
Abstract
Background:
Lymphoma involving the thyroid gland is rare. Diffuse large B-cell lymphoma and mucosa-associated lymphoid tissue lymphoma are the two most common histologic subtypes of primary thyroid lymphoma. Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) presenting initially as a thyroid abnormality is extremely rare, with very few reported cases in the literature.
Summary:
We report a case of a patient with a long history of Hashimoto's thyroiditis and goiter who presented with a recent enlargement of her thyroid gland. The sonographic finding of a distinct thyroid nodule in the heterogeneous background of chronic lymphocytic thyroiditis led to the performance of a fine-needle aspiration biopsy and flow cytometry, with a high index of suspicion for thyroid lymphoma. Subsequent surgical removal of the thyroid gland, prompted by the patient's history of head and neck radiation, confirmed the diagnosis of CLL/SLL. The patient's systemic illness was recognized only after the management of her thyroid disease. Although thyroiditis has long been associated with lymphoma arising in the thyroid gland, CLL/SLL involving the thyroid has not been linked to chronic lymphocytic thyroiditis. Therefore, the patient also had coexisting thyroiditis.
Conclusions:
Due to the rarity of thyroid lymphomas, our experience in the detection and management of this disease is limited. Primary thyroid lymphoma should be suspected in a patient with a history of chronic lymphocytic thyroiditis presenting with a rapidly enlarging neck mass. The initial diagnostic method for thyroid lymphoma should consist of a fine-needle aspiration biopsy with the use of ancillary techniques such as flow cytometry and immunohistochemistry for improved diagnostic accuracy. Although controversial, the treatment of thyroid lymphoma is typically guided by the histologic subtype and extent of disease. CLL/SLL is one of the rarest subtypes of lymphoma that can involve the thyroid gland. Diagnosis of this entity is difficult, particularly before the recognition of systemic involvement, requiring the expertise of a multidisciplinary team for early detection and optimal management.
Introduction
CLL/SLL is a low-grade indolent neoplasm characterized by small mature B lymphocytes in the peripheral blood, bone marrow, lymph nodes, and other tissues (3,9). Historically, SLL was considered a different disease entity from CLL. However, the World Health Organization classification of hematologic malignancies now recognizes CLL and SLL as different clinical manifestations of the same disease, with the term SLL applied in cases with tissue involvement (10,11). The presence of CLL/SLL cells in the thyroid gland is most likely due to a secondary involvement by a systemic disease (9,11). The reported incidence of CLL/SLL involving the thyroid is extremely low, representing ∼3%–4% of all thyroid lymphomas (2,4,8,12). Further, to the best of our knowledge, there have only been two case reports in the literature, both cases with simultaneous occurrence of other thyroid carcinomas (11,13). We report a rare case of CLL/SLL presenting initially in the thyroid gland, and the presence of systemic involvement was identified only after the workup of the patient's thyroid disease.
Patient Presentation
A 67-year-old woman with a 7-year history of hypothyroidism and goiter presented with a recent enlargement of her thyroid gland. She was asymptomatic and had no family history of endocrine diseases. However, she had a questionable history of radiation to her face as a teenager for acne. The patient's microsomal antibody level was 2217.7 IU/mL (normal value, <5.0) and thyroid-stimulating hormone level was 1.32 mIU/L (normal range, 0.4–5.5) on 50 mcg/day of levothyroxine. Physical examination revealed a visible bilateral goiter that was soft on palpation. Sonographically, the thyroid was heterogeneous in appearance, consistent with thyroiditis. Further, the thyroid gland was quite large, with the right lobe measuring 4.45 × 2.99 × 8.25 cm and the left lobe measuring 3.65 × 2.25 × 7.45 cm (Fig. 1). Located near the midportion of the left thyroid lobe, there was a well-circumscribed hyperechoic nodule measuring 2.56 × 1.18 × 2.02 cm with no hypervascularity or internal calcifications (Fig. 2). Ultrasound-guided fine-needle aspiration biopsy (FNAB) focused into this nodule was performed to rule out thyroid cancer cytologically. Additional aspirates were obtained for flow cytometry to rule out lymphoma. Cytology demonstrated benign follicular epithelium with a background of small mature lymphoid cells, consistent with chronic lymphocytic thyroiditis (Fig. 3). Flow cytometry identified a small population of monotypic B-cell lymphocytes that expressed CD19 and CD5 and were kappa light chain restricted. CD23 was equivocal. In contrast to the cytology results, the flow cytometry findings were concerning for possible PTL.
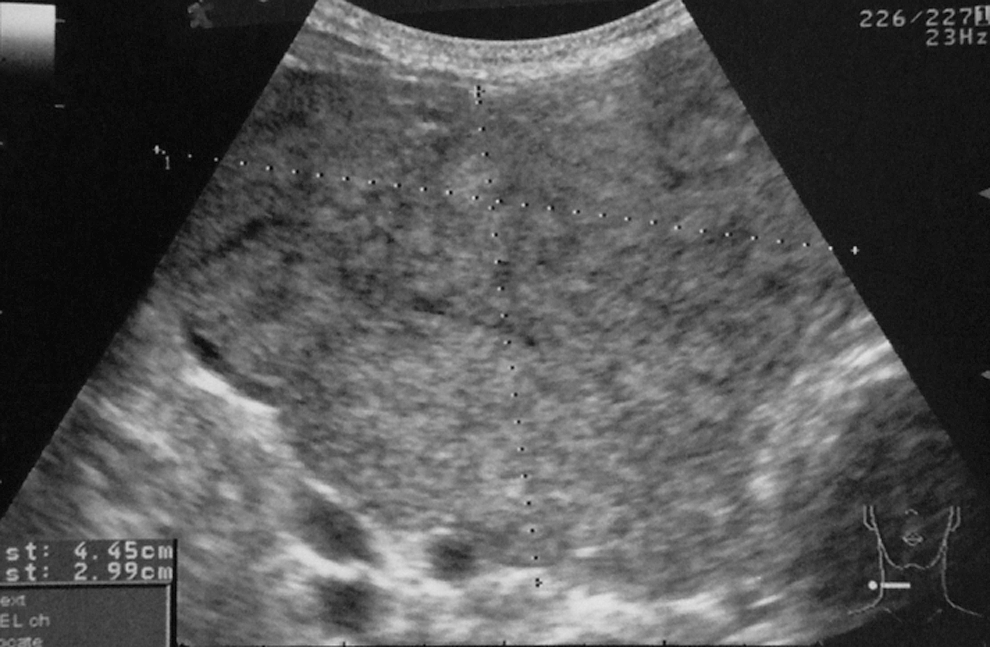
An enlarged right thyroid lobe with coarse hypoechoic appearance on ultrasound, typically seen with Hashimoto's thyroiditis.
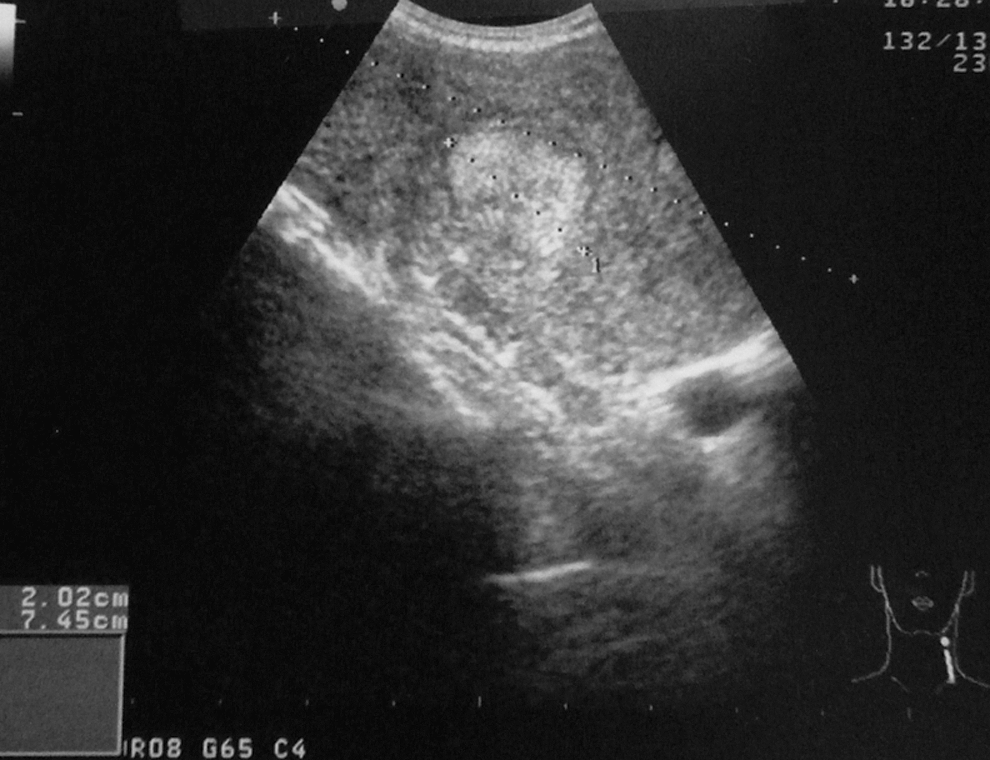
Ultrasonographic image showing a transverse view of the left thyroid lobe and nodule. The thyroid has a coarse heterogeneous appearance, whereas the nodule is hyperechoic.
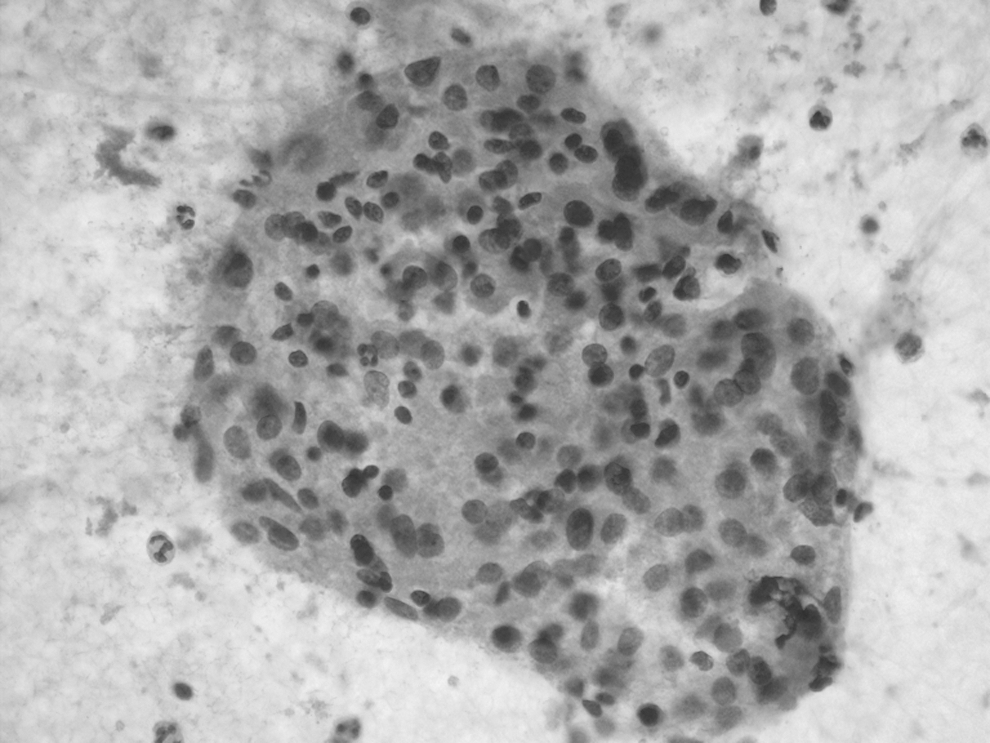
Aspirate smears demonstrate flat sheets of Hürthle cells with admixed lymphocytes, consistent with chronic lymphocytic thyroiditis (Papanicolaou stain, 20 ×).
The patient underwent a total thyroidectomy due to her history of head and neck radiation and its associated risk of differentiated thyroid cancer. A large, soft thyroid gland was removed without difficulty. Pathology revealed an atypical lymphoid infiltrate diffusely involving the thyroid parenchyma, which was composed of small mature lymphocytes that were immunohistochemically positive for CD20 and CD5, and negative for CD3, CD10, and cyclin-D1 (Fig. 4). These findings were most consistent with a diagnosis of CLL/SLL.

(
Postoperatively, the patient was referred to medical oncology for further workup of her lymphoma. Laboratory evaluation did not show an elevated absolute lymphocyte count, but flow cytometry of peripheral blood demonstrated a monotypic B-lymphocyte population expressing CD19, CD20, dim CD5, dim CD23, and kappa light chains. Computed tomography of the chest, abdomen, and pelvis did not reveal any evidence of lymphoma. However, the patient's bone marrow aspiration and biopsy demonstrated multiple large interstitial lymphoid aggregates with a nodular pattern, composed of small mature lymphocytes. Immunohistochemical stains demonstrated that the lymphoma cells were positive for CD5, CD20, and CD79a, but negative for CD3. Overall, the morphologic and immunophenotypic findings were consistent with bone marrow involvement by CLL/SLL. The patient currently remains asymptomatic from this disease, and she will continue to be monitored with blood counts and physical examination every 3 months and repeat imaging only if she becomes symptomatic or has new physical examination findings.
Discussion
PTL is a rare malignancy, with reports of DLBCL and MALT lymphoma comprising most of the literature. The relationship between Hashimoto's thyroiditis and PTL is well-known, as the vast majority of PTL arise in the background of chronic lymphocytic thyroiditis (9,12). Further, the association between Hashimoto's thyroiditis and MALT lymphoma has gained much attention. The hypothesis that chronic antigenic stimulation of lymphocytes by thyroiditis leads to the development of malignant clones has been proposed (2,5,12). However, the exact mechanism of this malignant transformation remains unknown, and the suggested theory is still controversial.
CLL/SLL is one of the most uncommon subtypes of lymphoma that can involve the thyroid gland, comprising only 3%–4% of all thyroid lymphomas (2,4,8,12). The typical diagnosis of CLL/SLL requires the presence of >5000 small mature B lymphocytes per microliter in the peripheral blood (14). Flow cytometry will demonstrate clonality, as determined by kappa or lambda light chain restriction, and CLL/SLL cells are typically positive for CD5, CD23, CD19, and CD20 (14). There have been two case reports of CLL/SLL involving the thyroid gland, both of which describe its presence with simultaneous occurrence of other thyroid cancers (11,13). The first report describes a patient with both medullary and papillary carcinoma of the thyroid. The patient's cervical lymph nodes contained papillary thyroid carcinoma metastases, as well as a concomitant small B-cell lymphocytic lymphoma (13). Similar to our patient, the diagnosis of systemic CLL/SLL was unknown at initial presentation. However, unlike our report, CLL/SLL involved the cervical lymph nodes, not the thyroid gland, and there was no clinical suspicion for lymphoma during the workup of the patient's thyroid disease. The second report also describes CLL/SLL occurring concurrently with papillary thyroid carcinoma in the thyroid (11). This patient, unlike ours, presented with known systemic CLL/SLL. An ultrasound-guided FNAB was performed, revealing a diagnosis of papillary thyroid cancer with an atypical lymphoid infiltrate, suspicious for lymphoma.
Our case presentation is different in that the patient's clinical history and sonographic findings led to a workup for thyroid lymphoma and, ultimately, the diagnosis of systemic CLL/SLL. The patient's history of Hashimoto's thyroiditis and recent enlargement of her thyroid mass are common manifestations of PTL. Although this presentation may have been sufficient to have a suspicion for thyroid lymphoma, the presence of a distinct thyroid nodule in the background of chronic lymphocytic thyroiditis led to the performance of an FNAB with flow cytometry, confirming our suspicion. The sonographic appearance of PTL has most commonly been described as a pseudocystic, hypoechoic mass; however, these characteristics have not been universal (15). Fortunately for our patient, the presence of a well-defined thyroid nodule, in addition to her clinical history, led to the initial workup for thyroid lymphoma that included FNAB with flow cytometry. The patient then underwent surgical resection, prompted by the history of head and neck radiation, which is associated with a significantly increased risk of differentiated thyroid cancer (16). Nonetheless, the surgical pathology was most consistent with the diagnosis of CLL/SLL with no evidence of other epithelial neoplasms. Although thyroiditis has long been associated with lymphoma arising in the thyroid gland, CLL/SLL involving the thyroid has not been linked to chronic lymphocytic thyroiditis. Therefore, this patient also has coexisting thyroiditis.
In the past, the majority of PTL were diagnosed incidentally after surgical removal of the thyroid gland for other indications (17). Thyroid lymphoma can be very difficult to distinguish from Hashimoto's thyroiditis on FNAB (5,17,18). Further, PTL and anaplastic carcinoma can present in a similar fashion, most often a patient with a rapidly enlarging neck mass (9,12,18). Currently, the value of FNAB has been emphasized, as the use of ancillary techniques such as flow cytometry, immunoglobulin gene rearrangements, and immunohistochemistry has improved diagnostic accuracy and obviated more invasive, open biopsy procedures (12,18). Numerous reports in the literature recommend FNAB with such ancillary studies as the first diagnostic tool for PTL. However, even using these techniques with FNAB, the diagnosis can remain uncertain. Therefore, open surgical biopsy continues to play an important role in the diagnosis of thyroid lymphomas, particularly when the treatment modality depends on the histologic subtype or when the diagnosis remains unclear (7,9,18).
The treatment of thyroid lymphoma is controversial. Thyroidectomy has traditionally been the mainstay of treatment, mostly due to the inability to preoperatively diagnose PTL (19). However, its role in the management of thyroid lymphoma has diminished in recent years, as the success of combined chemoradiation therapy has become evident (2,19). Although there have been no randomized controlled trials comparing multimodality versus single modality approach in PTL, the combination of locoregional radiation and chemotherapy (cyclophosphamide, doxorubicin, vincristine, and prednisone) is most often recommended and utilized for all DLBCL and MALT lymphomas extending beyond the thyroid gland (stages greater than IE) (1,2,7). Surgery or radiation therapy alone may be reasonable options for stage IE MALT and other less aggressive subtypes of lymphoma, when disease is confined to the thyroid gland, but this treatment modality remains controversial (2,4,7). Further, surgery may still play a crucial role in the management of patients with severe airway obstruction or compressive symptoms (2,15).
In conclusion, PTL is a rare disease that can pose diagnostic difficulty for clinicians. Even with ancillary techniques, a high index of suspicion for PTL is needed to allow clinicians to obtain adequate biopsy sampling and indicate to the pathologist the need to triage samples for special studies, such as flow cytometry. Good communication with the pathologist can therefore enhance diagnostic accuracy and dictate appropriate therapy. This case demonstrates one of the most uncommon subtypes of lymphoma, CLL/SLL, presenting initially in the thyroid gland, without prior knowledge of the patient's systemic disease. Unlike the other, more familiar subtypes of thyroid lymphoma, CLL/SLL involving the thyroid has not previously been associated with chronic lymphocytic thyroiditis. However, a patient with thyroiditis presenting with a rapidly enlarging thyroid gland should raise suspicion for thyroid lymphoma. An awareness of this rare disease entity can permit early detection and optimal treatment.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.