
Abstract
Background:
Three types of cervical thymic anomalies have been described: ectopia, thymic cyst, and thymoma. Thymic cysts are very rare causes of benign neck masses in adults and are usually not diagnosed before surgery. Their prevalence is less than 1% of all cervical masses, and they are usually noted in childhood. We systematically reviewed the literature concerning cervical thymic cysts (CTCs) in adults.
Summary:
We identified 36 adult patients with a CTC. Our analysis included age, gender, cyst size, location, type, symptoms, time from cyst appearance, treatment, pathology, and follow-up. The male/female ratio was 4/5, the mean age was 36 years. Most of the cysts were asymptomatic masses diagnosed by pathology. In only one case did the differential diagnosis include a thymic cyst. Surgery should be considered the treatment of choice, but the size and location of the lesion and its relationship to nearby vital structures should be defined as clearly as possible preoperatively. Excision can be made via a transverse cervical incision. It may be a demanding procedure because of the close anatomical relationship of the CTCs with the carotid sheath and major nerves of the neck (recurrent laryngeal nerve, glossopharyngeal nerve, hypoglossic nerve, and phrenic nerve), particularly if there is adherence of the CTC with those structures.
Conclusions:
CTCs are uncommon lesions causing neck swelling and are often misdiagnosed preoperatively. Surgical excision and histological examination of the specimen usually makes the diagnosis. The existence of normal thymus gland in the mediastinum should be confirmed intraoperatively, but this is not critical in adult patients. A CTC should be included in the differential diagnosis of cervical cystic masses.
Introduction
Three cervical thymic anomalies have been described. These are ectopic thymus, thymic cyst, and thymoma (4 –6). Cervical thymic cysts (CTCs) are uncommon causes of cervical swelling but should be considered in the differential diagnosis of neck masses (2). Although they are a well-defined entity, they are still frequently misdiagnosed (7,8). Their prevalence is less than 1% of all cervical masses, and they are usually noted (75%–85% of all cases) in childhood (8 –10). CTCs have rarely been described in adults (11,12). Thus, of the more than 150 cases of CTCs with pathology confirmation only a few were described in adults (11 –13). Here we review the literature concerning CTCs in adults.
One of the first descriptions of a CTC in adults was by Lane in 1960 (14). We found 20 publications since 1960 describing 35 well-documented cases of CTCs in adult patients (1,2,4,5,7,11 –26). By our criteria, well-documented reports contained information on at least seven characteristics. These included age, gender, cyst size, location, type, symptoms, time from cyst appearance, treatment, pathology, and follow-up. Thirteen of the patients (36%) were described in two articles, eight in 1978 by Guba et al. (2) and five recently by Silverman et al. (26). Among the 35 adults with CTCs, and an additional patient described later in this review, there were 16 men and 20 women. Their age averaged 36 years, ranging from 18 to 77. The majority of cysts were located in the left neck (64%). The rest were located in the right side of the neck (19.4%) or in the midline (16.6%). There is no explanation for the left predominance of CTCs. One CTC was found at autopsy (1), and two others were incidentally discovered during surgery for thyrotoxicosis (2,17). In most patients, the presentation was one of cervical swelling, but only 9 of them (23.3%) had symptomatic swelling. The most common symptoms were dyspnea, dysphagia, and hoarseness. Cervical swelling was first noted a few days to 36 months before surgery. All CTCs were unilateral and excised via a traverse cervical incision. About half extended to the upper mediastinum where there was a connection to the normal thymus gland. The connection was direct or by a fibrous cord. None of the patients required sternotomy. The cysts averaged 4.54 cm in size and ranged from 0.9 cm to 10.5 cm. Data concerning details about the cyst anatomy were available in 27 patients (77%). Fifteen cysts (55.5%) were unilocular, and the rest of them were multilocular. Preoperatively, most of these lesions were not thought to be CTCs but were thought to be thyroid, parathyroid, or branchial cleft cysts. In almost all cases, the diagnosis was made postoperatively by histopathology, the finding of thymic tissue and Hassal's corpuscles being diagnostic for a CTC. Only a minority of reports (18.2%) included follow-up information and, among these, there were no recurrences. In 2004, Moran et al. (24) reported three patients with “an unusual variant of carcinoma arising in multilocular CTCs.” In two patients, the histology pattern was similar to basaloid carcinoma of the thymus; in one case, “the pattern was that of squamous cell carcinoma.” This is the only report of malignancy in CTCs in adult patients; however, malignant transformation of thymic cysts in the medistinum has been already mentioned in three cases (27 –29). Table 1 summarizes the characteristics of CTCs in adults.
n/a, not available.
CTCs are more common in the pediatric population before puberty (2–12 years), perhaps because at that age the thymus gland attains its greater development (9,30). In that population, the cysts are larger (10,31), are more likely to occur in males (13), and are typically slowly growing asymptomatic masses. However, when symptoms occur in children, their severity tends to be greater than in adults (8,32). On rare occasions, CTCs in infants may become infected or hemorrhage (7,33).
The mechanism for the development of CTCs is unclear. An early paper by Speer (34) described five theories. Today, most hypothesize that CTCs are either congenital, due to persistence of the thymopharyngeal duct, or acquired, due to degeneration of Hassal's corpuscles within the remnants of ectopic thymus (8,9). The frequent association of CTCs with thyroid or parathyroid inclusions would seem to favor the first theory (3).
Due to the cystic nature of CTCs, preoperative evaluation should include clinical examination and imaging techniques (notably ultrasonography, computed tomography [CT], and magnetic resonance imaging [MRI]). Ultrasonography should confirm the cystic nature of the lesions, whereas CT visualizes the lesion's margins and its relationship to the adjacent structures. MRI, when performed, provides precise data of the cyst and its surroundings (9,35). If a CTC is suspected before surgery, an MRI is especially usefully to determine whether a thymus is present. If a thymus is not present and the patient is not an adult, the CTC should probably be left in place to avoid removing the only thymic tissue present in the patient. However, in all but one patient to date (21), a CTC was not suspected before surgery. If a CTC is not suspected before surgery, but evidence for it is noted during surgery, there should be an attempt to determine whether the patient has a thymus. If no thymus is present, and the patient is at any age when thymic function is important, the CTC should not be removed unless there are compelling reasons for doing so.
The differential diagnosis for lateral cystic neck masses includes common branchial cleft cyst, thyroglossal duct cyst, cystic hygroma, dermoid cyst, cystic teratoma, lipoma, cystic lymphadenopathy-lymphoma, and cystic metastases (5,11). Less frequent causes are thyroid and parathyroid cysts, cystic neuroma, hemangioma, laryngocele, hymphangioma, and venus malformations (7,36). Due to their infrequent occurrence and location, CTCs are and often misdiagnosed before surgery as branchial cleft cysts (37).
Macroscopically, CTCs are soft, unilocular, or more frequently multilocular masses. Multilocular CTCs are more often noted in the mediastinum and in this location tend to be accompanied by significant inflammation and fibrosis (38). The wall size of a CTC varies from a few mm to 1 cm, and the wall is usually irregular (5). The cyst fluid may be clear, straw-colored, red, brown, gelatinous, or even purulent. It may be semisolid due to necrotic debris, blood, and cholesterol crystals (5,39). Pathognomonic findings in the cyst's wall, supporting the diagnosis of thymic cysts, are thymic parenchyma, lymphoid tissue, and Hassal's corpuscles (5). The cyst wall may be lined with cuboidal, columnar or spindle, stratified, epithelium that may or may not be ciliated (6,32). In the patient described later, as well as in other reports, the CTC may contain elements of parathyroid tissue (3). The common embryological descent from the fourth pharyngeal pouch and their failure to descend further may explain this coexistence. Another explanation may be that some primordial thymic cells are multipotent with an ability to differentiate into parathyroid cells within the cyst (10).
Careful surgical exploration is the appropriate diagnostic procedure for neck CTCs and other neck masses whose nature is unclear. Excision can be made by a transverse cervical incision. The procedure is demanding because of the close anatomical relationships of CTCs with large vessels and neck nerves (carotid artery, jugular vein, vagus nerve, glossopharyngeal nerve, hypoglossic nerve, phrenic nerve, and recurrent laryngeal nerve), particularly if there is adherence of the CTC with those structures (6,11). For example, due to their similar evolution during embryological development, the CTC may be abherent to the carotid sheath. CTCs may also present surgical challenges if the cyst extends in to the mediastinum. In this situation, a medial sternotomy maybe required to remove the entire specimen. Rarely, the thymus is absent in the mediastinum, and CTC or the fibrin cord are the only available thymic tissue. In that case, the treatment of children and adults should differ. In children with no other thymic tissue, the CTC should generally be preserved (9,11,13).
CTCs, once removed by surgery, usually do not recur and the long-term prognosis is excellent (33).
Illustrative Patient
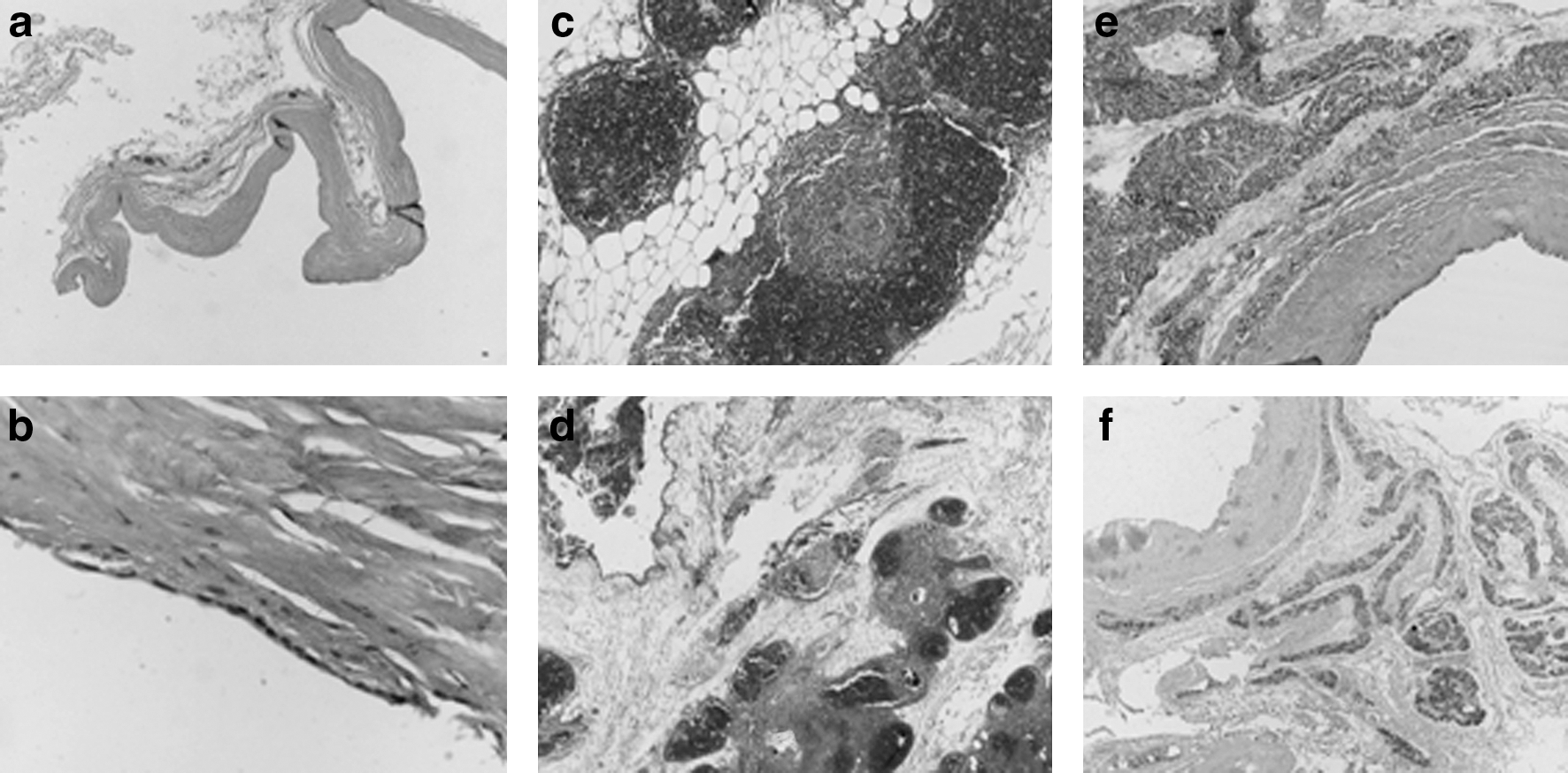
A 34-year-old male patient was referred to our department for the evaluation of unilateral cervical mass. The patient had a 2-year history of asymptomatic left-sided neck swelling, more apparent in the 6 months before presentation. Physical examination revealed a palpable, soft, non-tender mass the size of a small orange in the inferior portion of the left lateral neck. X-ray examination showed a left lateral mass dislocating the trachea. CT of the neck and the thorax demonstrated a cystic lesion occupying the inferior left lateral neck and the upper anterior mediastinum. MRI demonstrated a well-encapsulated, monolocular, not enhanced, cystic mass with thin walls that extended to the anterior mediastinum (Fig. 1). The cystic portion of the mass was surgically explored and resected. It originated from the thymus. The resected specimen was 9.5 × 5 × 6.5 cm in size (Fig. 2). Pathology examination revealed a large cystic lesion with a thin wall of fibrous tissue lined by cuboid or flattened epithelium. Normal thymus parenchyma with Hassall's corpuscles was identified in the periphery of the cyst. Some of the Hassal's corpuscles were beginning to degenerate. In a small area of cyst's wall we identified parathyroid tissue that stained positive for parathyroid hormone (Fig. 3). The postoperative course was uneventful, and the patient was discharged the second postoperative day. The patient's follow-up cervical ultrasound and CT 2 years after surgery demonstrated no recurrence of the cyst.


The patient just described has not been previously reported. His presentation and clinical course is typical for most CTCs. Similar to most other CTCs, the diagnosis of a CTC was not given serious consideration before surgery.
Summary and Conclusions
In summary, CTCs in adults are uncommon lesions causing neck swelling and are often misdiagnosed preoperatively. Surgical excision and histological examination of the specimen are required for the diagnosis. In adults, it is probably not essential to confirm that a thymus is also present before surgery, as the thymus is typically involuted in the adult and is much less important for immunological functioning than in children. CTCs, although rare, should be considered in the differential diagnosis of cervical cystic masses.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.