
Abstract
Background:
We previously reported that multiple thyroid cysts may be a cause of hypothyroidism in patients with a relatively high iodine intake and we termed it polycystic thyroid disease (PCTD). The aim of this study was to investigate the prevalence of PCTD in patients who visited our thyroid center. We hypothesized that patients with PCTD are not rare in a region with a high iodine intake.
Methods:
We retrospectively studied the cause of hypothyroidism based on medical histories and ultrasonography in new patients to our hospital from April 2008 to March 2009 whose serum tests for antithyroglobulin antibodies (TgAb) and thyroid peroxidase antibodies (TPOAb) were negative. Serum thyroid hormones, thyrotropin (TSH), TgAb, and TPOAb were measured in 8243 patients. Patients with four or more thyroid cysts, negative tests for TgAb and TPOAb, no evidence for thyroid diseases other than their thyroid cysts, and no exposure to thyroid-perturbing influences were defined as having PCTD.
Results:
Three hundred seven patients had overt hypothyroidism (TSH level above 10.0 μU/mL and free thyroxine level below 0.7 ng/dL), of whom 71 patients were both TgAb and TPOAb negative. There were 546 patients with subclinical hypothyroidism (TSH level above 5.0 μU/mL and normal free thyroxine), of whom 193 patients were both TgAb and TPOAb negative. There were 24 patients with overt hypothyroidism and PCTD, accounting for 7.8% (24/307) of all causes of overt hypothyroidism. There were 42 patients with subclinical hypothyroidism and PCTD, accounting for 7.7% (42/543) of all causes of subclinical hypothyroidism. PCTD was more common among elderly people than young people.
Conclusions:
PCTD appears to be a minor but not negligible cause of hypothyroidism, at least in iodine-rich regions. PCTD with hypothyroidism may have been misdiagnosed as thyroid antibody–negative Hashimoto's thyroiditis in many reports.
Introduction
Subjects and Methods
There were 14,365 new patients who came to Kuma Hospital, which specializes in thyroid diseases, from April 2008 to March 2009. The chief complaints of many of these patients were suggestive of thyroid disease. Therefore, serum thyroid hormones, thyrotropin (TSH), and both antithyroglobulin antibodies (TgAb) and antithyroid peroxidase antibodies (TPOAb) were measured in 8243 patients. Among them there were 307 patients with overt hypothyroidism (TSH level above 10.0 μU/mL and free thyroxine [FT4] level below 0.7 ng/dL). There were 543 patients with subclinical hypothyroidism (TSH level above 5.0 μU/mL and FT4 level 0.7–1.6 ng/dL). Among the 8243 patients studied, 4058 had negative tests for both TgAb and TPOAb. Among these patients negative for TgAb and TPOAb, 71 had overt hypothyroidism and 193 had subclinical hypothyroidism (Fig. 1). All of these patients with overt and subclinical hypothyroidism had thyroid ultrasonography to clarify the cause of their hypothyroidism. In addition, we retrospectively studied their medical histories for information that might provide the cause of hypothyroidism, including exposure to drugs with antithyroid properties, thyroid surgery, and radiation. Further, iodine intake was routinely estimated by a questionnaire that assessed the kind and amounts of seaweed the patients were taking.
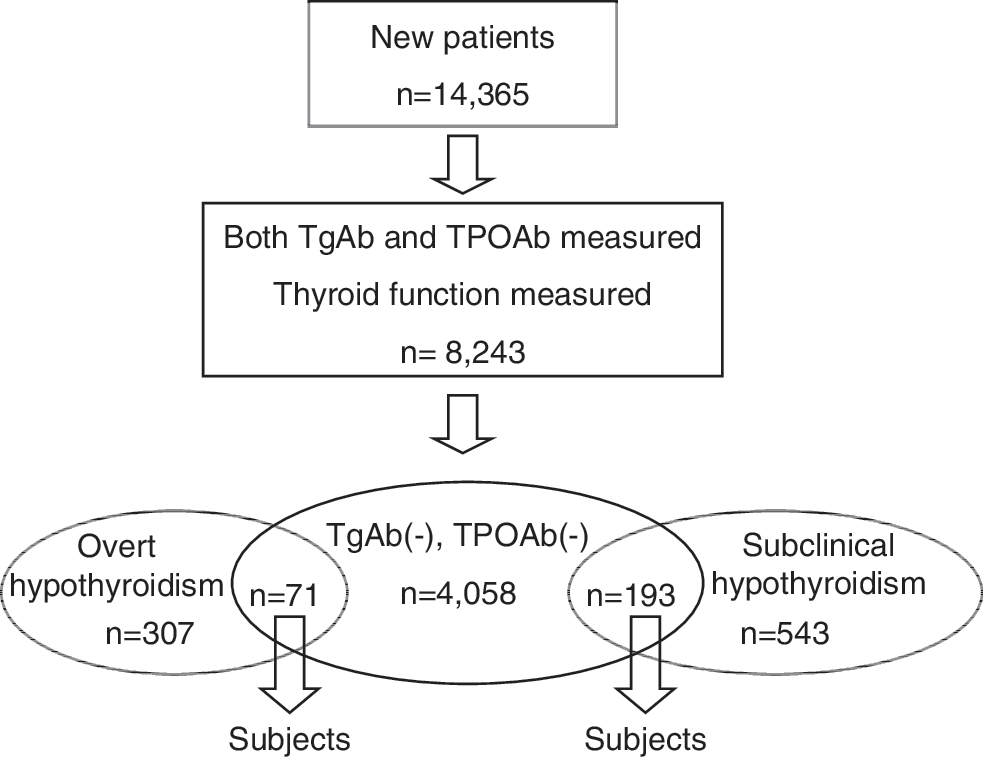
Selection of subjects. Overt hypothyroidism was defined by thyrotropin level above 10.0 μU/mL and free thyroxine level below 0.7 ng/dL. Subclinical hypothyroidism was defined by thyrotropin level above 5.0 μU/mL and free thyroxine level 0.7–1.6 ng/dL.
Patients with negative antithyroid antibodies having four or more thyroid cysts were defined as having PCTD unless they also had evidence for other thyroid diseases or exposure to antithyroid agents. Patients who were otherwise similar but who had several but not four or more thyroid cysts were categorized as having suspected PCTD. Three cases of PCTD from our previous report (1) are included in this study. Patients with negative antithyroid antibodies having a diffusely enlarged thyroid and inhomogeneous hypoechogenicity were classified as having Hashimoto's thyroiditis. Patients having two or more solid or mixed thyroid nodules were defined as having multinodular goiter.
Laboratory methods
TSH, FT4, and free triiodothyronine (FT3) concentrations were measured by employing chemiluminescent immunoassays (Architect TSH, Architect FT4, and Architect FT3, respectively; Abbott Japan Co.). Normal ranges are 0.3–5.0 mU/L for TSH, 0.7–1.6 ng/dL for FT4, and 1.70–3.70 pg/mL for FT3. Serum levels of TgAb and TPOAb were measured employing an electrochemiluminescence immunoassay (ECLusys 2010; Roche Diagnostics Corp.; normal range: <39.9 IU/mL for TgAb, <27.9 IU/mL for TPOAb).
Results
The causes of overt hypothyroidism in patients having negative tests for TgAb and TPOAb are summarized in Table 1. Twenty-four patients had PCTD and 4 patients had suspected PCTD. In the PCTD group with overt hypothyroidism, 13 patients were female and 11 were male. Their average age was significantly higher than that of all patients (71.54 ± 9.64 vs. 61.89 ± 16.55 years, respectively; p < 0.05, Mann–Whitney U test). The second largest group of patients presented in Table 1 was patients with Graves' disease who were taking antithyroid drugs or had received radioactive iodine ablative therapy. All patients with apparent drug over treatment for Graves' disease had been started on antithyroid drugs at their previous hospitals. Ten of 11 patients in this group had positive tests for TSH-binding inhibitor immunoglobulin when first seen at our hospital. The third largest group of patients with antithyroid antibody–negative overt hypothyroidism had Hashimoto's thyroiditis (see Subjects and Methods section for diagnostic criteria). The remaining patients had destructive thyroiditis, external radiation exposure to the neck, congenital thyroid abnormalities, and exposure to lithium carbonate. Patients with destructive thyroiditis had a history of transient thyrotoxicosis. We were unable to identify the causes of hypothyroidism in 16 patients, but many of these patients had slightly enlarged thyroids or slightly inhomogeneous hypoechogenicity in the thyroid. Therefore, a considerable number of patients in the group whose cause of hypothyroidism was not identified may have had very mild Hashimoto's disease. In 31 (43.7%) patients, the estimated daily iodine intake was >3 mg, which would be considered excess iodine intake. An excess iodine intake was mostly observed in the group with PCTD (17 of 24 patients) and the group without an identified cause of hypothyroidism (9 of 16 patients). Hypothyroidism was the severest in patients with Hashimoto's thyroiditis and the mildest in those with subacute thyroiditis.
Values are means ± SD. Normal range: FT4 0.70–1.60 ng/dL, FT3 1.70–3.70 pg/mL, TSH 0.30–5.00 μU/mL.
ATD, antithyroid drug; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyrotropin; SD, standard deviation; RAIT, radioactive iodine therapy.
Table 2 presents the causes of subclinical hypothyroidism in patients without positive TgAb and TPOAb. Forty-two patients had PCTD and 13 patients were suspected of having PCTD. In the PCTD group with subclinical hypothyroidism, 30 patients were female and 12 were male. Their average age was also significantly higher than that of all patients (66.60 ± 8.60 vs. 56.70 ± 16.84 years, respectively; p < 0.001, Mann–Whitney U test). The second largest group in Table 2 was patients with Graves' disease who were taking apparently excessive doses of antithyroid drugs or had been treated with radioactive iodine. The third largest group presented in Table 2 consisted of patients who were considered to have multinodular goiter. The remaining causes of subclinical hypothyroidism were Hashimoto's thyroiditis, destructive thyroiditis, external radiation exposure to the neck, and exposure to lithium carbonate. There was also one patient with a congenital thyroid abnormality. In almost half of the patients presented in Table 2, the causes of subclinical hypothyroidism were unidentified. Excess of iodine intake was observed in 43 (22.3%) patients. The prevalence of excess iodine intake in patients with subclinical hypothyroidism was lower than in patients with overt hypothyroidism.
Values are means ± SD. Normal range: FT4 0.70–1.60 ng/dL, FT3 1.70–3.70 pg/mL, TSH 0.30–5.00 μU/mL.
Discussion
Overt hypothyroidism was thought to be induced by PCTD and was present in 24 patients, which accounted for 7.8% (24/307) of all causes of hypothyroidism, including those with and without positive tests for antithyroid antibodies, in this study. Similarly, in 7.7% (42/543) of the patients with subclinical hypothyroidism, this was thought to be induced by PCTD. This means that hypothyroidism induced by PCTD is not rare, at least in Japan. PCTD has been probably misdiagnosed as Hashimoto's thyroiditis thus far (2), because the entity of PCTD as a cause of hypothyroidism was only reported recently (1). But that report did not establish the prevalence of PCTD in the general population or the percentage of patients with the ultrasound findings of PCTD and no other thyroid disorders or exposures to antithyroid agents but who had hypothyroidism.
The present study indicates that PCTD causes hypothyroidism in males as well as females. There were no male patients in our previous case report series (1), but, in the present study, 11 of 24 PCTD patients with overt hypothyroidism and 12 of 42 PCTD patients with subclinical hypothyroidism were male. In the previous case report series (1), we thought that the hypothyroidism induced by PCTD developed gradually over many years because the series contained no young patients. This concept was confirmed in the present study by the finding that the average age of patients with PCTD was the highest among all patients with hypothyroidism and negative tests for antithyroid antibodies.
In our previous case report series, we noted that patients with ultrasound findings of PCTD appear to be susceptible to the development of hypothyroidism when exposed to a high iodine intake, because some patients with PCTD became euthyroid when their iodine intake was decreased (1). In the present study, an excess dietary iodine intake was observed in two-thirds of the patients with PCTD, a finding also consistent with the concept that dietary iodine excess promotes the development of hypothyroidism in PCTD. We are now interested in whether PCTD is associated with hypothyroidism in iodine-deficient regions. There may be several reasons why PCTD as a cause of hypothyroidism has been only recently discovered. One is that hypothyroidism induced by PCTD is mild. Another is that in many patients the hypothyroidism may be transient as exposure to excess iodine is also transient. Finally, when assessed only by palpation, the goiter of PCTD may be difficult to distinguish from the goiter of Hashimoto's disease.
Presently, we do not know the mechanism of hypothyroidism induced by PCTD. We speculate that the volume of normal thyroid hormone–producing tissue is decreased because of multiple cysts in PCTD (1,3). We also need to determine if the cysts present in PCTD are different from simple cysts. In the literature from many areas of the world, multinodular goiter is not associated with hypothyroidism. Although PCTD may have been classified as multinodular goiter by ultrasonography, we assume that PCTD may be a different form of multinodular goiter. Unfortunately, we do not have any histopathological information in the present study.
In summary, we determined the cause of hypothyroidism in patients with overt and subclinical hypothyroidism whose tests for both TgAb and TPOAb were negative in a large series of patients who sought medical care at our hospital during a 1-year period. Of the 307 patients with overt hypothyroidism, 71 did not have positive tests for antithyroid antibodies, and in 24 patients (7.8%), PCTD was the cause of their thyroid dysfunction. PCTD was the cause of hypothyroidism in an almost identical percentage (7.7%) of patients with subclinical hypothyroidism. The cause of hypothyroidism in patients with PCTD has been probably misdiagnosed as thyroid antibody–negative Hashimoto's thyroiditis in many reports. PCTD appears to be a minor but not negligible cause of hypothyroidism, at least in iodine-rich regions.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.