
Abstract
Background:
The presence of estrogen receptors (ERs) in both normal and neoplastic thyroid tissues has been demonstrated in numerous publications. Growth-stimulatory effects of estrogen on thyroid tissue have been postulated to account for the prevalence of thyroid cancers in premenopausal women. However, the role of ERs in mediating these effects is by no means clear-cut, and the significance of ER expression by thyroid carcinomas is currently unknown. This article reports a patient with papillary thyroid cancer and a rare profile of immunohistochemical markers.
Summary:
A 67-year-old woman underwent a total thyroidectomy for papillary thyroid carcinoma and received radioiodine therapy postoperatively. The patient presented 3 months postoperatively with an enlarging neck mass at the surgical site associated with compressive symptoms and vocal cord paralysis. The patient underwent modified radical neck dissection for debulking of the recurrent tumor, which was invading into the prevertebral fascia. Immunohistochemical analysis of the resected mass revealed positive staining for ER-alpha (ER-alpha) and for gross cystic disease fluid protein 15, both markers with specificities for mammary carcinomas. However, evaluation for a possible primary breast cancer was negative. This case represents an unusual presentation of a rapidly recurring papillary thyroid carcinoma masquerading immunohistochemically as a primary breast cancer. Although the existence of ER-positive thyroid cancer has been well established, the dramatic increase in ER expression between initial and recurrent tumors in this postmenopausal woman raises the question of the significance of these receptors to the progression of the disease. Further, this case is the first to our knowledge to document gross cystic disease fluid protein 15 expression by a primary thyroid carcinoma.
Conclusions:
This case highlights the need to further explore the possible ramifications of ER expression in thyroid malignancy.
Introduction
Patient Report
The patient is a 67-year-old woman who was referred to the Endocrine Surgery clinic at Tulane University Hospital with an enlarging mass at the site of a previously resected PTC. She had undergone a right thyroid lobectomy for benign multinodular goiter in 1995 and a completion thyroidectomy in 2009 after fine-needle aspiration biopsy of a palpable left thyroid nodule revealed evidence of papillary carcinoma. Surgical pathology from her completion thyroidectomy confirmed the diagnosis of PTC, T1N0M0 (stage I), with a background of Hashimoto thyroiditis. The surgeon reported that the malignant nodule was invading the recurrent laryngeal nerve, which needed to be resected. The surgical margins were positive for malignancy. The patient received radioiodine ablation (150 milliCuries) postoperatively. A subsequent whole-body 131I scan revealed expected uptake in the thyroid bed as well as physiologic uptake in the sinuses, liver, bladder, and bowel, without evidence of metastatic disease. Unfortunately, 3 months after the initial thyroidectomy, she noticed hoarseness and the sensation of a growing mass in her neck, at which time she was referred to the clinic. At that time, her review of systems was also significant for dysphagia, odynophagia, and dyspnea.
Direct laryngoscopy revealed evidence of complete paralysis of the left vocal cord with good movement of the right vocal cord. Computed tomography scans of the neck and chest with and without contrast showed a significantly large necrotic mass within the left thyroid bed extending into the anterior mediastinum along the trachea and left side of the esophagus (Fig. 1a, b). The findings were concerning for involvement of these structures with tumor. Fine-needle aspiration cytology of the mass confirmed a diagnosis of recurrent PTC. Due to the patient's significant symptomatology and positive documentation for recurrence, the decision was made to perform modified radical neck dissection on the side of the tumor.

Intraoperatively, a large, hard, fixed mass was found extending from the cricoid cartilage down into the anterior mediastinum and adherent to prevertebral fascia. The mass was dissected off the carotid artery. A branch of the already inactive left recurrent laryngeal nerve was found to be encased in tumor, and was sacrificed as part of an en bloc resection. However, the mass involved the prevertebral fascia posteriorly on the left side; a remnant of tumor was not resectable and was therefore left in situ in this area and marked with clips. A central lymph node dissection and selective lateral neck dissections of levels 2, 3, and 4 on the left side were performed. Finally, a tracheostomy was placed due to concerns about airway compromise.
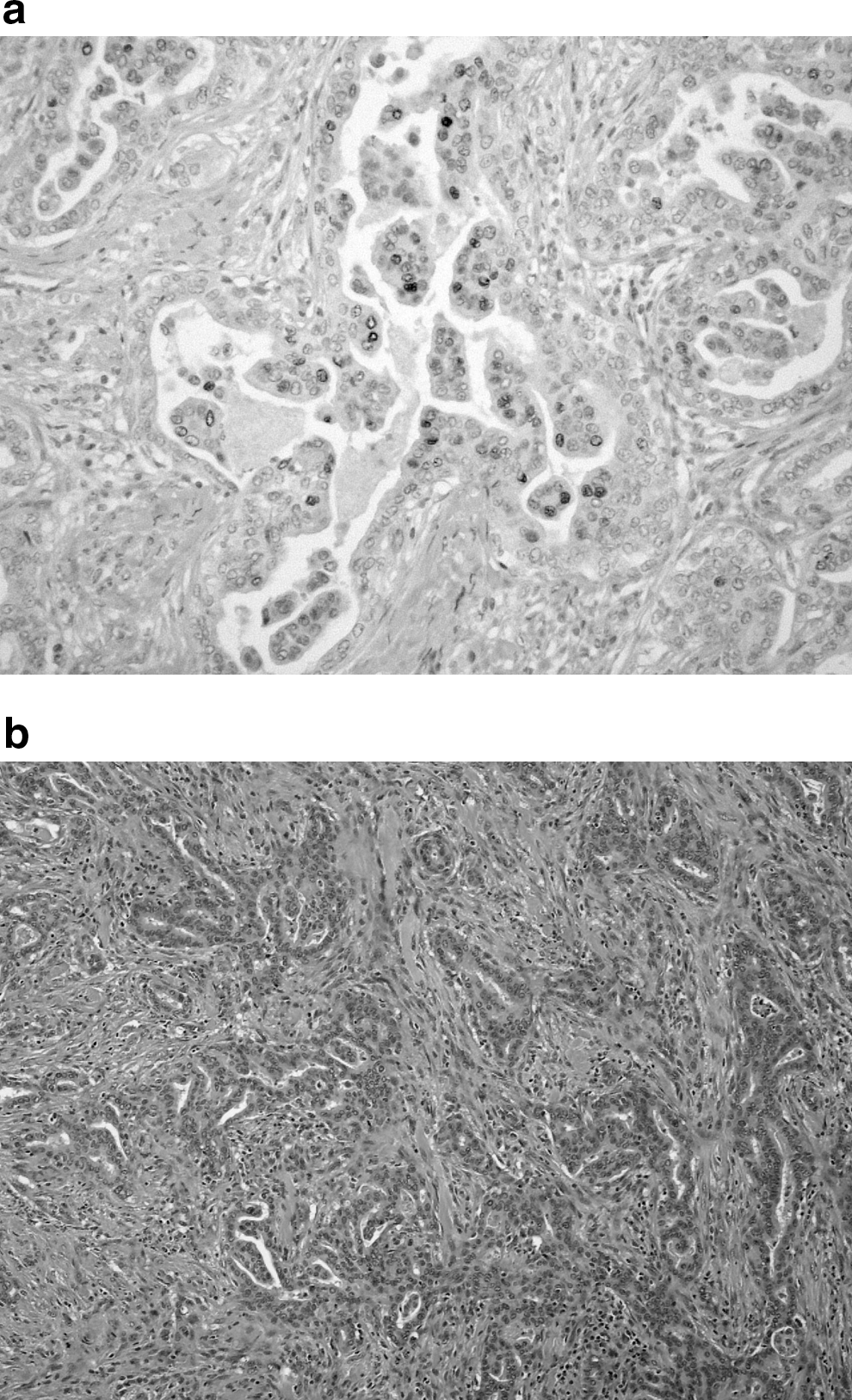
Surgical pathology revealed the recurrent tumor to be a poorly differentiated adenocarcinoma. Therefore, tumor samples were tested for positivity not only to the usual immunohistochemical markers for thyroid tissue, but also to a complete metastatic panel of immunohistochemical markers, including those more typical of breast and lung cancers. The recurrent tumor stained positively for CK7 and carbohydrate antigens 125 and 19.9, with additional weak reactivity for estrogen receptor-alpha (ER-α) (Fig. 2a, b) and focal positivity for gross cystic disease fluid protein 15 (GCDFP-15). The tumor was negative for TTF-1, thyroglobulin, CK20, progesterone receptor, and Her2Neu. Expression of ER-β was not evaluated. Ki67 staining ranged from 20% to 60% in moderately and poorly differentiated areas of tumor, respectively. Overall, this pattern of marker expression prompted concern for an extra-thyroid primary lesion, particularly a primary breast carcinoma. However, physical examination, mammogram, and ultrasonography of both breasts were negative for any suspicious findings. Comparison of immunohistochemistry studies of the initial malignancy with those of the recurrent tumor revealed interim loss of TTF-1 positivity, enhancement of ER-α positivity (<5% staining in the initial tumor versus 30% staining in the recurrent tumor), and gain of focal weak GCDFP-15 positivity, which was not present in the initial tumor. Of note, the patient had no history of estrogen-based hormone replacement therapy, either before presentation with her primary tumor or in the interim between her initial thyroidectomy and tumor recurrence.
To date, no further studies to evaluate for an occult breast carcinoma have been performed. Metastatic work-up has not revealed any evidence of distant spread of the patient's thyroid malignancy. The patient is undergoing external-beam radiation treatments, with the possibility of addition of radioiodine treatments and adjuvant chemotherapy with tyrosine kinase inhibitors at a later date.
Discussion
This case represents an aggressive form of PTC with an atypical immunohistochemical expression profile. Despite the patient's previous diagnosis of PTC, the recurrent tumor expressed neither TTF-1 nor thyroglobulin, both of which are considered important markers of thyroid tissue. However, this patient had a high titer of anti-thyroglobulin antibodies, which might explain the lack of immunoreactivity of her tumor to thyroglobulin. In addition, loss of TTF-1 expression has been reported in undifferentiated thyroid neoplasms as the result of an epigenetic silencing event (4).
The presence of both ER-α and GCDFP-15 staining in the recurrent tumor initially raised a high level of suspicion for a primary breast adenocarcinoma. Although metastases to the thyroid gland are rare, breast cancers are among the most commonly encountered primary malignancies that seed there (2). GCDFP-15 has been reported to have a sensitivity of 54% and a specificity of 96% for tumors of mammary origin (5). ER-α positivity is likewise most commonly associated with cancers of the breast or ovaries. There have certainly been at least six case reports of primary breast carcinoma with histopathologic features reminiscent of the tall cell variant of PTC (6). Nevertheless, mammography and ultrasonography of the breasts effectively ruled out the possibility of a de novo breast primary in this patient. Therefore, this is to our knowledge the first reported case of GCDFP-15-positive thyroid cancer.
It has previously been reported that the human thyroid gland expresses a low level of ERs (7 –9). ER expression seems to increase with proliferation of thyroid glandular tissue, both in cases of benign hyperplasia and in certain instances of thyroid malignancies (7,8). The ER isoform most abundantly expressed in these instances is ER-α, which seems to mediate the growth-stimulating effects of estrogen on various tissues (7,10,11). ER-β, the other receptor isoform, seems to be expressed at a basal level in both normal thyroid tissues and in a variety of thyroid lesions (7,8). ER-β appears to have pro-apoptotic actions, and so opposes the actions of ER-α (10,11). It has been widely hypothesized that an imbalance in expression of these two isoforms, such that ER-α becomes more abundant than ER-β, might play a role in proliferation of thyroid lesions in the setting of estrogen exposure. This molecular interplay has been put forth as a key factor in the prevalence of thyroid carcinoma in young woman patients (8,11 –13). Indeed, studies have demonstrated that estrogen or its agonists stimulate the proliferation of PTC cells in vitro in an ER-α-dependent manner (11 –13). A recent publication also reported ER-dependent estrogen-mediated stimulation of adhesion, migration, and invasion of both PTC and normal transformed thyroid cell lines in vitro (14). However, the relevance of these findings in clinical practice has been largely unaddressed. One exception is a small retrospective study of the characteristics of thyroid cancers in pregnant or postpartum versus nonpregnant women (15). This study found that a significantly higher percentage of thyroid cancers diagnosed during or shortly after pregnancy expressed ERs. Further, patients in these groups also had significantly higher persistence/recurrence, as well as a trend toward more extensive spread of cancer to local nodes, than patients whose cancer had no temporal relationship to pregnancy (15). These results provide clinical evidence in support of a role for estrogen in the development of more aggressive thyroid cancer, although the study's sample size was small and its findings were merely correlative.
Estrogen and estrogen-like compounds have also been shown to have effects on thyroid cancer cells in the absence of ERs. Early reports such as the one by Hoelting and colleagues suggested that the selective ER modulator tamoxifen inhibits growth and invasion of follicular and papillary thyroid cancer cell lines in vitro (16). This study also demonstrates decreased growth of follicular cancer xenografts in mice treated with tamoxifen versus placebo (16). Interestingly, none of the cell lines used in these experiments expressed ERs. A more recent publication by Vivacqua and colleagues reported that tamoxifen, as well as estradiol and the phytoestrogen genistein, stimulates in vitro proliferation of certain follicular and anaplastic thyroid cancer cell lines (17). In this study, both the estrogens and tamoxifen were demonstrated to activate the growth-promoting MAP kinase signaling pathway through the G-protein-coupled receptor GPR30 (17). In this manner, despite expression of ER-α in two of the three cell lines tested, the compounds promoted growth in all three cell lines by an ER-independent mechanism. Of note, no papillary thyroid cancer cell lines were examined by this research group.
The profile of certain coregulatory proteins expressed by thyroid cancer cells may be an additional important marker of clinical outcome along with ER status and the estrogenic environment of the tumor. In a study recently published by Kavanagh and colleagues, estradiol treatment of an ER-expressing follicular thyroid cancer cell line increased expression of steroid receptor coactivator-1 (SRC-1) and overall proliferation of the cells (18). However, SRC-1 siRNA knockdown decreased basal proliferation, but not estradiol-induced proliferation, in the same cells (18). The authors suggested that this result highlights the possibility of functional redundancy of steroid receptor cofactors in thyroid malignancy, similar to that postulated for breast cancer. The data also suggest that these coregulatory proteins may have growth-promoting roles both in conjunction with and autonomously from their established molecular pathways. In particular, SRC-1 was found to be highly expressed in anaplastic and poorly differentiated tumor specimens—an inverse expression pattern to that of ER-α—and was shown to be associated with capsular invasion and reduced disease-free survival (18). Conversely, ER-α expression was positively correlated with the expression of the nuclear corepressor NCoR, and presence of both proteins was correlated with well-differentiated tumors and good overall prognosis (18).
While it seems clear that estradiol can have growth-promoting effects on thyroid carcinomas, the role of ERs in mediating these effects remains less certain, given the host of growth-promoting signaling pathways shown to be activated by estradiol and demonstrated expression of ER coregulatory proteins in cells lacking ERs (18). With respect to the role of ERs in promoting metastatic potential of thyroid malignancies, more data are needed. Even in light of these past studies, our finding of ER expression by a PTC in a postmenopausal woman remains highly unusual. Even more dramatic is the increase in ER expression level from <5% in the original cancer to 30% in the recurrent lesion. Given the low serum levels of endogenous estrogens expected in such a patient, and in the absence of estrogen-replacement therapy, it seems unlikely that estrogen stimulation of the tumor explains its rapid growth. So what role, if any, does ER-α play in promoting the aggressive phenotype of this patient's tumor? On the basis of the literature, it seems plausible that an imbalance between ER-α and ER-β could be a factor. It is also possible that coregulatory proteins such as SRC-1 may have autonomously driven the proliferation of her malignant cells. Neither ER-β nor SRC-1 status was tested in this patient's tumor specimen. Further studies are necessary to establish the molecular pathways at work in thyroid carcinomas, particularly with respect to the de-differentiation of certain tumors. These data will in turn guide future selection of tumor markers that can be useful in predicting outcomes for patients found to have thyroid malignancy.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.