
Abstract
Background:
Most solitary hyperfunctiong regions on thyroid scan consist of benign tissue. Here we report a patient with a Burkitt-like lymphoma that was infilterated into a region containing a hyperfunctioning nodule.
Summary:
A 56-year-old man was referred to our Endocrine Unit in May 2009 due to the incidental discovery of a large left thyroid lobe nodule by a computed tomography study. This had been performed to search for a primitive tumor in a patient with bone metastasis. He was clinically and biochemically thyrotoxic with no evidence of humoral thyroid autoimmunity. The nodule had a dyshomogenous appearance at neck ultrasonography, with multiple hypoechogenic areas and calcifications. (99m)-Technetium thyroid scintiscan revealed a hot nodule with suppression of the contralateral lobe. Fine-needle aspiration cytology indicated the presence of neoplastic cells not of thyroid origin. Remission of hyperthyroidism was obtained with methimazole, and the patient was submitted to left lobe thyroidectomy and istmectomy. Histological analysis of the surgical specimen led to a diagnosis of Burkitt-like large B-cell lymphoma harbored within a thyroid adenoma. After further staging, the final diagnosis was stage IV E Burkitt-like lymphoma with the involvement of the bone and the thyroid. This is the first description of an aggressive Burkitt-like lymphoma that infiltrated an hyperfunctioning thyroid adenoma, thus presenting as a hot nodule at thyroid scintiscan. In our patient there was no humoral or histological evidence of thyroid autoimmunity, thus suggesting a metastatic seeding of the lymphoma within the hyperfunctioning thyroid nodule.
Conclusions:
Involvement of the thyroid gland by Burkitt-like lymphoma is extremely rare as is close localization of malignancy and a hyperfunctioning thyroid nodule. As highlighted by the present report, performing fine-needle aspiration cytology should be always considered in the clinical context of a metastatic disease of unknown origin or when there are ultrasonography signs suggesting malignancy, even when the nodule is hyperfunctioning.
Introduction
Patient
A 56-year-old man was referred to our Endocrine Unit in May 2009 for evaluation of a thyroid nodule that was noted on computed tomography as part of the workup of a suspected underlying neoplasm. In January 2009 he suffered a pathological fracture of the right femoral diaphysis due to a lytic lesion of unknown origin. A computed tomography scan of the thoracic and abdominal districts revealed two small nodules in the right kidney, an abnormal mass in the anterior mediastinum corresponding to the thymic area and a large nodule of the left thyroid lobe. In April 2009 the patient underwent an osteosynthesis of the right femoral diaphysis. At histology, the resected bone fragment was found to be extensively necrotic and to contain a neoplastic cell population, which was not further defined.
When first seen in our outpatient clinic, the patient appeared slightly thyrotoxic with fine tremors and sinus tachycardia, but no evidence of inflammatory eye disease. Neck palpation revealed a firm, 5-cm nodule in the left thyroid lobe. The right thyroid lobe was barely palpable and there was no evidence of lymphoadenopathy. Thyroid function tests indicated overt thyrotoxicosis (thyrotropin < 0.004 mU/L, range 0.4–4 mU/L; free thyroxine = 31.2 pg/mL, range 8.0–19.0 pg/mL; free triiodothyronine = 7.8 pg/mL, range 1.8–4.2 pg/mL). Tests for anti-thyroglobulin, anti-thyroid peroxidase, and anti-thyrotropin-receptor antibodies were negative. Serum thyroglobulin was high (434 ng/mL), and serum calcitonin was undetectable (<2 pg/mL).
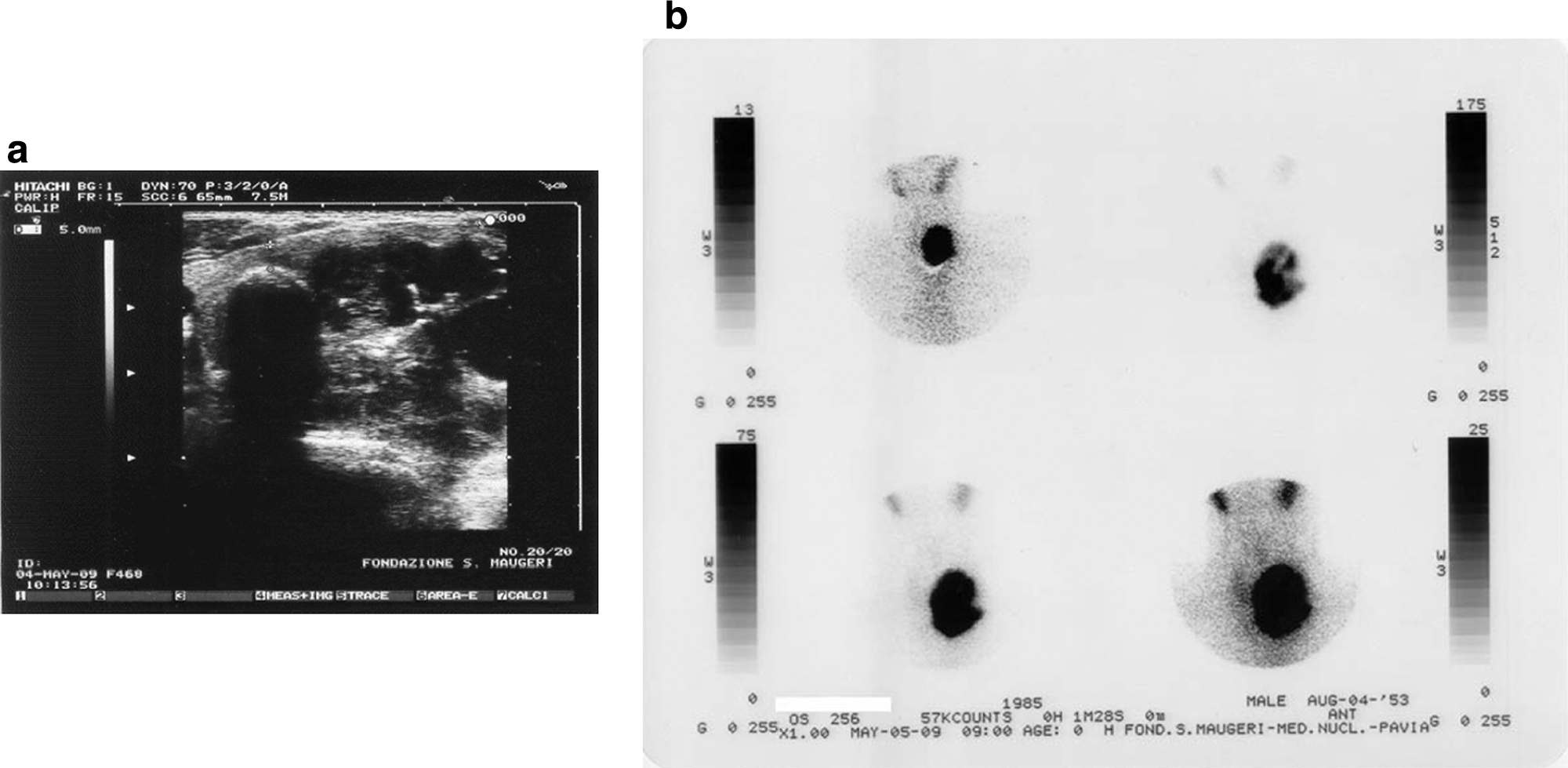
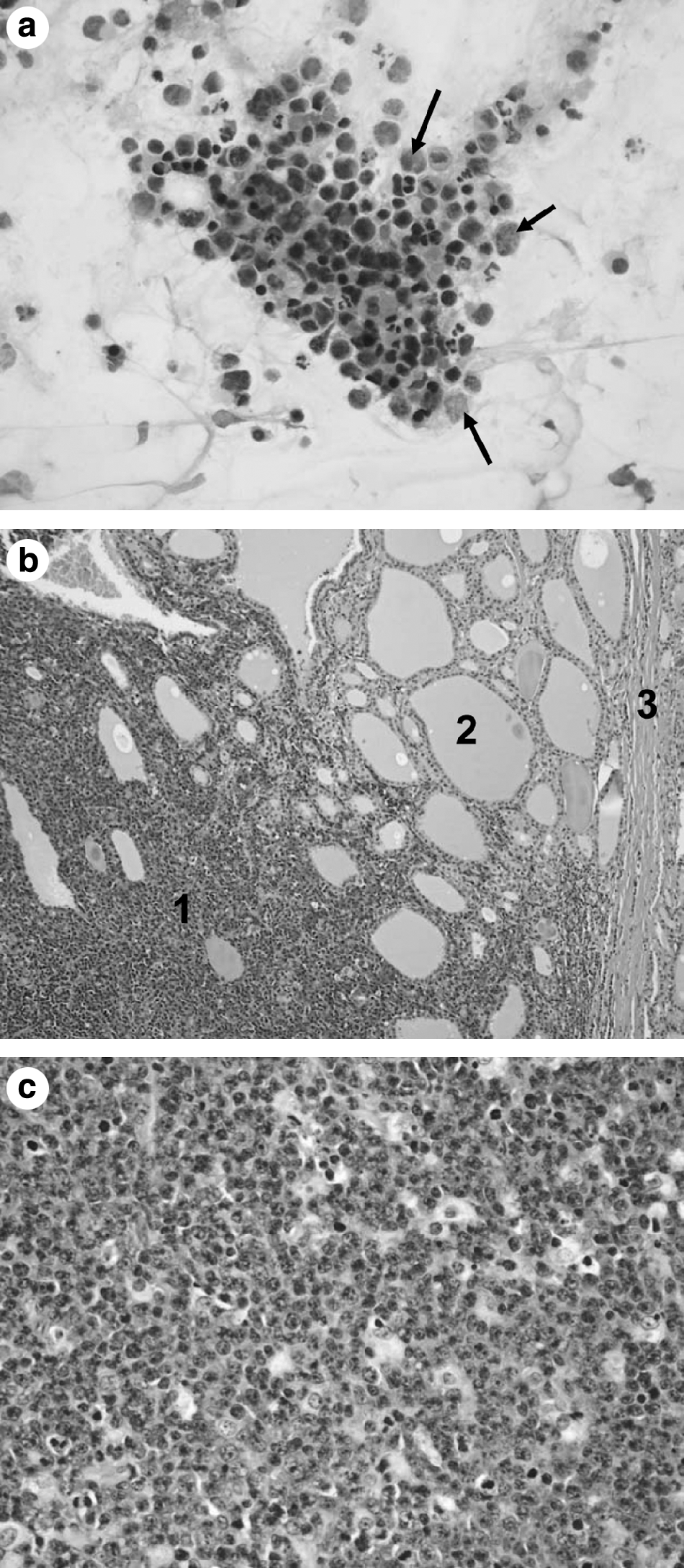
Neck US showed an asymmetrical thyroid with a huge left lobe (estimated volume = 70 mL), which was almost completely occupied by a large nodule measuring 46 × 49 × 60 mm. The nodule was not homogenous but contained multiple hypo and anechogenic areas, intralesional vascular spots, and calcifications (Fig. 1a). A rightward tracheal dislocation was evident. Due to the thyrotoxic state, a (99m)-technetium scintiscan was ordered, which revealed a large hot nodule of the left thyroid lobe. No radioisotope uptake was evident in the right lobe. Thus, the nuclear medicine imaging was consistent with a hyperfunctioning thyroid nodule with suppression of the contralateral lobe (Fig. 1b). FNAC of the left nodule was performed, which yielded a population of neoplastic cells that were not considered of thyroid origin (Fig. 2a). The patient was started on methimazole (20 mg/day), with remission of hyperthyroidism within 3 weeks. In June 2009, an 18-fluorodeoxyglucose positron emission tomography was performed, which showed a pathological uptake of the radioisotope corresponding to the left thyroid nodule, as well as in the mediastinum and right femur. Considering the malignant cytological findings and the surgical accessibility of the thyroid nodule, a left lobe thyroidectomy and istmectomy were performed. The thyroid nodule was easily resectable, with no evidence of adherence to the trachea or to other neck structures. Histological analysis led to the diagnosis of diffuse large B-cell lymphoma (DLBCL) (1), with an high proliferation index (Ki-67 > 95%) and a CD20/CD79a positivity. Given the high proliferation rate, it was classified as a Burkitt-like lymphoma (Fig. 2b, c). The surgical specimen of the nodule also contained thyroid tissue with a macrofollicular appearance, marked fibrosis, and dystrophic calcifications. A nuclear magnetic resonance of the brain excluded cerebral metastases. Further investigations involved the assay of serum lactate dehydrogenase (1585 U/L, range 240–480 U/L) and β2-microglobulin (2310 mg/L, range 609–2366 mg/L). A bone marrow biopsy did not show malignant cells. The final diagnosis was stage IV E Burkitt-like lymphoma according to the WHO classification. According to the recent revision of the 2008 WHO Classification (2), this lymphoma may alternately be included in the provisional category termed B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Burkitt lymphoma. The patient was treated with eight cycles of intensive chemotherapy (hyperfractionated cyclophosphamide, vincristine, doxorubicine, and dexamethasone), and had dramatic reduction of all lesions with improvement of symptoms.
(
(
Discussion
Lymphoma within the thyroid gland is a rare and heterogeneous disease, accounting for 1%–5% of all thyroid cancers and occurring in 1%–2.5% of all lymphomas (3). Lymphomas more commonly spread to lymph nodes, bone marrow, central nervous system, liver, and gastrointestinal tract. As noted, systemic lymphoma does not commonly spread to the thyroid gland (4). Primary thyroid lymphoma is a rare disease, almost always arising in the lymphocytic infiltrate of chronic autoimmune thyroiditis (4). Epidemiological studies indicate that patients with chronic lymphocytic thyroiditis have a 67- to 80-fold increased risk of developing thyroid lymphoma (5). In a large series of primary thyroid lymphomas (3), the most prevalent histotype was DLBCL (50%). Mucosa-associated lymphoid tissue lymphoma, follicular lymphoma, Hodgkin disease, Burkitt lymphoma, and small cell leukemia accounted for 23%, 12%, 7%, 4%, and 4%, respectively. Most patients affected by this type of neoplasia are middle-aged or elderly people, who develop a rapidly growing nodule (6), producing compressive symptoms such as hoarseness, dysphagia, and dyspnea (7 –9). A consistent proportion of these patients are hypothyroid, due to coexistent autoimmune thyroiditis, and the lymphomatous nodule appears as a cold area at thyroid scintiscan (10,11).
Thyrotoxicosis associated with thyroid lymphoma is exceedingly rare with only a few case reports (12) or brief comments in large series. The etiology of thyrotoxicosis in one case was thought to be Graves' disease (13), while in another there was a low radioiodine uptake consistent with thyroiditis (14). A patient with acquired immunodeficiency syndrome was reported in whom severe thyrotoxicosis was caused by the extensive destruction of normal thyroid tissue by an infiltrating anaplastic large cell lymphoma (4). In other patients the causes of thyrotoxicosis were not elucidated.
Our patient presented with a pathological fracture of the bone, a rare localization for lymphomas. Because of his diffuse disease, which also involved the thymus, it is not possible to determine whether he had primary thyroid lymphoma or spread of lymphoma from another site. He did not have a history of autoimmune thyroiditis, his tests for anti-thyroid antibodies were negative, and there was no inflammatory infiltrate of the thyroid. Laboratory and scintigraphic findings were consistent with the diagnosis of toxic adenoma. The remission of hyperthyroidism after methimazole treatment further confirms the diagnosis of a hyperfunctioning thyroid nodule that had been selectively infiltrated by a Burkitt-like lymphoma.
Burkitt-like lymphoma is a rare entity accounting for about 5% of all lymphomas. The onset of the disease is frequently characterized by a massive extranodal involvement (15) with high-grade behavior. To our knowledge, there has been only one case of Burkitt-like lymphoma of the thyroid, which was previously described in a three decades series of thyroid lymphomas (16).
In summary, this is the first description of an aggressive Burkitt-like lymphoma that infiltrated a hyperfunctioning thyroid adenoma, thus presenting as a hot nodule at thyroid scintiscan. In our patient there was no humoral or histological evidence of thyroid autoimmunity, thus suggesting a metastatic seeding of the lymphoma within the hyperfunctioning thyroid nodule. According to the recently delivered American Thyroid Association management guidelines for patients with thyroid nodules, hyperfunctioning thyroid nodules do not deserve FNAC (17). However, as highlighted by the present case report, performing FNAC of a thyroid nodule should be always considered in the clinical context of a metastatic disease of unknown origin or when, in spite of the hot appearance of the nodule, there are US signs suggesting malignancy.
Disclosure Statement
The authors declare that they have nothing to disclose.