
Abstract
Background:
Although clinically evident metastases of nonthyroid malignancies (NTMs) to the thyroid gland are uncommon, it is important to suspect them in patients who present with a new thyroid mass and a history, however far back, of prior malignancy. In fact, metastases from NTMs to the thyroid gland have been reported in 1.4%–3% of all patients who have surgery for suspected cancer in the thyroid gland. Here we review the literature over the last decade regarding this topic.
Summary:
Based on recent literature, the most common NTMs that metastasize to the thyroid gland are renal cell (48.1%), colorectal (10.4%), lung (8.3%), and breast carcinoma (7.8%), and sarcoma (4.0%). Metastases of NTMs to the thyroid are more common in women than men (female to male ratio=1.4 to 1) and in nodular thyroid glands (44.2%). The mean and median intervals between diagnosing NTMs and their metastases to thyroid gland are 69.9 and 53 months, respectively. In 20% of cases the diagnosis of the NTM and its metastases to the thyroid was synchronous. Recent reports indicate that there is a higher frequency of sarcoma metastasizing to the thyroid gland than reported in prior years. Fine-needle aspiration biopsy (FNAB) of thyroid masses is useful in diagnosis of thyroid metastases. However, this requires information about the NTM so that the proper antibodies can be used for immunohistochemical analysis; therefore it is of lesser utility if the NTM is occult. In patients with preexisting thyroid pathology the FNAB diagnosis can be more difficult due to more than one lesion being present.
Conclusions:
It is important to keep in mind that the thyroid gland can be a site of metastases for a variety of tumors when evaluating a thyroid nodule, especially in a patient with a prior history of malignancy. In patients with thyroid lesions and a history of malignant disease, regardless of time elapsed since the initial diagnosis of the primary neoplasm, disease recurrence or progression of malignancy must be considered until proven otherwise.
Introduction
On the other hand, some suggest that although clinically apparent metastases of NTMs to the thyroid gland are uncommon, they are no longer considered to be rare. Metastases from NTMs to the thyroid gland have been reported in 1.4%–3% of all patients who have surgery for thyroid malignancy (3,7 –11). The most commonly reported NTMs leading to clinically discovered metastases to the thyroid are renal cell carcinoma (RCC), and lung, colorectal, and breast carcinoma (7,10 –12). Older autopsy studies report a wide range of prevalences, from 1.9% to 24%, for metastases of NTMs to the thyroid (10,11). In autopsy studies, the most frequently encountered NTMs that metastasize to the thyroid are breast, lung, and melanoma (11,13).
One question that has been addressed in the literature is whether metastases from NTMs have more of a predilection for abnormal thyroid glands compared with normal glands. If the hypothesis of Willis is correct, diseased thyroid glands with reduced blood flow and lower iodine concentrations should be more susceptible to metastases. In 2000, Kameyama et al. reported only five cases of carcinoma metastatic to a thyroid adenoma in the literature, thus suggesting that tumor-to-tumor metastases are rare occurrences (14). In 2005 Peteiro et al. also noted that metastases to a preexisting thyroid neoplasm are rare (15). However, other studies have shown that metastases to the thyroid occur more frequently in diseased glands (16). In particular, in a series by Heffess et al. using the Endocrine Registry of the Armed Forces, 42% of patients with thyroid metastases from NTMs were noted in glands with adenomas or thyroiditis (17).
Here we review the literature between 2000 and 2010 on metastases from NTMs to the thyroid gland. Although historically metastases to the thyroid gland were considered to be an uncommon but potentially lethal diagnosis, their prevalence, ease of diagnosis, and appropriate management remain controversial. The purpose of this study was to investigate the prevalence, and primary sites of metastases of NTMs of the thyroid gland and their relationship to survival. We also examined the role of fine-needle aspiration biopsy (FNAB) in the diagnosis of thyroid metastases. To our knowledge, this is the first comprehensive review in recent years of the patterns and behavior of metastases of NTMs to the thyroid gland.
Review
A review of the English-language literature from January 2000 to early 2010, and selected other articles, was conducted for articles pertaining and relevant to metastases from NTMs to the thyroid gland (1
–131). We searched PubMed for all reported cases of metastases to the thyroid from January 2000 until early 2010 using any combination of keywords from the following categories: primary malignancy (kidney, breast, melanoma, lung, colon, rectum, sarcoma, bladder, neuroendocrine, pancreatic, ovarian, cervical testicular, uterine) and abnormal thyroid glands (adenoma, goiter, multinodular goiter, nodule, thyroiditis, Grave's disease, hyperthyroidism, hypothyroidism). A combination of these terms was used to select relevant articles on metastases to the thyroid gland. Cases in which thyroid metastases was discovered by autopsy were excluded. A total of 372 cases were reported during this period. Many retrospective chart reviews and case series published during this period included cases that occurred before this date range in the analysis. Our review also included two previously unreported cases, presented here as illustrative cases, that occurred in this period (see Supplementary Table S1; Supplementary Data are available online at
Demographic distribution
Of the total of 374 NTMs with metastases to the thyroid, 207 were in women and 151 were in men, a female to male ratio of ∼1.4. In 16 cases, the gender of the patient was not noted usually because the focus was on cytology and histopathology. Age was reported in 194 cases. The mean age was 59 years (range: 26 to 87) and the median was 60 years. In individual case series the mean ages were 62, 64.6, 64.9, 67, and 52 years (9,10,17 –19).
Sources of metastases to the thyroid gland
The most frequently reported (n=180) NTM was RCC. Following RCC, the next most common NTMs were colorectal, lung, and breast carcinoma (see Supplementary Table S2) (7 –12,15 –110). Melanoma is another common malignancy that can metastasize to the thyroid gland. The same number of melanoma (n=15) and sarcoma (n=15) cases metastasizing to the thyroid gland were reported, each accounting for 4.0% of metastases from NTMs to the thyroid gland in the last decade. There were isolated reports of various cancers, including urothelial sarcomatoid, bladder cancer, endometrial adenocarcinoma and carcinosarcoma, neuroendocrine cancers, meningioma, gastrointestinal stromal tumor, intraductal papillary-mucinous carcinoma of the pancreas, ovarian cancer, undifferentiated carcinoma of the nasopharynx, testicular seminoma, and uterine carcinoma metastasizing to the thyroid gland.
Interval between primary diagnosis and thyroid metastases
Metastases of primary tumors can be divided into two categories: synchronous and metachronous. Synchronous indicates that the tumors are detected at the same time as the thyroid metastases whereas metachronous indicates that the thyroid metastases are detected some time after the NTM was first noted. Thyroid metastases can present decades after initial diagnosis and treatment for a NTM, making diagnosis of metastases to the thyroid gland even more difficult. The recent literature reflects this, with the longest interval being 21 years between the initial diagnosis of foregut neuroendocrine carcinoma and metastases to the thyroid gland (20). In another patient, metastases of liposarcoma to the thyroid occurred more than 20 years after the initial diagnosis (21). In our review we noted 261 cases of metachronous metastases; the mean interval between discovery of the primary tumor and the thyroid metastases was 69.9 months (5.8 years) and the median was 53 months, or 4.4 years. In other reviews, mean disease-free intervals of 6.8, 9.4, 10.3, and <2 years were noted (9,10,17,18). Regarding synchronous metastases, there were 69 cases (20.9%) of synchronous diagnosis of the NTM and their thyroid metastases. In some of these cases, discovery of the thyroid metastases led to diagnosis of the primary malignancy. NTMs that presented synchronously with thyroid metastases are shown in Table 1. The most common of these was RCC. In some reports the primary malignancy was very advanced when diagnosed.
RCC, renal cell carcinoma; SCC, squamous cell carcinoma.
The interval between diagnosing NTMs and discovering their metastases to the thyroid gland was longest in patients with sarcomas (mean 75 months) and shortest in patients with lung cancer (mean 4.5 months). Table 2 indicates that the mean intervals between when NTMs were discovered and when thyroid metastases were noted was 68 months for RCC, 48.2 months for breast cancer, 41.5 months for colorectal cancer, and 20.9 months for malignant melanoma.
Leiomyosarcoma (n=6), liposarcoma (n=4), malignant adenomyoepithelioma (n=1), malignant fibrous histiocytoma (n=1), phyllodes tumor (n=1), intimal sarcoma (n=1), and paraganglioma (n=1).
Metastases to abnormal thyroid glands
Most of the literature does not indicate whether there were coexisting or preexisting thyroid conditions in cases of metastases of NTM to the thyroid. Of the 156 cases in which this was indicated there were 69 (44.2%) in which thyroid metastases occurred in glands that were also otherwise abnormal. These abnormalities included primary thyroid neoplasms and benign thyroid conditions. Malignant metastases were most commonly found concomitantly with goiters and follicular thyroid adenomas (Table 3). Notably, several cases, including the first of two cases reported later in this review, occurred in the setting of a preexisting multinodular goiter or thyroid nodule. In some reports thyroid metastases were suspected because there was enlargement of a preexisting nodule or goiter (22 –27,111,112). The most commonly reported NTMs to metastasize to an abnormal thyroid gland were RCC (n=14), lung (n=3), and sarcoma (n=3). Several retrospective chart reviews noted the presence of an abnormal thyroid gland but did not state the NTM that metastasized to the thyroid. We noted 1.9% of NTMs that metastasized to the thyroid gland were from an unknown primary malignancy (see Supplementary Table S2).
In some cases, abnormal thyroid glands had more than one abnormality.
Much of the literature did not indicate what the thyroid function was of patients with metastatic disease to the thyroid. There were 170 reports that did contain this information. Most patients were euthyroid (n=149; 87.6%). Hypothyroidism, when it occurred, was related to massive infiltration of the thyroid by a malignant tumor (13). When thyrotoxicosis occurs, it is likely due to the leakage of the hormones into the peripheral blood resulting from damage to the thyroid gland by neoplastic embolization (10,111,120). Five patients were hypothyroid and eight patients were hyperthyroid at the time of NTM diagnosis. Six patients (3.5%) had a history of hyperthyroidism and 4.1% had history of hypothyroidism. Notable all six patients with a history of hyperthyroidism prior to NTM diagnosis were euthyroid at the time of NTM diagnosis. Interestingly, among all the patients without a previous history of thyroid disease, three patients (1.8%) presented with thyrotoxicosis at time their NTM was diagnosed. In these cases, thyrotoxicosis was attributed to destruction of the thyroid gland by the malignancy, thereby causing uncontrolled release of thyroxine (T4). Two patients had the sick euthyroid syndrome. Three patients were euthyroid but had slightly increased serum thyroglobulin concentrations.
Concomitant thyroid and extrathyroidal metastases
There were 293 cases for which information was provided as to whether there were also metastases to extra-thyroidal tissues. Of those there were 118 (40.3%) in which there were no extra-thyroidal metastases. In 175 cases (59.7%), extra-thyroidal metastases were either previously present or discovered when metastases to the thyroid gland were first noted.
Presentation and diagnosis of thyroid metastases
In 338 cases information was provided regarding how the metastases to the thyroid gland were diagnosed. The majority of patients presented with clinical complaints (n=253) such as new or enlarging thyroid nodule, enlarged thyroid gland, neck swelling, dysphagia, dysphonia, and cough. Four patients presented, in a dramatic manner, with a rapidly enlarging thyroid gland and respiratory compromise requiring emergency thyroidectomy or emergency tracheostomy (16,31,65,112). There were 84 cases (24.9%) in which the presentation was incidental, including the second patient described later in this review. Twenty-five patients were diagnosed in the course of a routine physical exam that revealed either a new thyroid nodule or thyromegaly. In two patients, thyroidectomy was performed for other indications and histological examination of the specimen revealed metastatic deposits within the gland (24,28). Sixty patients were incidentally found to have thyroid metastases via screening exams such as screening or staging positron emission tomography (PET) scans, computed tomography (CT) scans, Octreoscan™ (82), or neck ultrasound. In the two cases presented later, the first presented with symptomatic dysphagia and the second by staging CT.
FNAB in diagnosis of thyroid metastases
FNAB has become an important and useful tool in diagnosis of thyroid pathology, including diagnosis of malignant metastases to the thyroid gland. However, FNAB may not yield a definitive diagnosis in all cases. Of the 167 patients who underwent preoperative FNAB there were 123 cases (73.7%) where this yielded the correct diagnosis of thyroid metastases. In the 40 cases (24.0%) where the FNAB diagnosis was incorrect, primary thyroid malignancy was the diagnosis in 13 patients, benign follicular nodule in 7 patients, normal thyroid in 14 patients, and inconclusive in 6 patients. There were a few cases of concomitant primary thyroid malignancy and metastases of NTM to the thyroid. In these FNAB diagnosed the primary thyroid malignancy but not the metastases to the thyroid. In one study there was a patient in whom FNAB had to be repeated five times before the correct diagnosis was established.
As shown in Table 4, the most common NTMs for which FNAB or their thyroid metastases did not make the correct diagnosis were esophagus (50%), cervix (33%), RCC (28.5%), and malignant melanoma (20%). NTMs for which thyroid FNAB generally provided the correct diagnosis were breast (94.7%), lung (90.1%), colorectal cancer (88.5%), and sarcoma (87.5%). As noted, thyroid metastases from squamous cell carcinoma of the esophagus were especially difficult to diagnose by FNAB. One report described a patient, with esophageal cancer with metastases to the thyroid gland, who was incorrectly diagnosed as having a primary pure squamous cell carcinoma of the thyroid, a very rare condition.
FNA, fine needle aspiration.
Immunohistochemistry (IHC) is usually able to differentiate between primary thyroid malignancy and secondary malignancy. Thyroglobulin antibody staining is particularly useful, except in certain cases of anaplastic thyroid cancer (81). Immunostaining of a thyroid mass, especially if traditional histopathology is equivocal, is especially important in the patient with known history of malignancy. In this setting the appropriate antibodies can be selected for IHC based on the patient's known malignancy. The selection of antibodies for IHC is more challenging when the patient presents with occult malignancy. However, in this setting careful analysis of the thyroid metastasis may help uncover the occult tumor.
A goiter may hinder the accuracy of FNAB. To rule out and treat metastatic disease, El Fakih et al. recommended total thyroidectomy in patients with history of malignancy who had developed nodular goiters (117). Wood et al. suggested that thyroidectomy should be performed if FNAB presents a difficult diagnosis (11). As an abnormal thyroid gland may increase propensity for metastatic deposits, patients with abnormal thyroid lesions should have careful clinical follow-up and serial neck sonographic evaluations especially if initial FNAB is nondiagnostic or equivocal.
Discussion
The thyroid gland has a rich blood supply of ∼560 mL/100 g tissue/min, which is reported to be second only to the adrenal gland (1). A rise in the incidence of primary thyroid cancer is well documented (113,121,122), but the prevalence of metastases to the thyroid gland is variable in reports. Autopsy studies have shown that the prevalence of metastases of NTMs to the thyroid gland ranges from 1.9% to 24% (10,11). Our review of the literature from the last decade, however, suggests that clinically significant metastases of NTMs to the thyroid gland are not rare.
There has always been a strong female predominance in cases of differentiated thyroid cancer (113). A recent study using the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) database reported a clear difference in prevalence between men and women for differentiated thyroid cancer. They noted that the rates of differentiated thyroid cancer rise rapidly among women during the reproductive years such that the burden among women peaks around 40 years of age (123). However, it remains unclear whether or not there is any sex predominance for metastases to the thyroid gland. One study found no female predominance and postulated that this reflects the pathogenic role of parity and estrogen on primary thyroid malignancy, whereas for secondary malignancy this is not the case (10). On the other hand, one study by Nakhjavani et al. in fact observed a male predominance of 3.6:1 (3). Others have noted female predominance of metastases to the thyroid, some reporting ratios of 1.4:1 and even 6:1 (11,17,64,81). In our review, we noted a modestly high female to male ratio of metastases to the thyroid gland. Of all cases of thyroid metastases reported from 2000 to 2010, there was a female sex predominance of 1.4:1. We also noted that the mean age of presentation was 59 years. This is younger than reported in most of the past retrospective chart studies. Given that the majority of our cases were reported in the form of case reports and that malignancy and metastases are unusual in younger patients, it is possible that there was a bias toward reporting younger patients which would skew downward the mean age of presentation that we calculated.
RCC was responsible for almost half (i.e., 48.1%) of metastases of NTMs to the thyroid gland in the past decade, confirming that RCC is the most common extra-thyroidal cancer to metastasize to the thyroid gland. Similarly, in recent reports, lung, colorectal, and breast carcinomas were the next most common extra-thyroidal cancers that metastasized to the thyroid. This is also consistent with earlier studies. Melanoma, esophageal carcinoma, and stomach carcinoma are also relatively prominent among extra-thyroidal cancers that metastasize to the thyroid (39). The biggest contrast between the earlier and more recent literature was for sarcomas. We identified 15 cases of sarcoma metastasizing to the thyroid gland in the literature of the past decade—this represented 4% of metastases of NTMs. In contrast, earlier studies did not report sarcoma to be a common NTM metastasizing to the thyroid gland (2,4,6,125). The true rate for sarcomas was previously thought to be underestimated by 50% because tabulations in the early versions of the population-based databases only included sarcomas arising in soft tissues, but not those arising in specific organs such as the skin and organ sites (126,127). The higher number of sarcomas in the last decade may be attributed to the recent shifts in the World Health Organization diagnostic criteria and classification of soft tissue sarcomas (114). Further, the use of modern diagnostic techniques, increase in number of radiation treatments, and greater awareness may account for the higher than previously reported cases of sarcomas.
The time to detection of thyroid metastases after the primary tumor diagnosis was variable in our review, but was often long, similar to the earlier literature. We noted, however, short intervals between diagnosis of the primary tumor and thyroid metastases for both lung cancer and melanoma, consistent with the aggressive nature of these tumors. In addition, while the early literature noted that thyroid metastases tend to occur after or along with widespread metastases (11), our review of recent literature indicated that 40.3% of metastasis were solitary to the thyroid gland alone. This reinforces the concept that metastases to the thyroid should be seriously considered in patients having only a thyroid nodule and a history of extra-thyroidal malignancy (66). The two cases presented at the end of this review illustrate how the work-up of a thyroid nodule in a patient with a history of a prior malignancy can lead to the correct diagnosis of metastases to the thyroid gland.
Although metastases to the thyroid gland may be associated with a poor prognosis, some suggest that early detection and aggressive surgical and medical treatment may improve survival in a small percentage of patients (3). Unfortunately, in one study it was noted that the overall survival time was not significantly different in cancer patients with metastases to the thyroid gland compared with those without thyroid metastases; it was concluded that the clinical course of patients with metastases from NTMs to the thyroid gland depends on the extent of disease dissemination and the stage of the primary tumor rather than its spread to the thyroid gland (10). Further experience should be analyzed to determine the effect of thyroid gland metastases on prognosis, and the benefit of surgical resection. At present the literature is equivocal regarding the impact of surgical management on survival time. Some authors have documented longer survival in patients surgically treated versus those nonsurgically treated (8,10). In selected patients total thyroidectomy is the mainstay of surgical intervention, despite the difficulty in knowing how beneficial thyroidectomy is in patients with NTMs. In carefully selected patients where the tumor is confined to one lobe hemithyroidectomy may be appropriate as it is likely to achieve complete resection and be associated with less morbidity.
In this review, 44.2% of metastases of NTMs to the thyroid gland occurred in glands with abnormalities such as primary thyroid neoplasms and benign thyroid conditions. This supports the hypotheses that abnormal thyroid glands that have been altered by goiters, neoplasms, or thyroiditis are more vulnerable to NTMs, presumably due to abnormal blood supply resulting in decreased oxygen content and iodine content (1,119,128). One should suspect metastatic disease to the thyroid gland in a patient with preexisting thyroid gland abnormalities and perform the appropriate diagnostic assays to avoid a delay in diagnosis of NTM to the thyroid gland.
Whether there is a cause-and-effect relationship between Graves' diseases and metastases to the thyroid gland is unclear. Mete et al. reported a case of a patient with a history of endometrial carcinosarcoma who presented with thyrotoxicosis, heat intolerance, and enlarging neck mass. She underwent bilateral thyroidectomy and pathologic analysis documented Graves' disease on the left and a carcinosarcoma metastases in the right thyroid lobe (98). They postulated that cancer antigens of malignant cells invading thyroid tissue may have triggered cytokines, leading to thyroiditis. Another hypothesis for why Grave's disease might occur in patients with metastases of NTMs to the thyroid gland is that thyroid destruction and release of thyroid autoantigens may trigger autoimmunity (98). However, there are few reports of patients with a history of Graves' disease who were affected by metastases to the thyroid gland. In fact, Graves' disease may be protective against metastases to the thyroid gland because of its enhanced blood flow.
Early detection and surgical intervention, if indicated, may prevent local recurrence and the development of complications such as thyrotoxicosis, respiratory compromise, and extension into local structures such as the recurrent laryngeal nerve and trachea. This is especially true in RCC, where metastases to the thyroid gland have a propensity to extend into the jugular veins (19). The majority of cases (74.9%) initially present with clinical manifestations such as a new neck mass, neck swelling, and dysphagia. However, 25.1% are incidentally noted on physical examination or imaging studies to have metastases of NTMs to the thyroid gland. Some authors have suggested that the screening chest CT in patients being followed up with cancers should be a thyroid-chest CT not to miss thyroid metastases (25). It is likely that increasing use of imaging technologies, such as PET, have led to the increase frequency of detected metastases of NTMs to the thyroid gland.
Although RCC was the most common source of metastases to the thyroid gland, we noted that the FNAB did not yield the correct diagnosis in 28.7% of patients with RCC. Other authors noted this occurrence (42,81) and, contrary to the wide consensus that FNAB is an accurate diagnostic tool, Mijovic et al. reported a high false negative rate of 13% (118). While FNAB has the lowest rate of complications, FNAB yields only cells for cytologic examination and thus inadequate sampling is one of the major causes of false negative results. In an era in which FNAB is the most reliable and commonly used tool to assess a thyroid mass, this surprisingly high finding of an incorrect FNAB is concerning. Thus, one should remain suspicious for metastatic disease to the thyroid gland when FNAB is negative for malignant cells or indeterminate. Given the limitations of interpreting FNAB in the setting of an occult malignancy, surgical excision may be the most appropriate management in patients with a history of malignancy when FNAB is equivocal or indeterminate.
One potential limitation of reviewing literature during a specific period is that our analysis may not accurately reflect the current status of metastases of NTMs to the thyroid gland. Importantly the majority of articles on this topic, those that were published before the period that we reviewed, reported postmortem findings. It is notable that an earlier report indicated that malignant melanoma was the predominant NTM to metastasize to the thyroid gland, accounting to 39% of all metastatic neoplasms of the thyroid at autopsy (13). In contrast, during the period we reviewed, we noted that melanoma comprised 4.0% of our clinical series. This difference between these and earlier reports suggests that in many patients with advanced malignancy metastases to the thyroid are likely clinically occult, but can be uncovered by careful autopsy studies.
Illustrative Patients
Patient 1
A 61-year-old female was diagnosed with malignant melanoma of the right leg. A wide local excision and sentinel node biopsy was performed and three right inguinal nodes were removed; one node was found to have rare, small aggregates of two to three cells, which were further evaluated using immunohistochemical staining tools. The cells were positive for homatropine methylbromide-45 (HMB-45) and thought to possibly represent early micrometastases. A PET scan done at an outside hospital showed no evidence of active disease and no adjuvant treatment was given at this point. The history was positive for hypothyroidism and levothyroxine treatment. A thyroid ultrasound was performed one year later. This showed a complex nodule in the right lobe measuring 2.1×2.3 cm containing multiple cystic regions. Thyroid stimulating hormone (TSH) at the time was 1.07 μIU/dL (normal range: 0.35–5.50 μIU/L), T4 was 11.2 mcg/dL (normal range: 4.5–11.2 mcg/dL), and free thyroxine (fT4) was 1.57 ng/dL (normal range: 0.9–1.8 ng/dL). FNAB of the right thyroid nodule at this time was consistent with nodular goiter.
The patient was followed, and a PET scan 3 years after her initial diagnosis showed increased activity in the right common iliac chain, but no evidence of other sites of disease. Biopsy of the mass in the right common iliac chain revealed metastatic malignant melanoma, however the mass appeared adherent to the iliac vessels without a good tissue plane, and it was thought not to be resectable for purposes of a cure. She was subsequently enrolled in a mitogen-activated protein/extracellular signal-regulated kinase (MEK) inhibitor trial and staging CT scan at that point showed a thyroid lesion. Thyroid ultrasound at this time showed interval increase in the size of the previously observed right lobe nodule and a new lesion in the inferior pole of the right thyroid gland. Another new 2.3 mm nodule was observed in the left lobe of the thyroid. TSH at this time was 1.32 mIU/dL, T4 was 10.6 mcg/dL. Since the patient was enrolled in the MEK inhibitor study at that time, the decision was made to repeat the thyroid ultrasound in 6 months. However, she tolerated the drug poorly, and after dose reduction, CT showed widely metastatic melanoma. The patient was then placed on palliative chemotherapy. The patient responded well to treatment, and PET scan then showed no evidence of active disease. However, surveillance PET scan 5 years after her original diagnosis showed active disease in a right common iliac lymph node, and decision was made to surgically remove the mass and perform a lymph node dissection. The resection was then followed by radiation therapy.
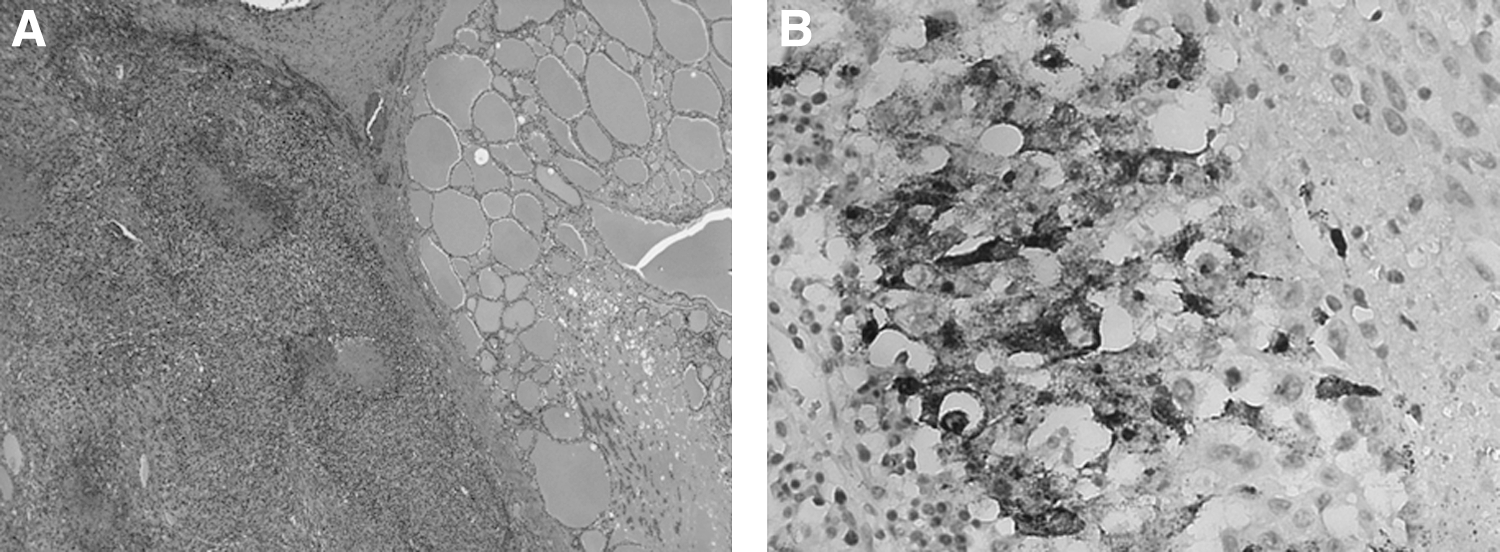
The patient then presented several months later with new complaints of dysphagia. Physical exam at this point demonstrated a diffusely enlarged thyroid gland without a discrete nodule. CT imaging showed a new left thyroid lobe mass and corresponding PET scan showed intense focal activity in the left neck corresponding to this with a standard uptake value (SUV) of 11.5 (Fig. 1). Additionally, there was a smaller focus of increased fludeoxyglucose activity (SUV of 4.5) in the right neck which corresponded to a right thyroid lobe nodule. A decision was made for total thyroidectomy. Histopathology of the thyroid showed metastatic melanoma present in the right, left, and pyramidal lobe of the thyroid (Fig. 2A). Immunostains using the antihuman melanoma antigen markers HMB-45 and melanoma-associated antigen recognized by T cells (MART-1) showed focal positive staining in the tumor in the left lobe of the thyroid, supporting metastatic melanoma (Fig. 2B). Two years after surgery, the patient died from metastatic melanoma.
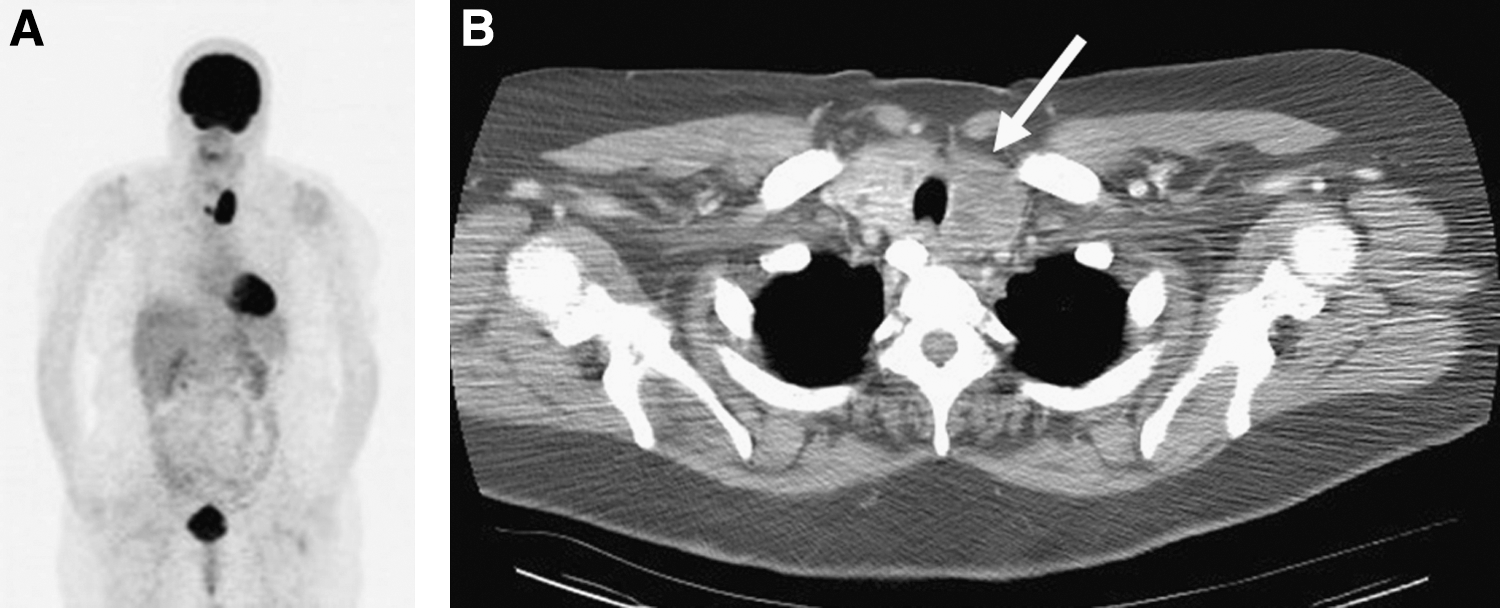
Metastatic melanoma to the thyroid gland.
Patient 2
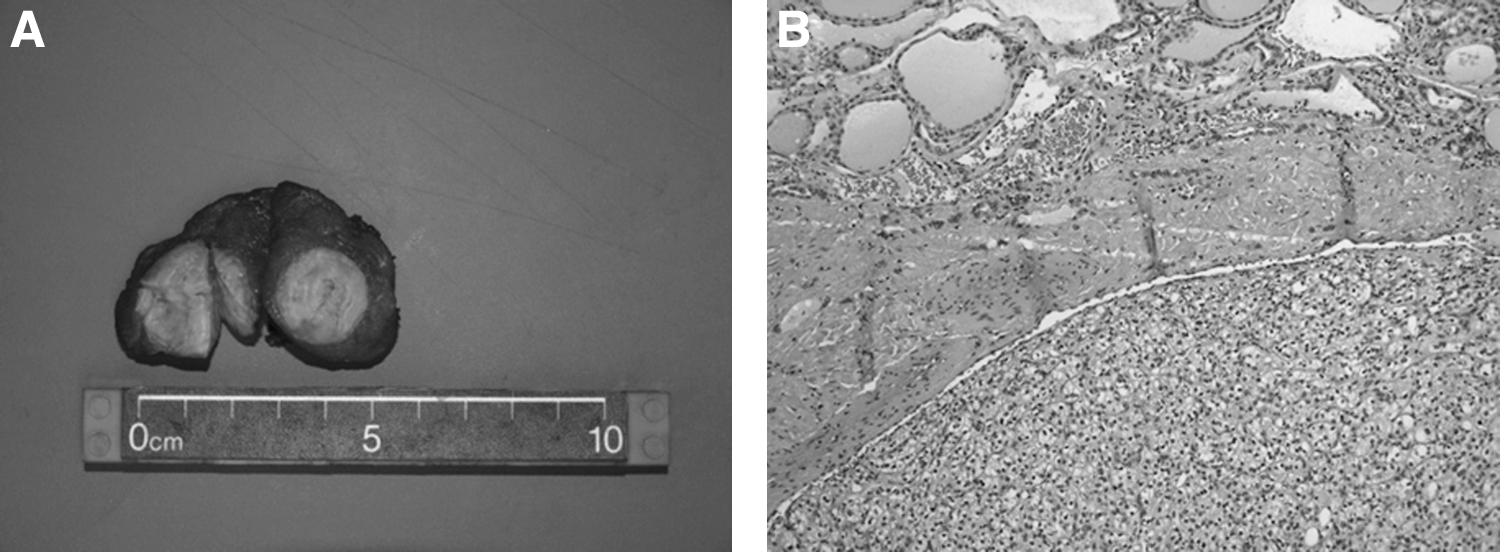
A 55-year-old male was admitted for a one year history of worsening fatigue, decreased appetite, and 40-pound weight loss. CT scan revealed a renal mass thought to be RCC, along with nodules replacing the adrenal glands bilaterally and a small lung nodule. CT of the thorax showed a left thyroid hypodensity measuring 2×2 cm. A decision was made to begin outpatient chemotherapy, with a plan to proceed with nephrectomy if the patient showed improvement with treatment. At this time, thyroid ultrasonography was performed and showed a 2.2×1.5 cm hypoechoic, heterogeneous mass in the left lobe of the thyroid with well-defined margins. Thyroid function tests were within normal limits. His fT4 was 1.17 ng/dL (normal range 0.90–1.80 ng/dL) and TSH was 2.01 μIU/mL (normal range 0.35–5.50 μIU/mL). FNAB of the thyroid mass was performed and predominantly showed thyroid follicular cells with microfollicular architecture and minimal colloid suggestive of a follicular lesion or neoplasm. Also noted was one small sheet of cells with large vacuolated cytoplasm and mild nuclear atypia, which raised concern for the possibility of metastatic RCC. Four months following the initial presentation, a partial nephrectomy and left adrenalectomy was performed. The final histologic diagnosis was RCC, Fuhrman grade 3 with metastases to the left adrenal gland. The primary neoplasm had a maximum diameter of 6.2 cm and showed extensive necrosis and invasion into the lymphatics. The patient was staged as pT1bNXM1, Stage IV. Six months following the initial operation, a right adrenalectomy was performed. Histology again showed metastatic RCC. About 2 months after the adrenalectomy, the patient underwent a left thyroid lobectomy. Frozen section during the operation was consistent with RCC, and a decision was made to perform hemithyroidectomy with wide margins, as there was no evidence of disease in the contralateral lobe. The final pathologic diagnosis was metastatic RCC (Fig. 3); immunostains showed RCC positive, common acute lymphocytic leukemia antibody (CD10) positive, thyroid transcription factor-1 negative, and thyroglobulin negative, confirming the diagnosis. Two years after surgery, the patient is doing well without evidence of disease recurrence.
The two patient cases above illustrate the diagnostic work-up for metastases of NTMs to the thyroid gland. The first case shows a patient with a benign thyroid goiter who later developed metastases to the thyroid gland. This is consistent with the concept that the persistence of thyroid abnormalities increase the risk of metastases of NTM to the thyroid gland. The second case illustrates a patient with RCC, the most common NTM to metastasize to the thyroid gland, in which the correct diagnosis depended on good cytologic sample from FNAB.
Summary and Conclusions
RCC is the common extra-thyroidal tumor to metastasize to the thyroid gland according to both earlier and more recent literature. It accounts for almost half of patients with this condition. Colorectal, lung, and breast are also relatively common sources of nonthyroid cancers that metastasize to the thyroid. Sarcomas metastasize to the thyroid gland more frequently than previously ascertained. It is not clear if there has been a real change in the behavior of sarcomas with regard to metastasizing to the thyroid or this is due to differences in ascertainment between the older and more recent literature. Females show a slight predilection for metastases to the thyroid from nonthyroidal tumors. Nodular goiter may be a preferential site for nonthyroid metastases compared with normal thyroid tissue but whether this is the case is difficult to confirm.
Clinical exam and imaging studies remain important in the diagnosis of thyroid metastases from nonthyroid tumors. Many patients have symptoms of compression, airway obstruction, hoarseness, dysphagia, and a few have transient thyrotoxicosis. There should be a high index of suspicion for thyroid metastases when a patient with history of NTM presents with a new thyroid finding. FNAB along with IHC is a useful diagnostic tool but may be misleading if nodular goiter is present. Therefore if the FNAB is difficult to interpret, there should be a low threshold for repeating the biopsy and utilizing optimal ultrasound guidance if metastases from a NTM are suspected.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.