
Abstract
Background:
Fine-needle aspiration diagnosis of follicular carcinoma presents a dilemma because malignancy is confirmed when vascular or capsular invasion is present. Completion thyroidectomy may be necessary when the diagnosis of follicular carcinoma is made following hemithyroidectomy. Ablation of the remaining lobe with radioactive iodine has been used as an alternative to completion thyroidectomy. Here we report an unusual apparent complication of this treatment.
Patient Findings:
A 51-year-old woman presented in September 24, 2009 with a stony, hard calcification of left thyroid gland. She complained of recent progressive hoarsening of her voice. Her medical history was positive for a subtotal thyroidectomy on September 6, 1993. Histologic analysis identified follicular carcinoma. Two months postoperatively, the remaining tissue was ablated with 131I (150 mCi) as an alternative to completion thyroidectomy. We performed computed tomography of the neck, which demonstrated 1.6 × 1.9 × 2.2 cm dense speculated calcification of the entire left residual thyroid gland. The calcification infiltrated the trachea wall. Completion thyroidectomy, including resection of the calcification, was performed. Histologic examination revealed dystrophic calcification.
Conclusion:
We report an unusual replacement of the thyroid remnant with calcification that developed over a period of 16 years following radioactive iodine lobe ablation as an alternative to completion thyroidectomy for thyroid follicular carcinoma. To our knowledge, this is the first such case in the English language literature.
Introduction
We report an unusual patient in whom there was diffuse calcification of the thyroid remnant following RAI lobe ablation, which was performed as an alternative to completion thyroidectomy for thyroid follicular carcinoma.
Patient
A 51-year-old woman presented in September 24, 2009 with stony, hard calcification of the left thyroid gland. She had been referred to our hospital for evaluation of a palpable right-sided neck mass on July 7, 1993. Ultrasonography (US) disclosed a 3.6 × 4.1 cm isoechoic nodule in the right thyroid gland. The remaining thyroid gland was normal. Because of the size of the nodule, she underwent subtotal thyroidectomy on September 6, 1993. Histologic examination identified follicular carcinoma. Two months postoperatively, the remaining tissue was ablated with 131I (150 mCi) as an alternative to completion thyroidectomy. Posttherapy whole-body iodine scanning revealed no distant metastasis. Therefore, she was maintained on thyrotropin suppression therapy and followed up annually with whole-body iodine scanning, which showed no local recurrence or metastasis.
Neck US was first performed on December 14, 2001, and it demonstrated coarse calcification without evidence of lymphadenopathy. US-guided fine-needle aspiration of the coarse calcification could not be performed because the calcification was too hard to easily penetrate with a needle. Hence, she was followed up annually with neck US, which showed persistent coarse calcification. It was difficult to evaluate the change of size because accurate size measurement was impossible because of acoustic shadowing.
She complained of recent progressive hoarsening of her voice on September 24, 2009. Subsequent computed tomography of the neck was performed and demonstrated a 1.6 × 1.9 × 2.2 cm dense speculated calcification of the left residual thyroid gland (Fig. 1). The calcification had infiltrated the trachea wall (Fig. 1). On laryngeal stroboscopic analysis, left vocal cord paralysis was observed.

Computed tomography of the neck shows a 1.6 × 1.9 × 2.2 cm dense speculated calcification of the left residual thyroid gland. The calcification infiltrates the trachea wall.
Completion thyroidectomy, including resection of calcification, was performed. At surgery the left recurrent laryngeal nerve was enveloped in calcification. Gross examination of the resected calcification revealed a stony, hard lesion 3.0 cm in greatest diameter that required decalcification before gross sectioning (Fig. 2). Histologic analysis of the specimen revealed dystrophic calcification (Fig. 3).
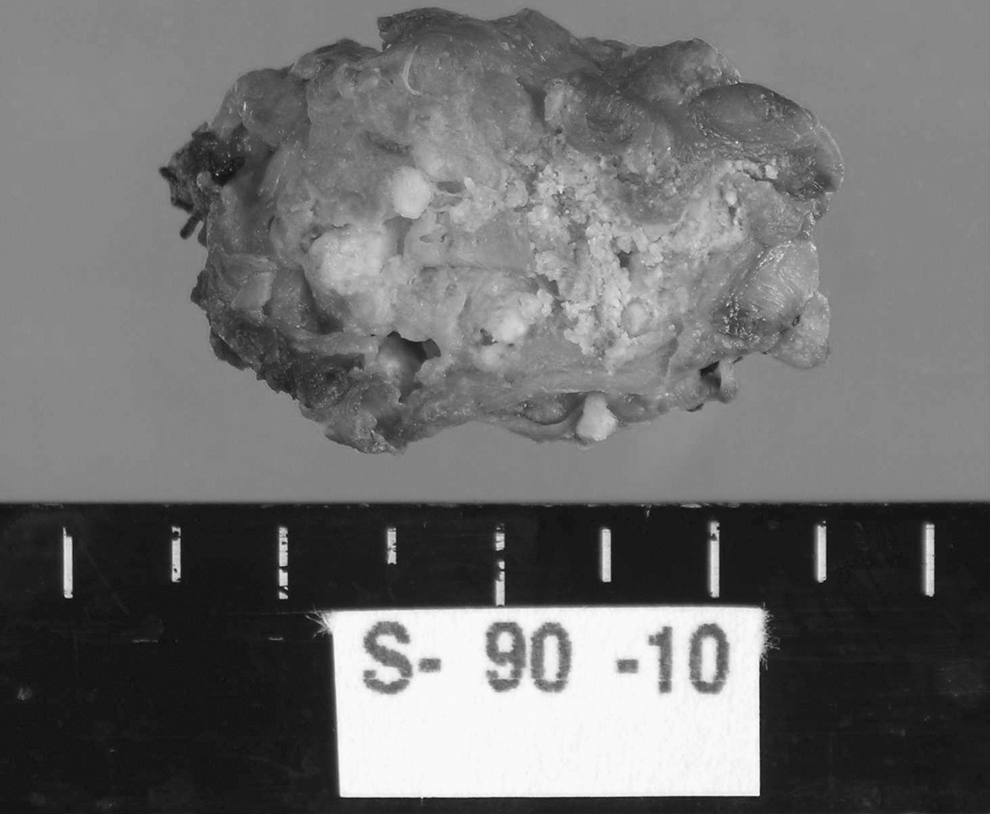
Surgical specimen showing a stony calcification of 3.0 cm in greatest diameter.
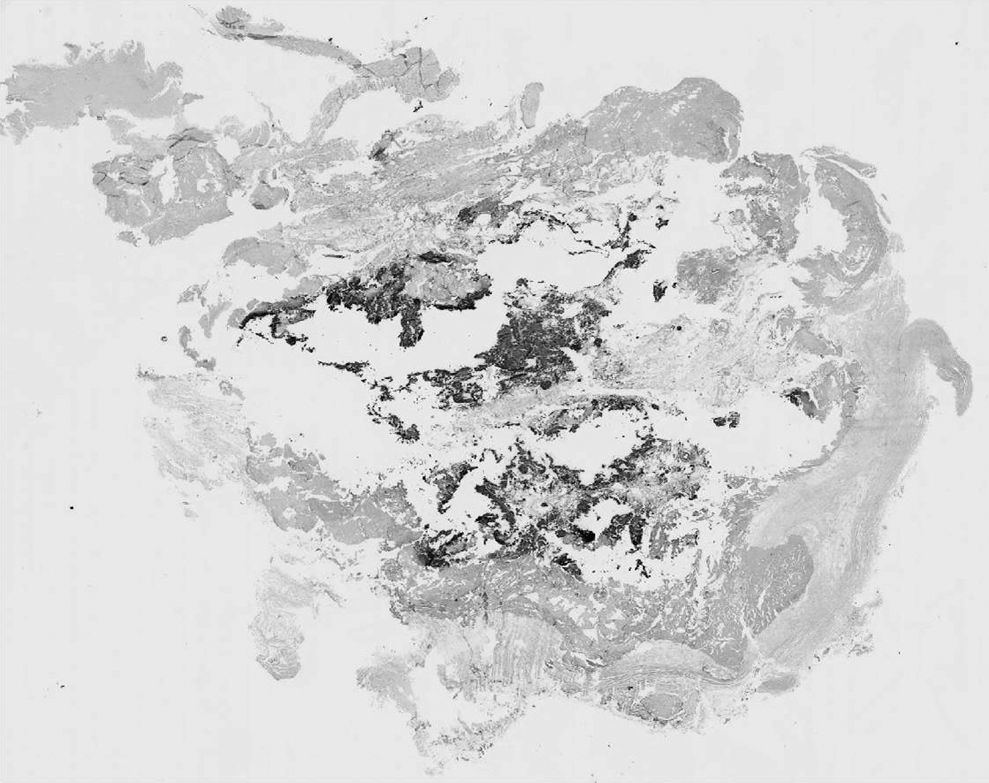
Histologic examination reveals dystrophic calcification (hematoxylin and eosin staining).
Discussion
This patient experienced unusual calcification of residual normal tissue over a period of 16 years after RAI ablation, which was performed as an alternative to completion thyroidectomy for thyroid follicular carcinoma. To our knowledge, this is the first such report in the English literature.
Calcification within the thyroid gland may occur in both benign and malignant thyroid diseases (3), and its pathogenesis remains nuclear. Some studies note that the prevalence of malignancy in a thyroid nodule containing calcification is greater than that in a noncalcified nodule (4,5). Intrathyroid calcification patterns include coarse, dense, nodular, piece-like, and rim-like calcifications, as well as microcalcification. Although microcalcifications are found in 61% of thyroid malignancies (6), intranodular coarse calcification may also be associated with malignancy (7).
On initial presentation, we suspected recurrent thyroid cancer in this patient because she had a history of follicular carcinoma and there was infiltration into the trachea wall and vocal cord paralysis. However, postoperative histologic analysis showed only dystrophic calcification without malignant cells. Advanced benign calcifications are extremely rare. Verburg et al. (8) reported a case of a benign goiter breaking through the trachea wall. There has been also a case report of a benign calcified thyroid cyst with skin sinus formation (9). In our patient, the shape of the calcification was interesting and has not been reported previously.
Dystrophic calcification is a calcification that occurs as a result of tissue necrosis or degeneration (10). Various forms of trauma have been implicated in its development. Damaged cell membranes leak calcium ions into cells, and these ions are subsequently concentrated by mitochondria, reaching levels that are high enough to form crystals (10). RAI ablation is a destructive force for normal residual thyroid tissue (11). Subcutaneous calcification as a manifestation of late effects of radiation treatment has been reported (12 –17). The process, which takes many years, is not clear.
The clinical effects of radiation depend on the dose, duration, and condition of the patient. Burmeister et al. (18) noted radiation thyroiditis in 60% of patients receiving lobe RAI ablation (50–150 mCi) and suggested a dose effect. Allweiss et al. (19) reported a greater risk of thyroiditis with larger thyroid remnants. Our patient underwent subtotal thyroidectomy and thus had a relatively large residual tissue, which received high-dose RAI therapy. We believe it is very likely that her dystrophic calcification resulted from prior RAI therapy.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.