrophic gastritis.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist