
Abstract
Background:
This study investigated the value of postoperative stimulated thyroglobulin (Tg) combined with neck ultrasonography for the prediction of the posttherapy whole-body scanning (RxWBS) and the efficacy of ablation with 30 mCi 131I in patients with thyroid cancer and low risk of recurrence to identify those who do not require ablation or only need a low 131I activity.
Methods:
A total of 237 consecutive patients with well-differentiated thyroid cancer and low risk of recurrence who were initially treated by total thyroidectomy followed by remnant ablation with 1.1 or 3.7 GBq (30 or 100 mCi) 131I were studied. Neck ultrasonography, Tg after levothyroxine withdrawal, and anti-Tg antibodies (TgAb) were obtained before, and RxWBS was performed 7 days after 131I administration. Patients with TgAb were excluded.
Results:
Postoperative ultrasonography revealed lymph node metastases in 5/237 (2%) patients. RxWBS showed ectopic uptake in 3/232 (1.3%) patients with negative ultrasonography. The negative predictive value of postoperative stimulated Tg <1 ng/mL (n = 132) or <10 ng/mL (n = 213) combined with negative ultrasonography was 100%. Among patients with detectable postoperative stimulated Tg <10 ng/mL and negative ultrasonography, 50 received 1.1 GBq 131I and 31 received 3.7 GBq. In the control assessment, stimulated Tg <1 ng/mL and neck ultrasonography without anomalies were achieved in 47/50 (94%) and in 29/31 patients (93.5%). All patients with stimulated Tg ≤1 ng/mL, negative TgAb, and normal ultrasonography before ablation continued to show the same results 8–12 months after initial therapy as expected, irrespective of the administration of 1.1 GBq (n = 82) or 3.7 GBq 131I (n = 50).
Conclusions:
Measurement of stimulated Tg combined with neck ultrasonography after total thyroidectomy may exclude the need for ablation in 56% of low-risk patients without TgAb (Tg <1 ng/mL) and permit the administration of an activity of 1.1 GBq 131I in another 34% with low Tg levels.
Introduction
Specifically in the low-risk group, diagnostic whole-body scanning (DxWBS) is no longer recommended during follow-up (1,2); therefore, one of the arguments in favor of ablation, that is, improvement of DxWBS sensitivity, can no longer be applied. Another argument in favor of ablation, that is, improvement of the specificity of thyroglobulin (Tg), does not apply to those patients in whom Tg is undetectable after thyroidectomy. The possibility of detection of unsuspected metastases by posttherapy whole-body scanning (RxWBS) is another argument in favor of ablation, but a close correlation is observed between the results of this imaging method and preablation Tg levels (1,2,4 –7). For these reasons, it has been proposed that ablation is not necessary in patients with undetectable postoperative Tg (1 –3). However, many investigators argue that this parameter does not exclude the possible detection of metastases by RxWBS and defend ablation for all patients (8 –10). In fact, the absence of persistent metastases must be confirmed to exclude the need for ablation; therefore, to make this decision based on postoperative Tg, this method indeed must have an excellent negative predictive value (NPV).
Excluding the interference of anti-Tg antibodies (TgAb), the main factor limiting postoperative Tg sensitivity is the presence of nonpalpable lymph node metastases that might be associated with low levels of this marker (4,5,8,9,11). Ultrasonography is currently the most sensitive imaging method for the detection of these metastases (1,5). Thus, it seems reasonable to assume that a combination of ultrasonography and Tg significantly increases the sensitivity and NPV of postoperative evaluation (5). In addition, since the NPV of preablation Tg depends on the prevalence of the disease in the population studied, it is likely that in many studies this value is higher in the low-risk group, with this distinction being important (3).
Another aspect of ablation with 131I in low-risk patients, considering the correlation between serum Tg levels and tissue volume (2) and that 30 mCi 131I is able to promote ablation when remnant tissue is discrete (12), is that low postoperative Tg values might be used as predictors of the success of ablation with a low radioiodine activity.
Therefore, the objective of the present study was to evaluate the value of postoperative stimulated Tg combined with ultrasonography for the prediction of the RxWBS result and of the efficacy of ablation with a low 131I activity in patients with low risk of recurrence to identify those who do not require ablation or only need to be submitted to ablation with 30 mCi 131I.
Materials and Methods
A total of 237 consecutive patients with well-differentiated thyroid carcinoma considered to be at low risk of recurrence (tumor ≤4 cm, no extensive extrathyroid invasion, and no lymph node involvement upon preoperative ultrasonography and perioperative examination) who were initially treated by total thyroidectomy (without prophylactic central neck lymph node dissection) followed by remnant ablation with 131I were studied. All patients had apparently complete tumor resection and a preoperative chest X-ray and postoperative clinical examination revealed no anomalies. Patients with unifocal intrathyroid tumors ≤1 cm were excluded. The characteristics of the patients studied are shown in Table 1. The study was approved by the Research Ethics Committee of our institution.
Neck ultrasonography was performed before ablation within a minimum period of 12 weeks after surgery. All suspected lesions apparent on ultrasonography (13,14) were evaluated by ultrasonography-guided fine-needle aspiration biopsy.
Ablation with 131I was performed 3–6 months after thyroidectomy. During this interval, the subjects were maintained on thyroid-stimulating hormone (TSH) <0.5 mIU/L. The patients were prepared by levothyroxine (L-T4) withdrawal for 4 weeks and received instructions regarding limiting exposure to environmental iodine and using a low-iodine diet for 2 weeks before 131I therapy. TSH, Tg, and TgAb were measured immediately before the administration of 131I. The patients received 1.1 or 3.7 GBq (30 or 100 mCi) 131I without undergoing DxWBS. Hormonal therapy was reintroduced 48 hours after radioiodine administration. Anterior and posterior whole-body images were obtained 7 days after iodine administration (RxWBS), and the scans were analyzed by three experienced nuclear medicine professionals.
The patients were reevaluated 8–12 months after initial therapy. Ablation was considered to be successful if stimulated Tg ≤1 ng/mL (after L-T4 withdrawal or recombinant human TSH administration), TgAb were negative, and neck ultrasonography showed no anomalies (1,2).
Tg was measured by a radioimmunometric assay (ELSA-hTG; CIS Bio International), with a functional sensitivity of 1 ng/mL. TgAb were determined by a chemiluminescent assay (Nichols Institute Diagnostics [detection limit of 1 IU/mL and reference value of up to 2 IU/mL] or Immulite 2000 [detection limit of 20 IU/mL and reference value of up to 40 IU/mL]). TgAb-positive patients were excluded.
Results
Postoperative ultrasonography
Ultrasonography revealed cervical lymph node metastases (confirmed by fine-needle aspiration biopsy) in 5/237 (2%) patients. The number of metastatic lymph nodes detected by ultrasonography ranged from 1 to 4 (mean = 2) and the size of these lymph nodes ranged from 6 to 12 mm. Among the 232 patients with negative ultrasonography for metastases, thyroid remnants were detected in 50 (21.5%) and residual thyroid volume was never >1.5 cm3.
Posttherapy whole-body scanning
RxWBS showed ectopic uptake corresponding to the lymph nodes seen by ultrasonography in three patients and revealed metastases in 3/232 (1.3%) with negative ultrasonography, including extracervical (pulmonary and mediastinal) metastases in 2. Among the 231 patients with RxWBS without metastases, uptake in the thyroid bed was observed in 220 (95.2%) and was ≤2% in all of them.
Correlation between postoperative stimulated Tg and imaging methods
Postoperative stimulated Tg was <1 ng/mL in 132 patients (stage T1 in 40, T2 in 52, and T3 in 40) and none of them had metastases on ultrasonography or RxWBS. Eighty-five patients (stage T1 in 20, T2 in 32, and T3 in 33) having Tg >1 and <10 ng/mL and 4 of these patients (4.7%) had persistent metastases as detected by ultrasonography and supported by RxWBS in 2 patients. Finally, Tg was >10 ng/mL in 20 patients (stage T1 in 2, T2 in 6, and T3 in 12), including 4 (20%) with metastases (detected by ultrasonography in 1 and by RxWBS in all of them).
Further, all patients with metastases detected by RxWBS but not by ultrasonography had stimulated Tg levels >10 ng/mL (RxWBS detected metastases in 3/19 [15.8%] patients with Tg >10 ng/mL and normal ultrasonography). The NPV of postoperative stimulated Tg <1 ng/mL (n = 132) or <10 ng/mL (n = 213) combined with negative ultrasonography was 100%.
The results obtained for patients with persistent metastases are shown in Table 2.
LN, lymph node metastases; RxWBS, posttherapy whole-body scanning; Tg, thyroglobulin.
Correlation between postoperative stimulated Tg and outcome of ablation
Among patients with detectable postoperative stimulated Tg <10 ng/mL and negative ultrasonography (n = 81), 50 received 1.1 GBq 131I and 31 received 3.7 GBq. The two groups were similar in terms of gender, age, tumor histology and stage, and Tg levels. In the control assessment performed 8–12 months after ablation, stimulated Tg <1 ng/mL and neck ultrasonography without anomalies were achieved in 47/50 (94%) patients and in 29/31 (93.5%), respectively. Five patients had detectable Tg alone.
All patients with stimulated Tg ≤1 ng/mL, negative TgAb, and normal ultrasonography before ablation continued to show the same results 8–12 months after initial therapy as expected, irrespective of the administration of 1.1 GBq (n = 82) or 3.7 GBq 131I (n = 50).
Among patients with postoperative stimulated Tg >10 ng/mL and negative ultrasonography (n = 19), 7 received 1.1 GBq 131I and 12 received 3.7 GBq. In the control assessment, ablation was considered to be successful in three (43%) and nine (83.3%) patients, respectively; four patients had elevated Tg alone and three had detectable Tg and apparent disease.
Discussion
Persistent metastases after total thyroidectomy are uncommon in patients with a low risk of recurrence. In fact, in the present study only 3.4% of these patients had metastases on postoperative ultrasonography or RxWBS. Postoperative assessment of these patients is more useful to define ablation and the 131I activity to be administered. Considering that low-risk patients with undetectable stimulated Tg and normal neck ultrasonography after ablation are considered to be free of disease (1,2), it is reasonable to assume that adjuvant therapy with 131I is not necessary for those patients who, even before ablation, have these results. The fact that DxWBS is no longer recommended for the follow-up of this group (1,2) weakens the argument that ablation increases the sensitivity of this test. Improvement of the specificity of Tg with ablation does not apply to these patients who already have undetectable stimulated Tg with surgery only. Finally, in many studies preablation Tg levels ≤1 ng/mL were associated with negative RxWBS in almost all patients (6,7,15 –18). Although low postoperative Tg does not rule out the possibility of detection of lymph node metastases by RxWBS (4,5,8,9,11), its combination with neck ultrasonography, the most sensitive method for the detection of these metastases (5), significantly increases the NPV. In fact, RxWBS was negative for metastases in 100% of the low-risk patients with Tg-ablation ≤10 ng/mL and negative postoperative ultrasonography (n = 213).
Some authors contest the excellent NPV of postoperative Tg (8 –10). We believe that the data of those studies are not applicable to the situation studied here, that is, the specific group of low-risk patients with postoperative Tg ≤1 ng/mL and negative neck ultrasonography. Patients with poorly differentiated tumors, incomplete tumor resection, and high risk of recurrence, or those undergoing previous treatment with 131I are not part of the discussion. In the series of Park et al. (9), 86.5% of patients with metastases seen on RxWBS and Tg ≤2 ng/mL had lymph node metastases, and 57.7% of them were stage III or IV, and, therefore, high risk. In the study of Phan et al. (10), analyzing specifically low-risk patients with undetectable Tg-ablation, none of the patients had metastases on initial RxWBS. Brendel et al. (8), using a cut-off value of 3 ng/mL, identified 19/224 patients with negative stimulated Tg and metastases detected by RxWBS. Ten patients had cervical metastases, however, and 58% of patients with extracervical metastases had moderately differentiated follicular carcinoma, and no stratification regarding recurrence risk was provided.
After demonstration of the excellent NPV of postoperative Tg ≤1 ng/mL in the low-risk group, it remains to be determined whether this level can be achieved in a good part of these patients. According to Schlumberger (19), after total thyroidectomy 95% of patients without persistent disease have Tg/T4 ≤1 ng/mL and 80% have stimulated Tg ≤1 ng/mL. In the present study, 56% of the patients had stimulated Tg levels ≤1 ng/mL before ablation and these Tg levels were also achieved in other studies in ≥50% of cases submitted to thyroidectomy only (3,5,15,20). In contrast, there are series in which postoperative Tg levels <2 ng/mL were only obtained in 10% of patients (7). This variation might be related to the surgical technique and extent of surgery and may also be influenced by the time when Tg was measured since this marker can remain elevated for some weeks after thyroidectomy (1,2,13). Therefore, in the present study the measurements were obtained 12 weeks after surgery.
Candidates for ablation with 131I, low-risk patients with Tg-ablation levels between 1 and 10 ng/mL and negative ultrasonography might be treated with a low 131I activity (30 mCi). In the present study, this group corresponded to 34% of the patients. No metastases were detected by RxWBS in any of these patients and an activity of 30 mCi resulted in successful ablation in 94%. If we consider the correlation between tissue volume and Tg levels (2), a discrete residual volume should be taken into account if postoperative Tg is low. In fact, even in these patients with detectable Tg, the thyroid remnant volume was discrete upon ultrasonography (this study). Particularly in this situation, 30 mCi is known to be sufficient to promote ablation of residual tissue (12).
One limitation of the proposal of the present study (indication and definition of 131I activity in low-risk patients based on Tg and postoperative ultrasonography) is that Tg may remain elevated and ultrasonography might be compromised due to postoperative alterations for several weeks after surgery (5,13). As a consequence, Tg measurement and ultrasonography should be performed ∼3 months after thyroidectomy; therefore, L-T4 therapy should be initiated early after surgery, maintaining TSH levels low until the time for the evaluation proposed.
In conclusion, measurement of stimulated Tg combined with neck ultrasonography after total thyroidectomy may exclude the need for ablation in 56% of low-risk patients without TgAb (Tg ≤1 ng/mL) and permit the administration of an activity of 1.1 GBq 131I in another 34% (low Tg levels). On the basis of these results, a proposal for the selection of patients who do not require ablation or only need a low 131I activity, including the current availability of recombinant human TSH, is summarized in Figure 1.
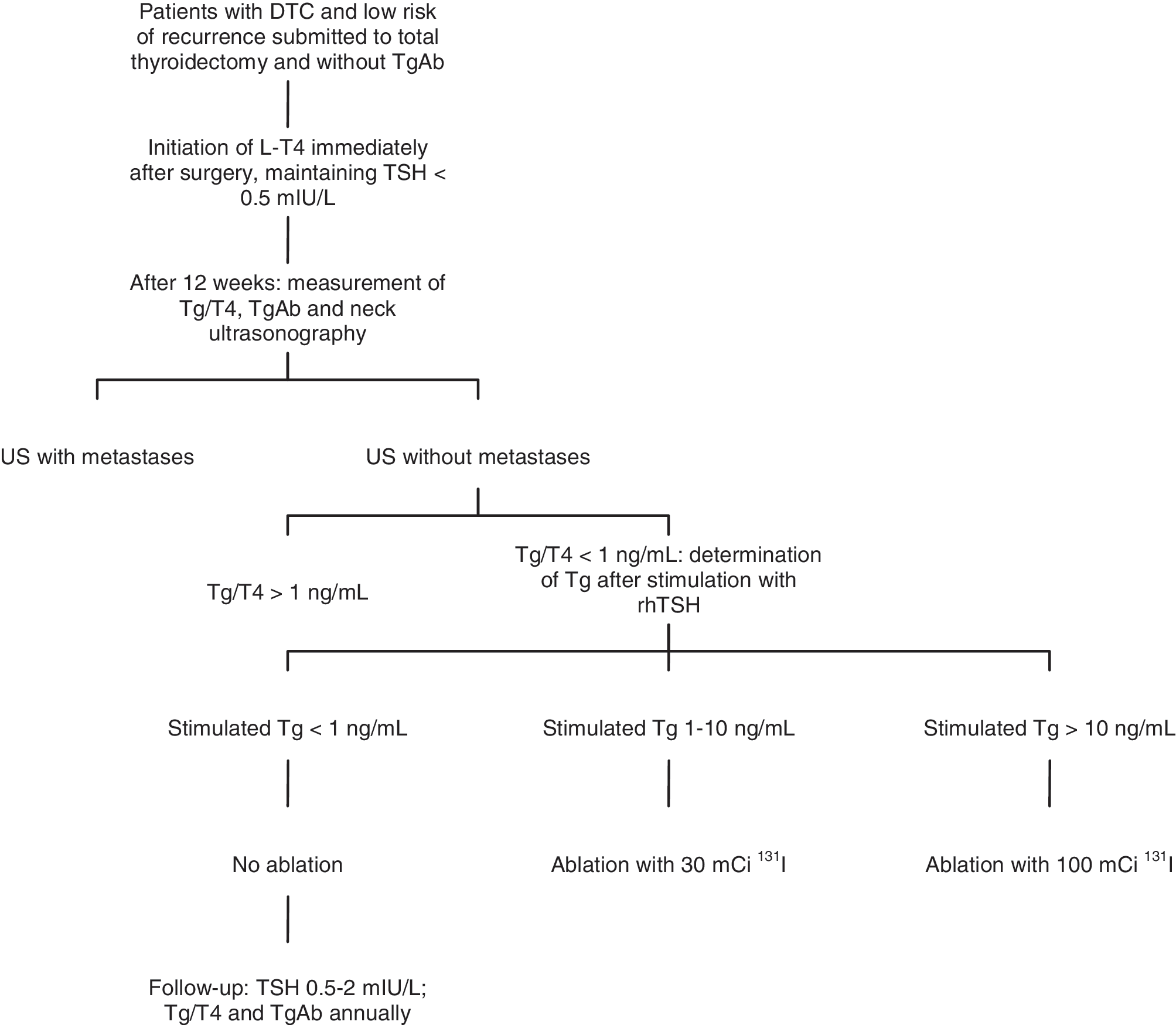
Proposal for the selection of patients who do not require ablation or only need a low 131I activity. DTC, differentiated thyroid cancer; TgAb, antithyroglobulin antibodies; Tg/T4, thyroglobulin measured during therapy with levothyroxine (L-T4) and low thyroid-stimulating hormone (TSH); rhTSH, recombinant human TSH; US, ultrasonography.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.