
Abstract
Background:
Although it is known that Hashimoto's thyroiditis in children and adolescents can go into long-term remission, and that treatment with thyroxine (T4) may not be necessary, it is difficult to quantify changes in the degree of autoimmune destruction of the thyroid. Here we report a patient in whom there was a relationship between functional and anatomical changes as assessed by hormone measurements and ultrasonography.
Summary:
The patient was a 12-year-old girl with Hashimoto's thyroiditis who was initially euthyroid and later treated with 50 μg levo-T4 when her free T4 (fT4) had declined from 17 to 7 pmol/L (normal range, 8–22 pmol/L). At this time her thyroid-stimulating hormone (TSH) was 4.1 mIU/L (normal range, 0.30–4.0 mIU/L) and thyroid ultrasonography demonstrated features of early inflammation. Two years later, while on the same dose of T4, ultrasound examination revealed severe end-stage Hashimoto's thyroiditis and thyroid function tests showed a T4 of 14.0 pmol/L and TSH of 0.81 mIU/L. Twelve months later, however, the thyroid ultrasound had returned to almost normal with only minimal features of inflammation. Thyroid function tests showed a fT4 of 12.8 pmol/L and TSH of 0.75 mIU/L. Her T4 treatment was then stopped. Eight, 17, and 30 weeks after this, her fT4 was 16.8, 9.7, and 13.9 pmol/L, respectively, and her respective TSH values at the same times were 0.10, 2.24, and 0.75 mIU/L.
Conclusions:
This is the first recording of serial thyroid ultrasound changes in a patient with Hashimoto's thyroiditis that paralleled changes in thyroid function. This indicates that thyroiditis can go into remission in some children. Thyroid ultrasound may be useful to make presumptive therapeutic decisions in children and adolescents with Hashimoto's thyroiditis whose dose of thyroid hormone seems to be less than is full replacement. Thyroid function tests, however, should ultimately guide T4 dosage.
Introduction
Patient Report
The patient was a 12-year-old girl when first seen in 2006 with a presumptive diagnosis of Hashimoto's thyroiditis based on high serum titers of thyroid antibodies and goiter. She felt well and the examination was normal apart from an enlarged, firm, nodular, and slightly tender thyroid gland. She was prepubertal. Serum fT4 was 17 pmol/L (normal range, 9–19 pmol/L) and TSH was 1.31 mIU/L (normal range, 0.4–4.0 mIU/L), but 6 months later she was biochemically hypothyroid with a low fT4 (7 pmol/L) and borderline increased TSH of 4.10 mIU/L and (Table 1). For the first time, she suffered from mild fatigue and weight gain. Treatment with 50 μg of levo-T4 (L-T4) was commenced. Over the next 3 years she remained well on this dose of T4 and went through normal puberty, gaining about 15 kg. Despite these changes the dose of L-T4 needed to maintain her in a euthyroid state remained unchanged at 50 μg.
Abs indicates antibodies; TPO, thyroid peroxidase A (reference range, 0–35 IU/mL); Tg, thyroglobulin (reference range, 0–40 IU/mL).
fT4 indicates free thyroxine (normal range, 9–19 pmol/L).
TSH indicates thyroid-stimulating hormone (thyrotropin) (normal range, 0.4–4.0 mIU/L).
NT, not tested; L-T4, levothyroxine.
Real-time thyroid ultrasonography (Sonosite Titan portable, 4–7 MHz small parts probe, black and white images, and color Doppler) was carried out at the first visit and on another two occasions over the next 3 years. Representative images of the left lobe are shown in Figure 1. Initially (Fig. 1A), the thyroid showed changes of early thyroiditis with a thin patchy texture, slight cystic changes, and reduced vascularity, and the gland was mildly enlarged. There were a few small nodular areas consistent with inflammatory lesions but no clearly defined nodule that required further assessment with fine-needle aspiration biopsy. A second ultrasound was carried out 24 months later in February 2008 because of continuing tenderness and some new nodularity. At this time the thyroid gland demonstrated a diffusely empty, cystic appearance with marked hypoechoicity throughout (Fig. 1B). This was considered to be consistent with the end-stage autoimmune destruction as seen in adult patients with Hashimoto's thyroiditis. A year later, she was well and still taking 50 μg of L-T4. A third ultrasound was carried out, in part to determine why she needed such a small dose of T4 despite significant weight gain and puberty, and in part to re-assess the nodularity. To our surprise her thyroid gland had filled in, was no longer hypoechoic and cystic, and overall looked fairly normal (Fig. 1C). On the basis of the small dose of L-T4 needed and the ultrasound appearance, T4 therapy was ceased and follow-up arranged for 6 weeks later. At that time she felt well but serum TSH was 0.1 mIU/L and fT4 16.8 pmol/L. TSH receptor antibody test was performed at this time and was negative (<1.0 mIU/L). Subsequently, her TSH and fT4 levels have remained normal (Table 1) and she feels well, except for being a little tired late in the day.
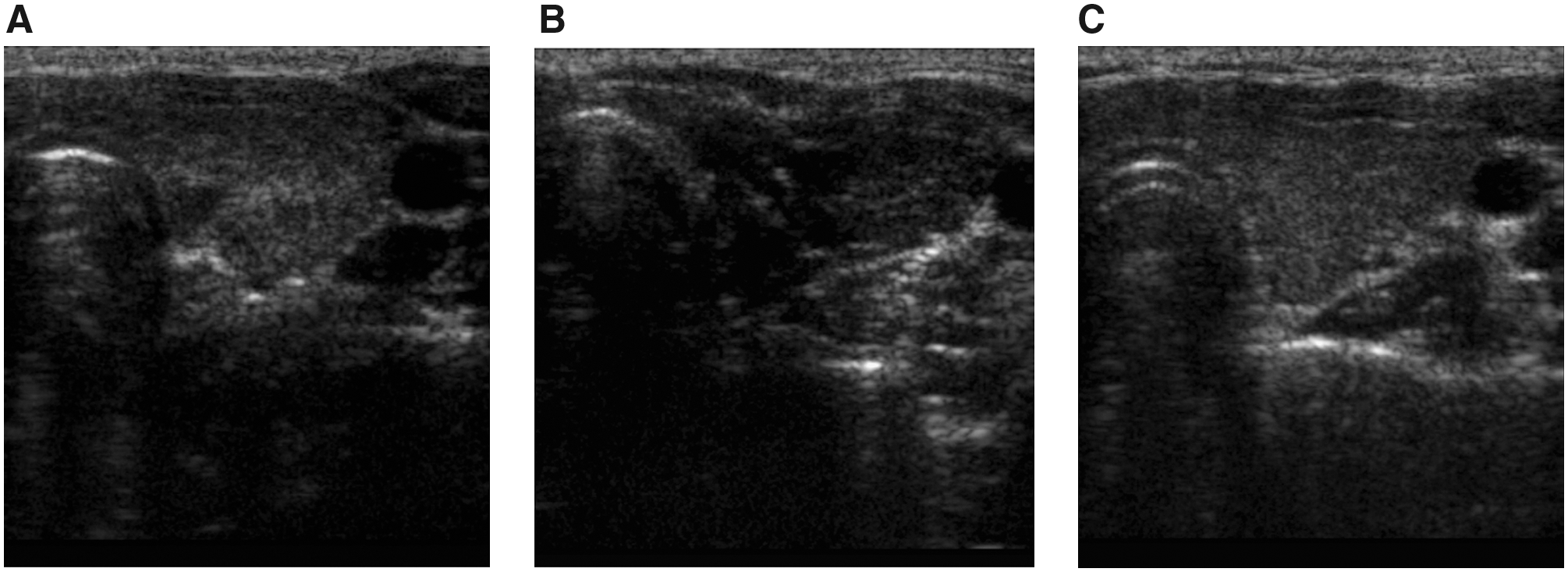
Thyroid ultrasonographic appearance in a 12-year-old girl with Hashimoto's thyroiditis and hypothyroidism.
Discussion
Although thyroid autoimmunity is generally considered to be progressive, it is becoming apparent that Hashimoto's thyroiditis is not always permanent in children in whom about a third will not need T4 therapy in the long term (1 –5). While other human organ-specific and multisystem autoimmune disorders, such as rheumatoid arthritis, type 1 diabetes, and multiple sclerosis, tend to be of a variable nature, relapsing, and remitting, but progressive in the long term, Hashimoto's thyroiditis, the most common of all human autoimmune disorders, appears to be different. For example, it is well known that Hashimoto's thyroiditis can convert to Graves' hyperthyroidism associated with the new production of TSH receptor antibodies (7). Soon after stopping T4 our patient had a serum TSH of 0.1 mIU/L. Although this might have reflected conversion to Graves' hyperthyroidism, it is more likely that she was having an episode of painless thyroiditis.
There have not been any studies using ultrasonography as a quantifiable parameter of the autoimmune reactions in the thyroid. One recent study of a large number of children with Hashimoto's thyroiditis (8) found abnormal findings in 37% of children that took from 4 to 17 months to become abnormal, but there was no case of resolution of changes in previously demonstrated end-stage disease. In this study, while 50% of children with normal ultrasound appearance initially developed changes within 7 months, full development took up to 5 years.
Remission of the thyroiditis in our patient coincided with puberty. However, it is generally thought that the surge in cases of Hashimoto's thyroiditis at the time of puberty accounts for the female preponderance of the disease (9). It is also possible for the thyroiditis to improve and even go into long-term remission at the time of puberty, as demonstrated by this patient. The reasons for the apparently variable effect of puberty on thyroid autoimmunity are unclear but may reflect the complex hormonal changes (10 –12) and increased iodine needs at this time (13).
Another possibility to consider is that because the damaged thyroid gland has the ability to regenerate, perhaps due to the growth effects of TSH, the amount of thyroid antigen(s) seen by the infiltrating immunocompetent cells increases. This leads to suppression of the autoimmune reaction through low (antigen) dose immune tolerance. Eventually, this would result in repopulation of the thyroid gland and clinical remission. While the same mechanism may apply in adults with Hashimoto's thyroiditis, this may be missed because older patients are expected to have permanent disease and are thus treated for life.
In summary, we have documented for the first time serial changes in the ultrasonographic appearance of the thyroid gland in a patient with Hashimoto's thyroiditis. These showed progression of the disease to classical end-stage destruction followed by return to almost normal over a 3-year period. Our patient's course suggests that in children and adolescents with Hashimoto's thyroiditis who require a relatively low doses of T4, the need for thyroid hormone replacement therapy should be periodically re-evaluated. Perhaps thyroid ultrasound would be a useful ancillary guide in this process.
Footnotes
Acknowledgments
This research was supported by grants from Sydney West Area Health Service (Nepean Hospital) and the Nepean Medical Research Foundation.
Disclosure Statement
The authors declare that no competing financial interests exist.