
Abstract
Background:
Tumor thrombus in the thyroid vein or the internal jugular vein may be caused by thyroid malignancies. Therefore, a tumor thrombus is very suspicious for malignancy. Total thyroidectomy should be performed in such patients if there is a primary thyroid tumor, and a high probability of pulmonary metastasis seems likely as there is direct exposure of malignant cells to the circulation. Our study was performed to determine whether ultrasonography is an effective preoperative modality to detect tumor thrombi of thyroid malignancies and whether tumor thrombi are associated with pulmonary metastases.
Methods:
Between 2004 and 2009, all thyroid surgery patients at Kuma Hospital had preoperative neck ultrasonography to look for tumor thrombi in the thyroid veins and the internal jugular veins as well as thyroid masses and abnormal lymph nodes. We looked for solid masses with an echogenic “tongue” in the internal jugular vein and masses with a projection from thyroid tumor to the thyroid vein on grayscale ultrasonography. We also used Doppler ultrasonography to look for the absence of blood flow.
Results:
Among 7754 patients who had thyroid surgery, there were 9 patients with tumor thrombi. In seven of the patients, tumor thrombi were detected by preoperative ultrasound, and in the remaining two patients, tumor thrombi were detected during surgery. Tumor thrombi were identified in the internal jugular vein in six patients and in the thyroid vein in three patients. Pulmonary metastases were present in three patients (50% of the patients with thyroid carcinoma). The patients with tumor thrombi were more likely (33.3%) to have pulmonary metastasis than those without (0.9%) tumor thrombi (p < 0.0001). In four patients with papillary carcinoma, projection-like lesions of irregularly shaped tumors were misdiagnosed to be tumor thrombi in the thyroid veins on preoperative ultrasound. These four patients did not have pulmonary metastases.
Conclusions:
The preoperative detection of a tumor thrombus on ultrasonography has important clinical significance. Therefore, preoperative neck ultrasound in patients with thyroid masses should attempt to determine whether there are signs of tumor thrombi as well as to characterize the nature and location of abnormal thyroid and extrathyroid masses.
Introduction
Here, we report that preoperative ultrasonography is an excellent modality to detect tumor thrombi of thyroid malignancies; this has implications in the clinical management of these patients.
Materials and Methods
Patients
We retrospectively reviewed the medical database of patients with thyroid tumors who underwent surgery between January 2004 and December 2009 in Kuma Hospital, including the demographic characteristics of patients with tumor thrombi. Preoperative ultrasonography was performed in all the patients who had thyroid surgery during this period. The ultrasound readings used in this study were made part of the routine care of these patients. Surgical samples of the thyroid, tumor thrombi, and lymph nodes were cut before fixation. Chest X-rays were performed in all the surgical patients, and chest computed tomography (CT) scans also were performed in the patients with malignancies before surgery. Pulmonary metastases were detected before surgery by chest X-rays and CT scans. Specimens were fixed in buffered formalin and embedded in paraffin, and hematoxylin and eosin and immunohistochemical stainings were performed. All related pathological specimens were reviewed (by M.H.), and the histopathological diagnosis was included in this study. The preoperative ultrasound readings were verified by surgeons during surgery and by histopathological examination postoperatively (1). The surgical findings and histopathological diagnosis were recorded in the medical database of the hospital.
Ultrasonography
Ultrasound examination was performed by well-trained, registered ultrasonographers, using a TOSHIBA Aplio SSA-770A ultrasound system with PLT-1204AX (7–14 MHz) and PLT-805AT (5–12 MHz) linear probes. In performing ultrasonography, we make it a rule to follow a standard scanning protocol to prevent missing clinically important lesions. After closely assessing normal anatomical structure in the neck and tumors in the thyroid gland, we tried to identify the presence of tumor thrombi and metastatic lymph nodes.
Ultrasonic diagnosis of tumor thrombus
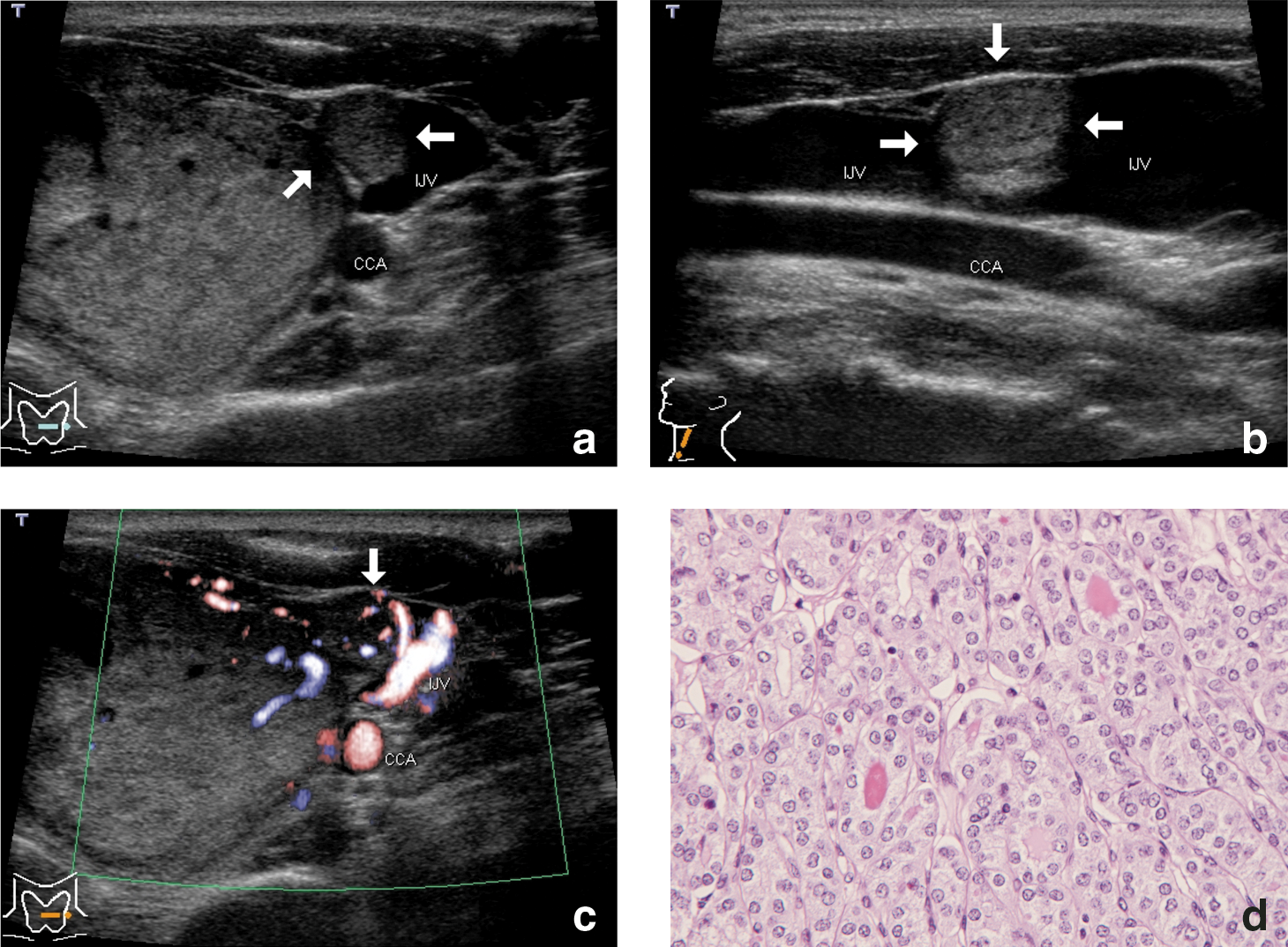
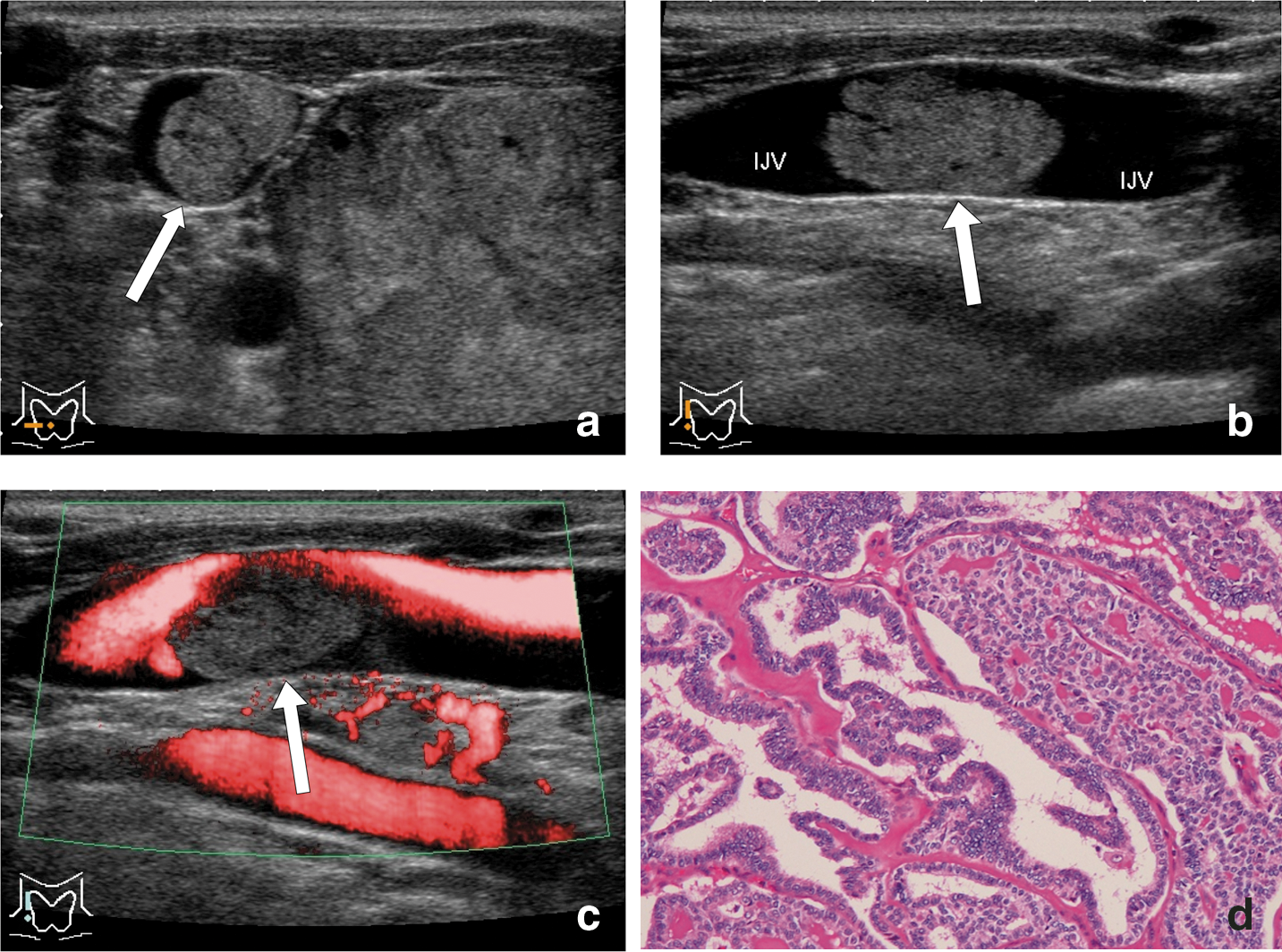
Anatomically, the thyroid gland has superior, middle, and inferior thyroid veins, and these veins flow into the internal jugular vein or the brachiocephalic vein (1). When a tumor thrombus extends and exists in the lumen of the internal jugular vein, grayscale ultrasonography shows a solid mass, that is, an echogenic “tongue.” An echogenic “tongue” extending from the thyroid tumor into the lumen of the internal jugular vein can be observed in the transverse and longitudinal (saggital) planes. Color or power Doppler ultrasonography shows turbulent Doppler signals of moving blood flow in the residual lumen of the internal jugular vein (2). When a tumor thrombus does not reach the internal jugular vein, a projection directly from thyroid tumor can be observed in the thyroid vein on grayscale ultrasonography. The lumen of the thyroid vein is completely occupied with a tumor thrombus; therefore, there is a projection of a solid mass adjacent to the thyroid tumor on grayscale ultrasonography. Doppler ultrasonography will not show a signal of blood flow in the region of the thrombus portion or the distal portion of the thyroid vein.
Statistical analysis
Statistical analysis was performed using chi-square test with InStat version 3.0. Statistical significance was set to a probability (p) value of <0.05.
Results
Patients
A total of 7754 patients undergoing thyroid surgery were included in this study. There were 2247 patients with benign thyroid tumors and 5507 patients with a thyroid malignancy or metastasis to the thyroid. Of these patients with malignancy, 5207 had papillary thyroid carcinoma, 183 had follicular thyroid carcinoma, 117 had poorly differentiated carcinoma, and 10 had metastatic carcinoma to the thyroid.
Of the 5507 patients with thyroid malignancy, there were 9 patients with tumor thrombi. In seven of these patients, tumor thrombi were detected by ultrasound before thyroid surgery, and in two patients, they were not reported on preoperative ultrasound but were detected during surgery and on postoperative histopathological examination. There were four patients in whom tumor thrombi were reported on preoperative ultrasound but were not reported intraoperatively and on postoperative histopathological examination. In these four patients with papillary carcinoma, projection-like lesions of irregularly shaped tumors were misdiagnosed to be tumor thrombi in the thyroid veins on preoperative ultrasound. These four patients did not have pulmonary metastases.
Patients with tumor thrombi
Table 1 shows the nine patients with tumor thrombi and thyroid malignancies. Tumor thrombi in seven patients (Patients 1–7) had been detected by ultrasonography preoperatively. Tumor thrombi in two patients (Patients 8 and 9) had not been detected by ultrasonography preoperatively but were detected intraoperatively. Histopathological examination showed follicular thyroid carcinoma in two patients (Patients 1 and 2), papillary thyroid carcinoma in three patients (Patients 3, 4, and 8), poorly differentiated carcinoma in one patient (Patient 5), metastastic carcinoma to the thyroid from renal cell carcinoma in two patients (Patients 6 and 7), and metastastic carcinoma from hepatic cell carcinoma in one patient (Patient 9). The side of tumor embolism was on the left side in three patients (Patients 1, 2, and 5) and on the right side in six (Patients 3, 4, and 6–9). Tumor thrombi were noted within the internal jugular vein in six patients (Patients 2–7) and within the thyroid vein in three (Patients 1, 8, and 9). Pulmonary metastases were diagnosed in three patients (Patients 1, 5, and 8). Pulmonary metastases were detected before surgery by chest X-ray and CT scans in two patients (Patients 5 and 8); this was detected by chest CT scan at 3 years and 10 months after surgery in one patient (Patient 1).
FC, widely: follicular thyroid carcinoma, widely invasive type; PC: papillary thyroid carcinoma; Poorly C: poorly differentiated carcinoma of the thyroid; m/RCC: metastatic carcinoma to the thyroid gland from renal cell carcinoma; m/HCC: metastatic carcinoma to the thyroid gland from hepatic cell carcinoma; mid.TV: middle thyroid vein; inf.TV: inferior thyroid vein; IJV: internal jugular vein.
Forty-nine patients (0.9%) had pulmonary metastasis among the 5498 patients without tumor thrombi. In contrast, 3 of 9 patients (33.3%) with tumor thrombus had pulmonary metastasis (p < 0.0001). As pulmonary metastases were noted exclusively in patients with thyroid carcinoma, 50% of the patients with thyroid carcinoma and tumor thrombi had pulmonary metastases.
Figure 1 presents an ultrasonographic image of a tumor thrombus of follicular carcinoma of the thyroid, widely invasive type, and the histopathological appearance in Patient 2. Direct tumor extension via the middle thyroid vein into the left internal jugular vein can be seen. Figure 2 presents an ultrasonographic image of a tumor thrombus of papillary thyroid carcinoma and the histopathological appearance in Patient 3. The tumor thrombus can be clearly observed as a protrusion into the internal jugular vein on ultrasonography.
Discussion
In patients with thyroid masses, it is important to determine whether preoperative ultrasound shows evidence of tumor thrombi. In Patients 1 and 2, the preoperative cytology was not positive for malignancy. Therefore, the presence of a tumor thrombus in the thyroid vein or internal jugular vein is strongly suspicious for malignancy even in the absence of malignant findings on cytology. Therefore, we recommend that total thyroidectomy be performed in such patients if they have a primary thyroid tumor. Our results also indicate that there is a strong possibility of pulmonary metastasis in patients with thyroid tumors and tumor thrombi. This is probably because there is direct exposure of malignant cells to circulatory blood flow.
Vascular invasion in histopathological sections is a well-documented microscopic characteristic of follicular thyroid carcinoma and a much more reliable sign of malignancy than capsular invasion. In general, the invaded vessels are located within the capsule or immediately outside it, and malignant cells of follicular carcinoma project into the vessel lumen in a thrombus-like fashion. A tumor thrombus or direct extension into the thyroid vein or the internal jugular vein is presumed to be a macroscopic form of the vascular invasion of follicular carcinoma.
Some previous reports documented the extension of follicular carcinoma into the internal jugular veins and superior vena cava (2 –5). Bussani and Silvestri (6) reported a rare case of neoplastic thrombotic endocarditis of the tricuspid valve in a patient with poorly differentiated follicular carcinoma of the thyroid. Extensive vascular invasion should be considered a risk factor for distant metastases or relapse (7,8). Tumor thrombus may increase the risk of distant metastatic disease, which can alter the clinical course of the patient. Although the prevalence of tumor thrombi in patients with papillary carcinoma is low in comparison with follicular carcinoma, the clinical importance of a tumor thrombus is the same in patients with follicular carcinoma.
Thyroid malignancies with tumor thrombi presence detected by ultrasonography have been reported in literature (9 –14). The invaded veins were the great veins of the neck in these reports. It is not difficult to detect a tumor thrombus in the internal jugular vein by ultrasonography. It is, however, very difficult to detect a tumor thrombus when it is located in the thyroid vein but does not reach the internal jugular vein. Two patients (Patients 8 and 9) had not been identified as having a tumor thrombus preoperatively by ultrasonography. Patient 8 had papillary carcinoma with a tumor thrombus in the middle thyroid vein; we preoperatively misdiagnosed the tumor thrombus as a metastatic lymph node in the neck. Patient 9 had metastatic carcinoma to the thyroid gland from hepatic cell carcinoma, with a tumor thrombus in the inferior thyroid veins; we could not detect the tumor thrombus by ultrasonography because of the complete obstruction of the fine veins under the clavicle.
In summary, the preoperative detection of a tumor thrombus on ultrasonography has a clinically important significance. On preoperative ultrasound examination, efforts should be made not only to localize and characterize thyroid masses, but also to determine whether tumor thrombi are present.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.