
Abstract
Background:
Graves' disease (GD) is caused by thyrotropin (TSH) receptor antibodies (TSHRAbs) that bind to TSHR and activate thyrocytes. The measurement of TSHRAbs therefore has been used to assist in the diagnosis and management of GD.
Methods:
In this study, we evaluated the clinical significance of a newly developed bioreporter assay for the detection of TSHRAbs (Thyretain™). The Thyretain bioreporter assay utilizes a chimeric receptor (Mc4), in which residues 262–335 of TSHR are replaced with a rat lutropin-choriogonadtropin receptor segment. This bioreporter is designed to specifically detect stimulating TSHRAbs (Mc4-TSHRAbs).
Results:
The Mc4-TSHRAb level of sera obtained from 110 normal healthy controls, 103, 99, and 50 patients with untreated GD, painless Hashimoto's thyroiditis (PT), and subacute thyroiditis (SAT) were 27.3% ± 11.3%, 327.8% ± 105.9%, 48.9% ± 48.5%, and 24.9% ± 13.4%, respectively. Compared with the Mc4-TSHRAb levels of patients with PT and SAT, and normal healthy controls, the Mc4-TSHRAb levels of untreated GD patients were significantly higher (p < 0.01). The sensitivity and specificity of the Thyretain bioreporter assay for GD and PT were 95.1% and 96.0%, respectively, at the optimal cut-off value of 128%. Measurement of TSHRAbs with a bioassay that uses porcine thyroid cells (TSH-stimulating antibody [TSAb]) showed a positive correlation (r = 0.472, p < 0.001) with the Thyretain assay for untreated GD, and strong positive correlation (r = 0.821, p < 0.001) for the entire untreated GD, PT, and SAT population. The positive rate of Mc4-TSHRAbs for GD was significantly higher than that of TSAb (95.1% vs. 89.3%, p < 0.05) and the negative rate of PT by Mc4-TSHRAbs was also significantly higher than that of TSAb (96.0% vs. 86.9%, p < 0.01). As a result, Mc4-TSHRAbs showed statistically better (p < 0.01) diagnostic accuracy in differentiating GD from PT than TSAb.
Conclusions:
These data suggest that the Thyretain bioreporter assay with a chimeric TSHR (Mc4) is more useful in the differential diagnosis of GD from PT than the bioassay with wild-type TSHR on porcine thyroid cells.
Introduction
Materials and Methods
Patients sera
Included in this study were 103 patients with untreated GD (mean age, 40 ± 14 years; 14 men, 89 women), 99 with painless Hashimoto's thyroiditis (PT; 41 ± 13 years; 6 men, 93 women), and 50 with subacute thyroiditis (SAT; 49 ± 11 years; 1 men, 49 women). GD, PT, and SAT diagnoses were based on clinical data and findings, power Doppler sonography, and thyroid uptake of Tc-99m. The study was approved by the Committee for Medical Research Ethics of Kamijo Thyroid Research Institute and Kamijo Thyroid Clinic. All patients were informed of the purpose of this study. Sera of 110 normal healthy controls (age range 6–82 years; 25 men, 85 women) were obtained from subjects referred because of suspected goiter on palpation during routine checkup. All controls were euthyroid, were thyroid autoantibody negative, and had normal thyroid volumes measured by thyroid sonography. All serum samples were stored at −20°C.
Mc4-TSHRAb assay
Mc4-TSHRAbs in patient sera were measured with the Thyretain bioreporter assay according to the manufacturer's instructions (Diagnostic Hybrids, Inc., Athens, OH). This bioreporter assay is specific to stimulating TSHRAb activation due to the chimeric receptor expressed on the CHO cells. Stimulating TSHRAb specificity is conferred by a chimeric receptor in which a small region of the C-terminus TSHR (amino acids 262–335) is substituted with amino acids, 261–329 of the rat LH-CG receptor (Mc4). When stimulating TSHRAbs in the patient sera bind to the chimeric receptors on the CHO cells, the G protein receptor is activated. Subsequently, detachment of the α subunit from the βγ complex activates adenylate cyclase through the effector to increase intracellular cAMP. The cAMP induces activation of the promoter containing a cAMP-regulated enhancer upstream of the luciferase gene. The luciferase activity, measured as relative light units, is determined in cell lysates with a luminometer in an enzymatic reaction containing luciferin (Fig. 1). Mc4-TSHRAbs was assayed as follows. Serum samples were diluted 11-fold with reaction buffer, and 100 μL aliquot was added to a well of a 96-well microplate, which was confluent with CHO cells expressing chimeric receptors, together with 100 μL of reaction buffer. The plate was incubated at 37°C, 5% CO2 for 3 hours. After discarding the solution, 75 μL of cell lysis solution containing luciferin substrate was added to each well. Chemiluminescence intensity was measured 10 minutes after the addition of substrate solution. All assays were performed in triplicate. The Mc4-TSHRAb level of each patient serum was expressed as percentage of luciferase production compared to that of the reference control.
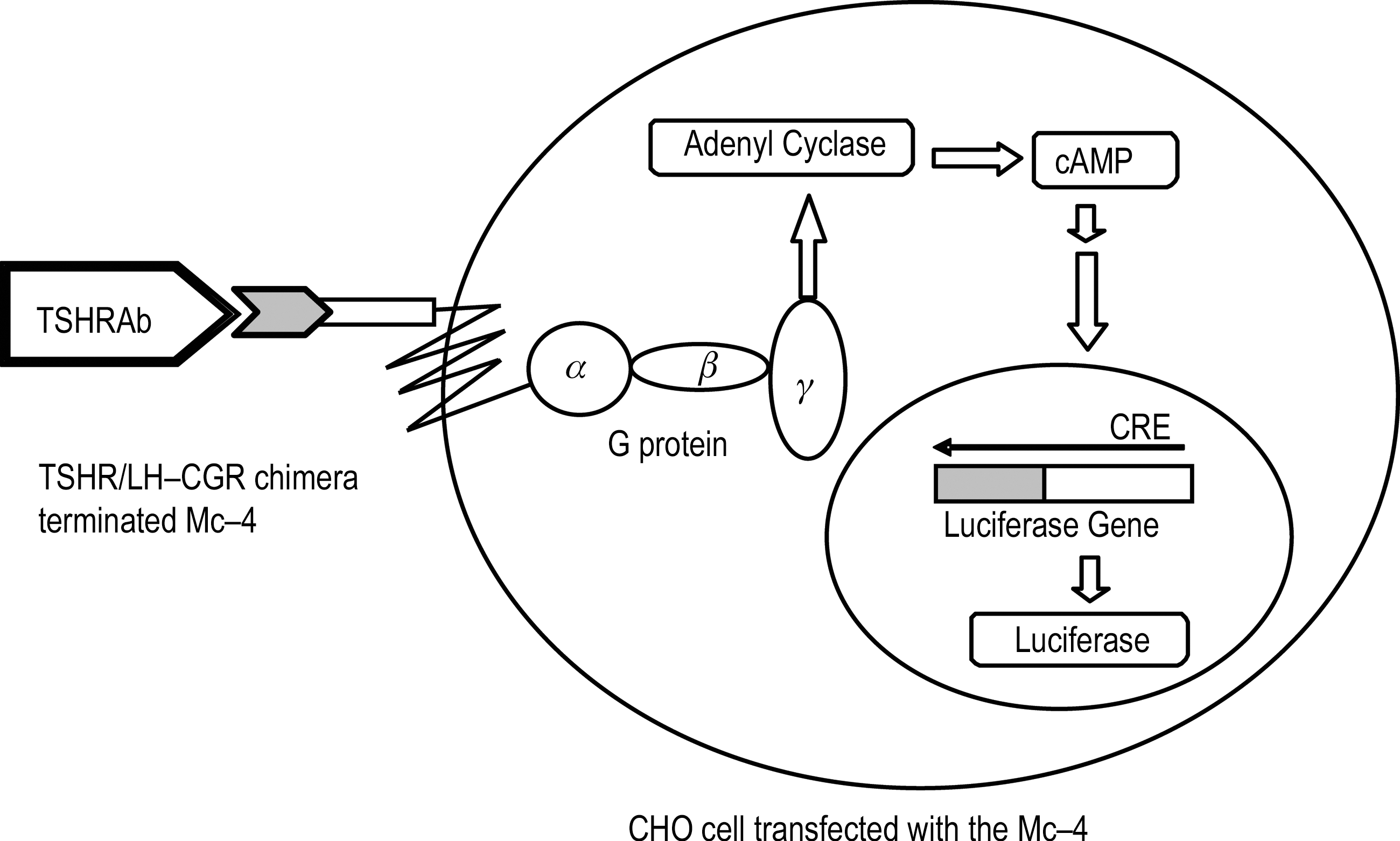
The principle of Mc4-TSHRAb bioreporter assay. Mc4-TSHRAb bioreporter assay detects serum-stimulating TSHRAbs using Chinese hamster ovary cells transfected with a chimeric human TSHR (Mc4). Mc4-TSHRAb binding to the chimeric TSHR induce a signaling cascade resulting in increased production of luciferase. Mc4-TSHRAb level in patient sera is determined by measuring the increase production of luciferase. TSHRAbs, thyrotropin receptor antibodies.
TSH-stimulating antibody assay
TSHRAbs were also assayed by measuring cAMP production in cultured porcine thyroid cells (TSH-stimulating antibodies [TSAb]). TSAb activity was measured according to the previously reported method (13). The TSAb level of each patient serum was expressed as percentage of cAMP production compared to that of normal control serum. The cut-off value of TSAb was 180%.
Statistical analysis
Statistical analysis of proportion was performed by Delta test. Correlations were assessed by Spearman's test. The optimal cut-off point was obtained by receiver operating characteristic (ROC) analysis and the area under the curve (AUC) was also calculated. The AUCs of the two different assays were evaluated if they were significantly different by Delta test.
Results
Intraassay and interassay variability of the bioreporter assay
To evaluate intra- and interassay variability of the Thyretain bioreporter assay, we measured Mc4-TSHAb levels of three different serum samples (N, R, and P). Intraassay coefficient of variation (CV) of each serum samples was 5.4%, 4.7%, and 3.0%, respectively (Table 1a). Interassay CV of each serum samples was 34.7%, 6.9%, and 11.8%, respectively (Table 1b). A relatively large CV (34.7%) was observed with serum sample N, but this was related to the low mean value of this serum sample.
CV, coefficient of variation; SD, standard deviation.
Estimation of the cut-off value of Mc4-TSHRAbs by the ROC curve analysis
To estimate the optimal Mc4-TSHRAb cut-off value, we performed ROC analysis of Mc4-TSHRAb levels with untreated GD and PT. The ROC analysis suggested 128% of Mc4-TSHRAb level as the optimal cut-off value (Fig. 2). The sensitivity and specificity at the optimal cut-off value were 95.1% and 96.0%, respectively.

ROC analysis for estimation of Mc4-TSHRAb cut-off value. From the ROC analysis with untreated GD (n = 103) and PT (n = 99), the Mc4-TSHRAb cut-off value was estimated to be 128%. GD, Graves' disease; PT, painless Hashimoto's thyroiditis; ROC, receiver operating characteristic.
Method comparison
The correlation between Mc4-TSHRAb and TSAb level was shown in Figure 3 for 103 untreated GD (Fig. 3a) and all of untreated GD, PT, and SAT population (Fig. 3b). We observed a positive correlation (r = 0.472, p < 0.001) in a comparison of untreated GD (Fig. 3a) and a strong positive correlation (r = 0.821, p < 0.001) in a comparison of all of untreated GD, PT, and SAT population (Fig. 3b).

Correlation between Mc4-TSHRAb and TSAb values. A significant positive correlation was observed between log (TSAb) and Mc4-TSHRAbs in the 103 patients with untreated GD (
Clinical evaluation
Mc4-TSHRAb levels in the various groups
Mc4-TSHRAb levels of sera obtained from 103, 99, and 50 patients with untreated GD, PT, and SAT, and from 110 normal healthy controls were 327.8% ± 105.9%, 48.9% ± 48.5%, 24.9% ± 13.4%, and 27.3% ± 11.3%, respectively. Mc4-TSHRAb level of untreated GD was significantly higher (p < 0.01) than those of normal healthy control, PT, or SAT. Out of 103 untreated GD, 98 cases (95.1%) were positive. In contrast, out of 99 PT, only 4 cases (4.0%) were positive and the remaining 95 cases (96.0%) were negative. Among the 50 cases of SAT, all were negative (Fig. 4).

Distribution of serum Mc4-TSHRAb value in normal healthy control and various thyroid diseases. The mean value and standard deviation of Mc4-TSHRAbs (*) in 110 normal healthy controls (▴), 103 patients with untreated GD (○), 99 patients with PT (•), and 50 patients with SAT (▵) were 27.3% ± 11.3%, 327.8% ± 105.9%, 48.9% ± 48.5% and 24.9% ± 13.4%, respectively.
Comparison with diagnostic performance of Mc4-TSHRAbs and TSAb
Using the ROC analysis with untreated GD as positive and PT as negative references, we compared the diagnostic performance of Mc4-TSHRAbs and TSAb. Mc4-TSHRAbs showed superior diagnostic performance, p < 0.01 (Fig. 5). The positive rate 95.1% of Mc4-TSHRAbs in patients with untreated GD was significantly higher than 89.3% for TSAb (p < 0.05). Moreover, the negative rate 96.0% of Mc4-TSHRAbs in patients with PT was significantly (p < 0.01) higher than 86.9% for TSAb (Table 2). As a result, Mc4-TSHRAbs showed higher diagnostic accuracy (p < 0.01) in differentiating GD and PT (Delta test).
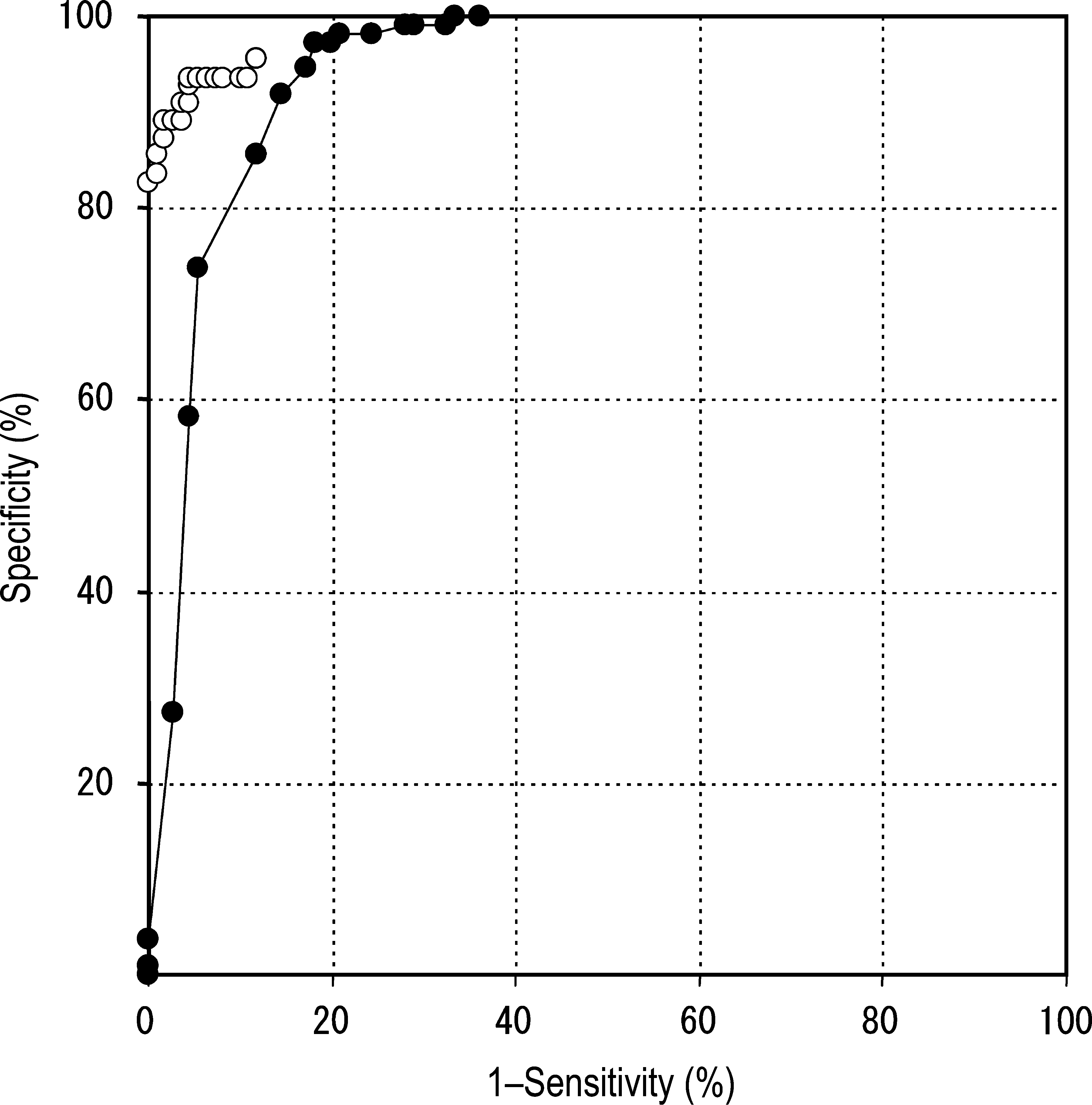
Comparison of the ROC analysis between Mc4-TSHRAbs and TSAb. The diagnostic performance of Mc4-TSHRAbs (○) or TSAb (•) in the detection of GD was evaluated using the ROC analysis with PT (n = 99) and untreated GD (n = 103). The area under the curve for Mc4-TSHRAbs (0.9883 ± 0.0064; mean ± standard error) was significantly larger than for TSAb (0.9469 ± 0.0105, p < 0.01).
In untreated GD, the positive rate of Mc4-TSHRAbs was significantly higher than that of TSAb (p < 0.05) by Delta test. In PT, negative rate of Mc4-TSHRAbs was significantly higher than that of TSAb (p < 0.001) by Delta test. Diagnostic accuracy of Mc4-TSHRAbs as a result was significantly higher than that of TSAb (p < 0.01) by Delta test.
GD, Graves' disease; PT, painless Hashimoto's thyroiditis; TSAb, thyrotropin-stimulating antibody; TSHRAbs, thyrotropin receptor antibodies.
Discussion
Most GD sera have two types of TSHRAbs, stimulating TSHRAbs, which bind to TSHR and elevate cAMP levels in thyroid cells, and nonstimulating TSHRAbs, which bind to the TSHR but do not elevate cAMP levels in thyroid cells (TSBAbs). TSBAbs in GD sera also can be classified based on their target epitopes on the TSHR. There are TSBAbs that bind to epitopes on N-terminus of the extracellular domain of TSHR and those that bind to epitopes on the C-terminus of the extracellular domain of TSHR (9). The TSBAbs associated with the C-terminal epitopes appear to be able to block stimulating TSHRAbs as well as TSH activity, whereas the TSBAbs associated with the N-terminal epitopes appear to be able to block only TSH activity (10,11). These findings suggest that stimulating TSHRAbs detected by a bioassay using porcine thyroid cells would be interfered with by the TSBAbs associated with the C-terminal epitopes of TSHR. Further, these findings also suggest that a C-terminus-substituted chimeric receptor with an intact N-terminus, which is critical for expressing stimulating TSHRAbs, would be more useful for detecting stimulating TSHRAbs in GD sera.
Recently, a bioreporter assay (Thyretain) that is based on an Mc4 chimeric receptor (Mc4) was developed. Mc4 lacks residues on the C-terminus to which certain TSBAbs bind. The Mc4 receptor is known to strongly decrease measurable high-affinity TSH binding and TSH-induced cAMP stimulation, although there is no significant effect on stimulating TSHRAbs' activity (14). The ROC analysis performed with untreated GD and PT showed that the Thyretain bioreporter assay had high sensitivity and specificity in the diagnosis of GD and PT (sensitivity and specificity were 95.1% and 96.0% respectively, at an optimal cut-off of 128%). The Mc4-TSHRAb levels of untreated GD detected by the Thyretain bioreporter assay were significantly higher than those of normal healthy controls and PT or SAT patients, which demonstrates the clinical significance of the bioreporter assay. In a comparison between the bioreporter assay and a bioassay that uses cultured porcine thyroid cells, we observed a significant correlation between Mc4-TSHRAbs and TSAb of untreated GD. On the basis of the report of Grasso et al., in only 25% of GD sera, TSBAbs associated with the C-terminal epitopes appear to be able to block stimulating TSHRAb as well as TSH activity (9). This might be a reason why a significant correlation between Mc4-TSHRAbs detected by Mc4 chimera and TSAb detected by wild-type porcine TSHR was noted. However, comparision of the AUC of the ROC analysis showed the superiority of Mc4-TSHRAbs compared with TSAb for correctly diagnosing untreated GD. The positive rate of 95.1% of Mc4-TSHRAbs in patients with untreated GD is significantly higher than the 89.3% of TSAb (p < 0.05). These findings may result from the difference between TSHRAb detection by the Mc4 chimeric TSHR and detection by wild type of TSHR.
TSHRAbs have been also measured using an assay based on the inhibition of TSH binding to TSHR (TBII). However, it has not been clear whether TSHRAbs measured by stimulation of cAMP is the same as TSHRAbs measured by TBII and whether TSHRAbs and TSH are binding to the same site of TSHR. There is some evidence that indicates that both stimulating TSHRAb and TSBAbs are heterogeneous (9,11). Therefore, it would be interesting to compare the Mc4-TSHRAbs of GD sera detected with the Thyretain bioreporter assay that uses the Mc4 chimeric receptor, with TSAb detected by wild type by TSHR and TBII. These studies are ongoing. Further Mc4-TSHRAbs should be evaluated for other clinical applications such as monitoring during ATD treatment, prognostic assessment after ATD treatment, and correlation with Graves' eye disease. It would also be worthwhile to determine whether Mc4-TSHRAb has prognostic value for predicting neonatal hyperthyroidism in pregnant patients with GD.
In summary, our result suggests that the Thyretain bioreporter assay using Mc4 chimeric TSHR is a significantly better test for the measurement for TSHRAbs in GD sera than the bioassay that uses a wild-type porcine TSHR.
Footnotes
Disclosure Statement
Kamijo Thyroid Research Institute has received research grants from Yamasa Corporation. H.M., T.U., and K.T. are employed by Yamasa Corporation. Yamasa Corporation consulted for Diagnostic Hybrids, Inc. G.J.K. has served as an unpaid advisor for research and manuscript preparation.