
Abstract
Background:
Iodide transport defect (ITD) is an infrequent condition associated with congenital dyshormonogenetic goiter due to mutations in the Na+/I− symporter (NIS) gene transmitted in an autosomal recessive manner. Herein, we describe a patient with ITD and discuss the features important for the diagnosis, focusing on whether or not measuring the saliva/serum radioactive iodide ratio is useful.
Summary:
A 42-year-old Japanese man attended our hospital in 2010. At that time, he had been off L-thyroxine for several months. He had no obvious mental retardation. His parents were cousins and his sister also had a goiter. Since thyroid dyshormonogenesis could not be ruled out, thyroid function tests, scintigraphy, and ultrasonography were performed. The results showed marked hypothyroidism with a high thyroglobulin level of 627 ng/mL. The results for thyroglobulin antibody and thyroid peroxidase antibody were both negative. Ultrasonography showed an enlarged thyroid gland. Neither the thyroid nor the salivary gland was visualized by 99mTcO4 − scintigraphy. Therefore, we performed genetic testing for the NIS gene without measuring the saliva/serum radioactive iodide ratio. A homozygous mutation, T354P, was identified in the NIS gene. On the basis of this finding, we could make the definitive diagnosis of ITD due to an NIS mutation.
Conclusions:
We recommend confirming the presence of the thyroid by ultrasonography of the neck first and then performing 99mTcO4 − scintigraphy. If neither the salivary gland nor the thyroid is visualized, screening for NIS mutations should be undertaken. This approach obviates the need to undertake measurement of the saliva/serum radioactive iodide ratio to diagnose ITD.
Introduction
Patient
The patient was a 42-year-old Japanese man from Kumamoto Prefecture who had been on levothyroxine sodium (LT4) since around 23 years of age for hypothyroidism. Thyroid function tests were performed when the patient attended our clinic at 32 years of age, and these tests revealed a thyroid-stimulating hormone (TSH) level of 0.07 μU/mL, free thyroxine of 1.86 ng/dL, and free triiodothyronine of 3.45 pg/mL, indicating TSH suppression. On ultrasonography, the thyroid gland was small but contained several nodules. The patient was then followed up with a prescription of oral LT4 at 200 μg/day, but his compliance was poor. In January 2010, at 42 years of age, the patient reattended our hospital. At that time, he had been off LT4 for several months. On that occasion, we reevaluated the diagnosis. The patient was 152.0 cm tall and weighed 63.0 kg. He had no obvious mental retardation and worked in the construction industry. Further history taking disclosed that his parents were cousins and his sister also had a goiter. Since thyroid dyshormonogenesis could not be ruled out, thyroid function tests, scintigraphy, and ultrasonography were performed. The results showed marked hypothyroidism with a TSH level of 676 μU/mL (normal range: 0.22–3.30 μU/mL), free thyroxine of 0.15 ng/dL (normal range: 0.9–1.8 ng/dL), and free triiodothyronine of 0.81 pg/mL (normal range: 2.2–4.30 pg/mL). The laboratory findings also showed a high thyroglobulin level of 627 ng/mL (normal: below 35 ng/mL). The results for both thyroglobulin antibody and thyroid peroxidase antibody were negative. On ultrasonography, the thyroid volume was shown to have increased and many nodules were noted within the gland, as shown in Figure 1. Neither the thyroid nor the salivary gland was visualized by 99mTcO4 − scintigraphy, as shown in Figure 2. The finding that neither the thyroid nor the salivary gland was visualized on 99mTcO4 − scintigraphy despite the presence of thyromegaly was important, strongly suggesting ITD (4). Therefore, we performed genetic testing for the NIS gene with the patient's consent. A homozygous mutation, T354P, was identified in the NIS gene (Fig. 3). On the basis of this finding, we made the definitive diagnosis of ITD due to an NIS mutation.
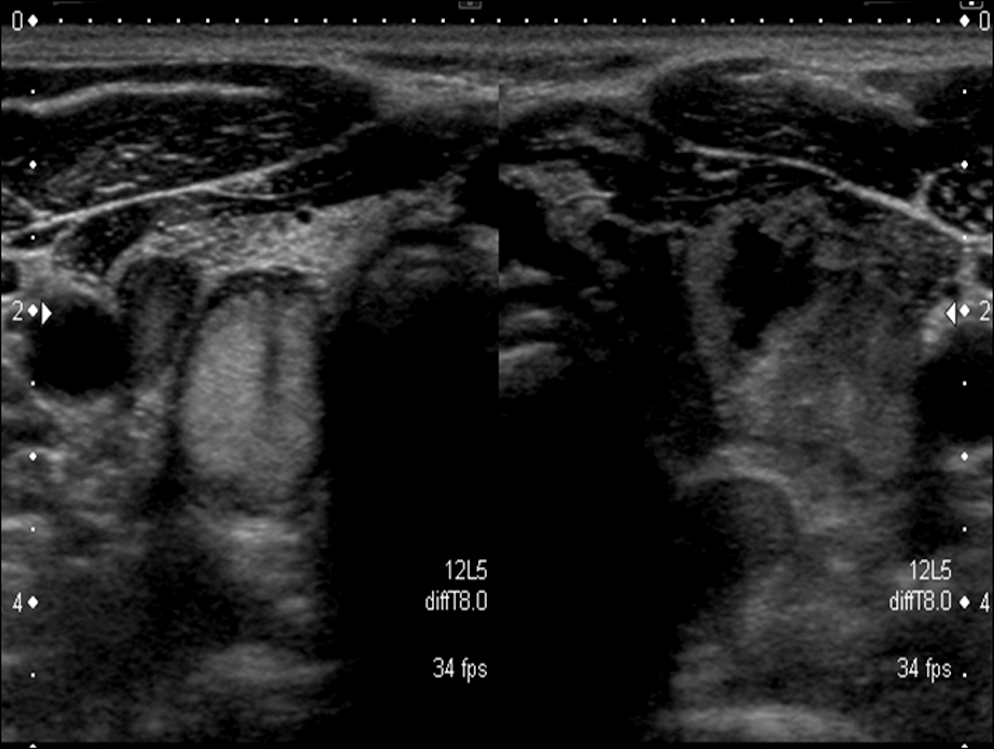
Transverse ultrasonographic image: enlarged goiter with multiple nodules. The right lobe measures 1.99 × 1.70 × 4.99 cm, and the left lobe 2.47 × 2.22 × 5.36 cm.
99mTcO4 − scintigram. Neither the thyroid nor the salivary gland was visualized.

Electropherogram. The patients were shown to be homozygous for the T354P mutation [Thr354→Pro (ACA→CCA) (arrow)] in the NIS gene.
Discussion
Is it essential to determine the saliva/serum radioactive iodide ratio, a conventional diagnostic method, for the diagnosis of ITD? The NIS protein exists not only in the thyroid but also in the salivary gland, gastric mucosa, lactating mammary gland, choroid plexus, and ciliary body of the eye (2). Further, the NIS protein transports iodide and 99mTcO4 − in the same manner (6). Taking these facts into consideration, if neither the thyroid nor the salivary gland is visualized by 99mTcO4 − scintigraphy, abnormalities in the NIS protein are strongly suggested, unless the salivary gland has been destroyed due to a disease such as Sjögren's syndrome (7). If the above finding is obtained, it is reasonable to immediately screen for NIS mutations to make a definitive diagnosis. Figure 4a shows a scintigram from a patient with painless thyroiditis, in which the thyroid was not visualized but the salivary gland was distinctly observed. Figure 4b is a scintigram from a patient with Graves' disease whose 99mTcO4 − uptake was extremely high. In this case, the salivary gland was not visualized, because 99mTcO4 − uptake by the thyroid had been increased.

99mTcO4
− scintigram.
We recommend first confirming the presence of the thyroid by ultrasonography of the neck and then performing 99mTcO4 − scintigraphy. If neither the salivary gland nor the thyroid is visualized, then screening for NIS mutations should be immediately undertaken. According to Kosugi et al., there may be many patients in whom ITD has not been diagnosed (4). The diagnostic procedure that we have presented herein allows rapid and accurate diagnosis of ITD due to abnormalities in the NIS gene and could thereby provide further insights into not only ITD but also the NIS gene and its product.
Disclosure Statement
The authors declare that no competing financial interests exist.