
Abstract
Background:
The lingual thyroid is uncommon, and the need for resection of this condition is even more rare. Techniques for removal have historically included wide access with associated disfiguring incisions. We sought to describe a minimally invasive and safe technique for the management of the obstructive lingual thyroid gland that achieves optimal hemostasis with the use of technology.
Methods:
Institutional Review Board approval was obtained to evaluate the safety and efficacy of a minimally invasive technique to remove the obstructive lingual thyroid gland. The procedure is performed in ∼1 hour; requires no splitting of the lip, tongue, or mandible, is associated with negligible blood loss, and is accomplished on an outpatient basis.
Results:
The procedure was undertaken in a 34-year-old woman with a longstanding lingual thyroid that began to cause dysphagia. She was found to be clinically and biochemically euthyroid, and was referred for surgical intervention. The procedural time was 90 minutes, and the estimated blood loss was 15 mL. She was discharged shortly after recovery, on an outpatient basis.
Conclusions:
A number of surgical approaches to the obstructive lingual thyroid have been described, including the use of a lip-split, tongue-split, mandibulotomy, and cervical pharyngotomy approach. We describe a minimally invasive transoral procedure that incorporates Harmonic technology and high-resolution endoscopy and is accomplished with no external incisions on an outpatient basis.
Introduction
When a lingual thyroid becomes symptomatic, removal is advocated. Because this is uncommon, there are few reports in the literature describing proposed techniques, and most of these are invasive and associated with substantial morbidity [including splitting of the lip (5), splitting of the tongue (6), splitting of the mandible (7), and transcervical pharyngotomy approaches (8)].
Minimally invasive surgical techniques have been proposed for more than two decades, and now have been applied to virtually every surgical discipline. In the head and neck, minimally invasive cervical thyroid techniques have been increasingly embraced. Minimal access transoral resection of oropharyngeal and hypopharyngeal lesions was popularized by Steiner et al. (9) and has proven to be beneficial for many patients.
Simultaneous with the advent of minimal access techniques has been the introduction of certain technologies that may facilitate these approaches. Chief among these have been the refinement of high-resolution endoscopy, and the advent of robust hemostatic energy devices, including Ligasure and Harmonic technology.
We sought to combine the principles associated with minimally invasive surgery with application of technology to achieve a straightforward, minimally invasive lingual thyroidectomy technique with ample videoendoscopic documentation.
Materials and Methods
Institutional Review Board approval was obtained to perform an analysis of a new surgical technique for the management of the obstructive lingual thyroid gland. Relevant data were acquired in a prospective manner.
Comprehensive patient demographic data were obtained on a patient with a lingual thyroid gland (Fig. 1), including age, gender, thyroid function studies, and comorbidities. Careful preoperative documentation of the diagnosis of lingual thyroid gland included an 131I scan (Fig. 2) and a contrasted neck CT scan (Fig. 3). Additionally, a preoperative laryngoscopic examination of the lingual thyroid was recorded (see Supplementary Video, available online at
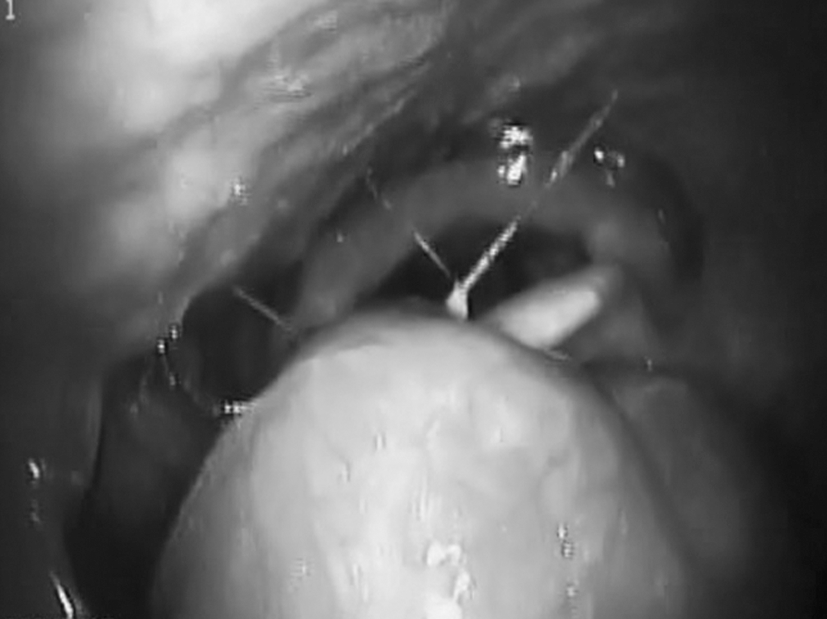
Preoperative flexible laryngoscopy revealing an obstructive lingual thyroid gland.
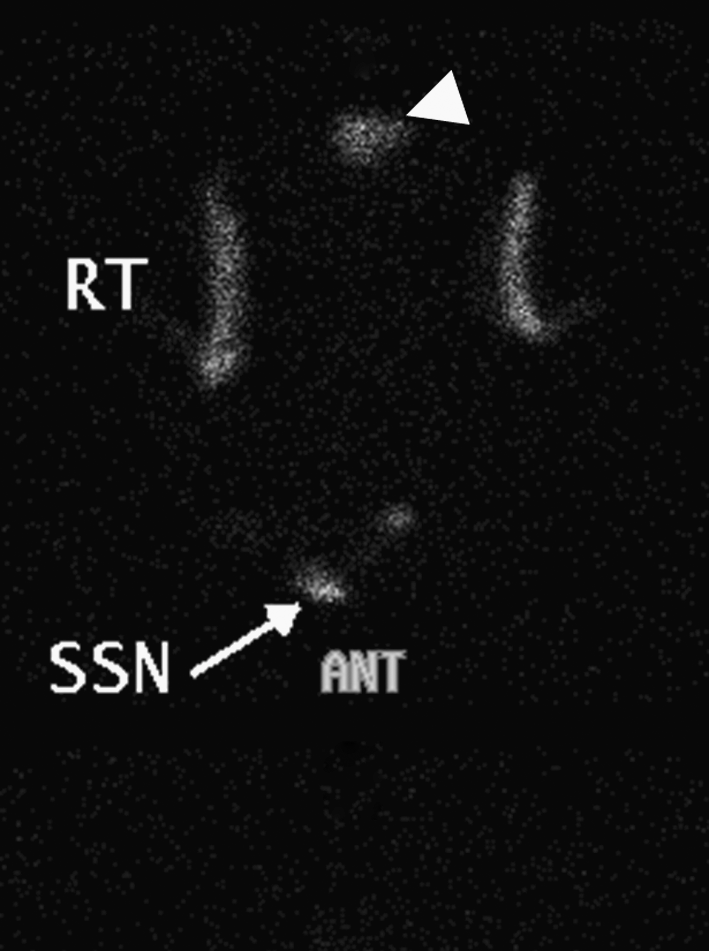
Iodine-123 scan demonstrating uptake of radioactive iodine in the tongue base (indicated by the white arrowhead). SSN, suprasternal notch; RT, right; ANT, anterior.
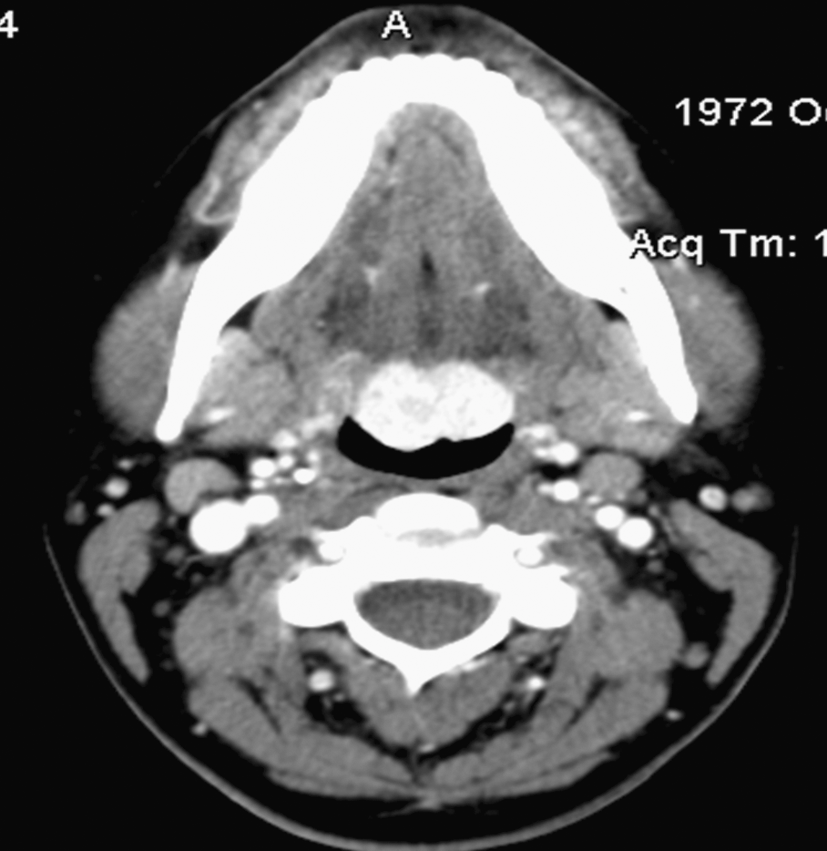
Contrast-enhanced axial CT scan demonstrating concentration of the contrast material in the lingual thyroid gland at the base of tongue.
While suppression of this gland had been attempted, because of a prior difficult intubation related to the lingual thyroid gland and new onset of dysphagia, surgical excision was requested.
Results
The safety and efficacy of the proposed technique were validated in a 34-year-old woman with a lingual thyroid gland. Her thyroid function tests were normal, and her only comorbidity was hypercholesterolemia. She was on a suppressive dose of 100 mcg of levothyroxine. After informed consent was obtained, an endoscopic surgical excision was undertaken (see Supplementary Video). The surgical time was 90 minutes, and the estimated blood loss was 15 mL.
Description of procedure
The patient was brought to the operating room and placed supine on the operating table. After satisfactory induction of anesthesia and sterile prepping and draping of the patient, intraoral access was established and maintained with a side-biting mouth gag.
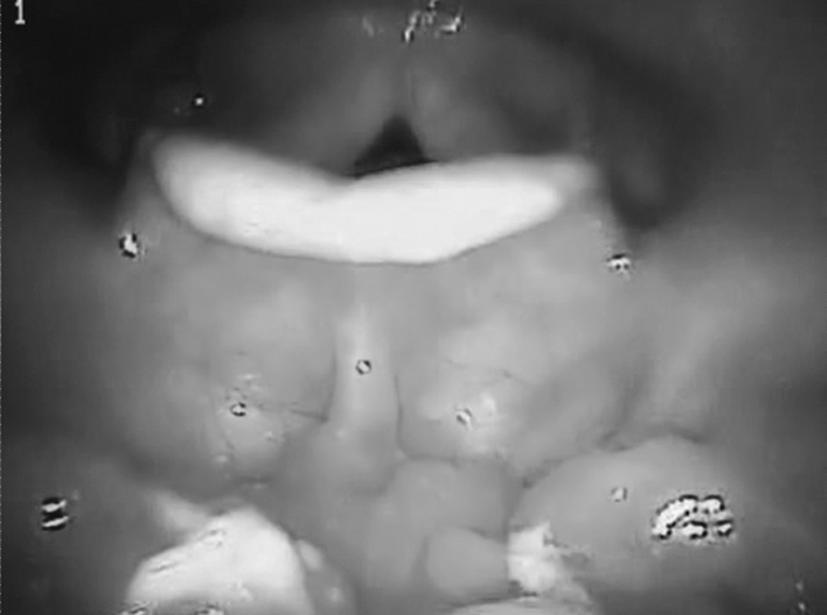
A retraction suture of 2-O silk was placed in the midportion of the oral tongue, and excellent exposure of the lingual thyroid gland was therefore established. Under endoscopic guidance using a 10-mm 30-degree laparoscope, a Harmonic shears (ACE-23p; Ethicon Endo-Surgery, Cincinnati, OH) was used to incise the mucous membrane adjacent to the attachment of the lingual thyroid. A cleavage plane between the thyroid and tongue musculature could be appreciated, and was divided in sequential fashion using the Harmonic shears (Fig. 4).

Endoscopic-assisted resection of lingual thyroid gland with Harmonic shears.
Once the plane was developed anteriorly and on either side of the lingual thyroid, a clamp was used to grasp an edge of the thyroid gland to afford retraction. This facilitated the final resection cuts posteriorly, where the exposure was somewhat limited. Steam generated by the ligation of tissue with the Harmonic was simultaneously evacuated.
At the completion of the resection, small areas of bleeding were sealed with the Harmonic, and the resection bed was left unreconstructed to heal by secondary intention, similar to a lingual tonsillectomy.
The patient was observed in the recovery room according to routine protocol, and was discharged to home ∼2 hours after the procedure. She was maintained on a liquid and then soft diet for a period of 10 days, at which time the lingual bed was observed to be healing rapidly (Fig. 5). Postoperative laryngoscopic examination of the surgical bed can be viewed (see Supplementary Video). The patient is now >3 years out from surgery with no recurrence.
Postoperative flexible laryngoscopy demonstrating absence of lingual thyroid and healing tongue base.
Discussion
The occurrence of a lingual thyroid is uncommon (1), and the need for surgical resection of this condition is even more rare (3). Indications for surgery include the same as for a eutopic thyroid gland (concern for malignancy, thyrotoxicosis, and obstructive symptoms) and in the current case was represented by the obstructive nature of her lesion, which had caused a difficult intubation and concomitant onset of dysphagia.
Techniques for the removal of a lingual thyroid that have been published are often quite invasive and are associated with substantial patient morbidity and prolonged hospitalizations. These include lip- (5) and mandible-splitting access (6), cervical approaches (7), and even lip degloving (8).
Transoral ultrasonic resection of the lingual thyroid gland is a nearly bloodless, low-morbidity, and outpatient procedure associated with rapid recovery. The impact on our patient was minimal, and therefore associated with excellent patient satisfaction. She is now >3 years out from surgery with no recurrence.
We have provided a well-illustrated documentation of this technique, which can be performed by any surgeon trained and skilled in transoral techniques and familiar with Harmonic and endoscopic technologies. It does require a skilled assistant to complete the resection. This report is necessarily limited by the lack of surgical volumes, although this will be a limitation of any report on this condition because it is so rare.
Conclusions
The occurrence of a lingual thyroid gland is uncommon, and the need for resection is more uncommon. When surgery becomes necessary, the addition of technology, consisting of endoscopic guidance and Harmonic vascular control, affords the ability to accomplish a safe minimally invasive outpatient procedure.
Disclosure Statement
There was no financial or material support for this research and work. D.J.T. has directed a series of thyroid courses sponsored by Johnson and Johnson. M.W.S. and R.B.V. have no financial disclosures.
Footnotes
Presented at the Triological Society Southern Section Meeting, Bonita Springs, Florida, January 2009.