
Abstract
Background:
Immunosuppressive therapy with glucocorticoids alone or in combination with radiotherapy is first-choice treatment for the active phase of Graves' ophthalmopathy (GO). Intravenous methylprednisolone (mPRED) pulse therapy is much more effective, safer, and better tolerated than steroids orally administered. There have been some reports, however, of unfavorable reactions to mPRED pulse therapy on liver function. Here, we report laboratory test results in patients with GO before and after intravenous mPRED therapy.
Methods:
Thirty patients (24 women and 6 men) whose mean age was±standard error of the mean 53±1.3 participated in the study. All patients were treated with mPRED for their history of GO. None had received radiotherapy before mPRED. There was no history of liver disease including viral hepatitis in any of the patients. A battery of tests including general serum chemistries and liver function tests as well as those relating to clotting parameters and viral forms of hepatitis were performed a week before and 2 days after mPRED therapy.
Results:
mPRED pulse therapy caused a significant, below reference range, decrease in alkaline phosphatase activity from 119.43±14.98 to 105.53±13.98 IU/L and an increase in gamma-glutamyltranspeptidase activity (above reference range, but not statistically significant) from 23.76±2.93 to 25.3±1.52 IU/L. No significant changes were noted in other liver enzymes activities. We also observed a significant, below reference range, decrease in serum total protein as well as a significant, above reference range, increase of alpha-1 globulins, and low-density lipoproteins cholesterol levels. Pulse therapy also resulted in a significant, but still within reference range, decreases in activated partial thromboplastin time (APTT) from 29.03±0.86 to 26.13±1.16 s, fibrinogen from 3.85±0.2 to 3.05±0.13 g/L, and increase of International Normalized Ratio (INR) from 1.06±1.06 to 1.11±0.06. Despite a lack of a history of viral hepatitis, six patients had positive tests for anti-Hepatitis B e (HBe) antibodies before mPRED administration. In two of these patients, anti-HBe antibody tests became negative after mPRED treatment. In two of the six patients who had positive anti-HBe antibodies, anti-HBc antibodies in the IgG class were also present before and after mPRED treatment. Another patient was found to have anti-HBc IgG both before and after mPRED treatment. Other markers of A and C viral hepatitis were negative in all patients.
Conclusions:
Patients who are on anticoagulents need careful monitoring of their INR, APTT, and fibrinogen while on mPRED therapy. We recommend at least once a week. In patients without evidence for active viral replicating disease, but with past hepatitis B, as judged by the presence of pertinent markers, mPRED pulse therapy for GO does not appear to reactivate hepatitis B.
Introduction
Immunosuppressive treatment with glucocorticoids alone or in combination with radiotherapy is the first choice to treat the active phase of GO. Recurrences of active GO are a problem when glucocorticoids are withdrawn or tapered. Conversely, chronic administration of high doses of glucocorticoids cause a deterioration of the quality of life. There are several regimens of glucocorticoid therapy, ranging from small doses, given orally for weeks or months to high-dose intravenous pulse therapy. Many consider that methylprednisolone (mPRED) pulse therapy is better tolerated, safer, and more effective in achieving earlier and longer remission (5 –17). The Clinical Activity Score (CAS) and the titer of the thyrotropin (TSH)-receptor autoantibodies decline more rapidly after intravenous pulse therapy than after oral glucocorticoid treatment (7,13).
The possibility of hepatotoxicity is of concern when using glucocorticoids, especially in high doses. Marino et al. (18) described a patient with acute hepatitis with lymphocytic infiltration. She was a 43-year-old woman who received a cumulative dose of 4.7 g mPRED for GO during a 12 week period (two infusions every other week for a total of 12 infusions). Salvi et al. (19) also reported a 43-year-old woman who received a cumulative dose of 5.5 g mPRED (7.5 mg/kg per cycle) over a period of 16 weeks (one cycle every 2 weeks, each cycle comprising two infusions on alternate days) for GO. Shortly before her last dose, there was an acute increase in her liver enzymes. Marino et al. (20) studied a group of 800 patients treated with intravenous pulses of mPRED for GO. These patients received doses of mPRED ranging from 7.5 to 15 mg/kg daily from periods of 8 to 16 weeks (cumulative dose range=3.0 to 24 g). In seven patients, severe liver damage occurred, in three of whom this complication was fatal. The total dose of mPRED was slightly higher in patients who died (10.8±3.6 g) than in those who recovered (7.9±2.9). Le Moli et al. (21) compared two groups of patients with GO. One group (n=13) received cumulative doses of 8.45 g mPRED, and the other (n=14) received 4.5 g mPRED. Increases in liver enzymes occurred in about 38% of the higher dose group and in 14% of the lower dose group, but it was only in seven persons in the group receiving the higher dose of mPRED that the hepatic enzyme increased to more than the reference ranges. Similar observations were made by Hiromatsu (22), who compared lower (4.5 to 6 g) with higher (9 to 12 g) cumulative doses of mPRED for GO. More hepatotoxicity was noted in the group receiving the higher doses of mPRED with three fatalities due to liver failure in that group.
Due to unclear mechanism of acute liver damage during mPRED therapy, the aim of the study was to assess changes of selected liver function parameters before and after mPRED therapy, intravenously administered in a cumulative dose of 8 g within 4 weeks in patients with GO. In papers that considered the influence of high doses of mPRED therapy on liver function, a group of patients have not been examined with regard to the presence of viral hepatitis markers before and after glucocorticoid treatment. We wished to look for markers that would identify patients who would be more likely to develop liver disturbances during mPRED treatment, as this information might help define the tests that should be performed before starting high doses of mPRED.
Materials and Methods
The study enrolled 30 patients (24 women and 6 men) of mean age±standard error of the mean 53±1.3. To be included in the study, patients needed to have moderately severe or severe active GO (at least 2 to 6 weeks before mPRED therapy) with a CAS equal to or greater than 4, their tests for anti-TSH receptor antibodies needed to be positive, and they had to be euthyroid as far as clinical parameters and thyroid function tests were concerned for at least 4 months. Thus, the exclusion criteria for the study were nonactive GO, medications with hepatotoxic actions, nonviral liver diseases, renal failure, alcoholism, psychiatric disturbances, advanced osteoporosis, inflammatory diseases, viral, bacterial or fungus diseases, pregnancy, lactation, unstable diabetes mellitus, endogenous hypercortisolism, hypo- or hyperthyroidism, and lack of patient's consent for study enrollment.
Seventeen patients had GO when they first developed Graves' disease and, in 13 patients, GO developed 4 to 8 months after the onset of Graves' disease. None of the patients had received corticosteroids before their mPRED pulse therapy and were not taking any other medications for GO except only local ocular protective agents. None of the patients had received radiotherapy for GO before mPRED pulse therapy. All patients had been euthyroid for at least 4 months having previously been treated for hyperthyroidism with methimazole for 6 to 18 months. One patient had received previous radioiodine therapy for hyperthyroidism, and two had undergone thyroid surgery. These patients had been taking levothyroxine replacement therapy, and twelve patients had been smokers.
Before treatment, the activity of GO was assessed by using the CAS (23) and magnetic resonance imaging (MRI) of eye muscle and retro-orbital tissues. The severity of GO was classified according to a modified NOSPECS* classification (24). All patients in the study had a NOSPECS classification of class III or greater. A clinical examination with exophthalmometry and monocular fixation field measuring by Goldmann perimetry were carried out before and after steroid pulse therapy, MRI was performed only before the treatment. When taking the patient history, there was special focus on a history of viral hepatitis, vaccinations for hepatitis, use of hepatotoxic drugs, and past exposure to hepatotoxic substances. Abdominal ultrasonography was performed in all patients before and after mPRED therapy to assess liver structure.
Before and directly after mPRED pulse therapy, a number of parameters were assessed. These included total protein and serum protein electrophoresis, C-Reactive Protein (CRP), serum immunoglobulins (IgG, IgM, and IgA), coagulation tests (activated partial thromboplastin time, International Normalized Ratio [INR], protrombin time, protrombin, and fibrinogen), serum enzyme activities (glutamic pyruvic transaminase, glutamic oxyloacetic transaminase [SGOT], alkaline phosphatase [ALP], gamma glutamyltranspeptidase [GGTP], lactate dehydrogenase), direct and indirect bilirubin, iron and transferrin, lipid profile (high-density lipoproteins [HDL], low-density lipoproteins [LDL], and triglycerides), neoplastic markers (alpha-fetoprotein, carcinoembryonical antigen [CEA], carbohydrate antigen 19-9 [Ca 19-9]), and viral hepatitis parameters (Hepatitis B [HBs] surface antigen, Hepatitis B surface antibody [anti-HBs], Hepatitis B e antigen [HBe], Hepatitis B e antibody [anti-HBe], core antibody IgG class [anti-HBc IgG or total IgG], core antibody IgM class [anti-HBc IgM], Hepatitis C antibody [anti-HCV], and Hepatitis A antibody [anti-HAV]). Tests for viral markers were performed by using immunoenzymatic method.
All patients enrolled in this study gave their informed consent. The study was approved by the Ethics Committee of the Silesian Medical University.
To test data for normal distribution, the Shapiro-Wilk test was used. Statistical analysis for data that were normally distributed was performed by using paired Student's t-test. Wilcoxon signed-rank test was used otherwise. p-value ≤0.05 was considered significant. Unless otherwise indicated, data were expressed as mean±SEM.
Results
Effect of mPRED therapy on GO
All patients experienced improvement in clinical soft tissue swelling after mPRED therapy. The CAS was significantly reduced from 5.06±0.19 before treatment to 2.67±0.17 after the treatment (p<0.01). Limitation of eye movement was improved in 12 patients (40%). No change was observed in the degree of proptosis.
Effect of mPRED therapy on circulating biochemical parameters
mPRED pulse therapy was associated with a significant decrease of total serum protein and ALP to below the reference range as well as a significant increase of alpha-1 globulins and LDL cholesterol concentrations to above the reference range. There was also a significant decrease in a number of tests, though not to below the reference range. These included serum gamma globulins, CRP, immunoglobulins IgA and IgG, fibrinogen, direct bilirubin, and triglycerides. Beta globulins, INR, total cholesterol, HDL cholesterol, iron, CEA, and Ca 19-9 markers increased but not to above the reference range. Mean serum GGTP activity increased to above the reference range, but this increase was not significant. Tests for antinuclear antibodies (ANA) and antimitochondrial antibodies (AMA) were negative before and after mPRED treatment (Figs. 1 and 2, Tables 1 and 2).
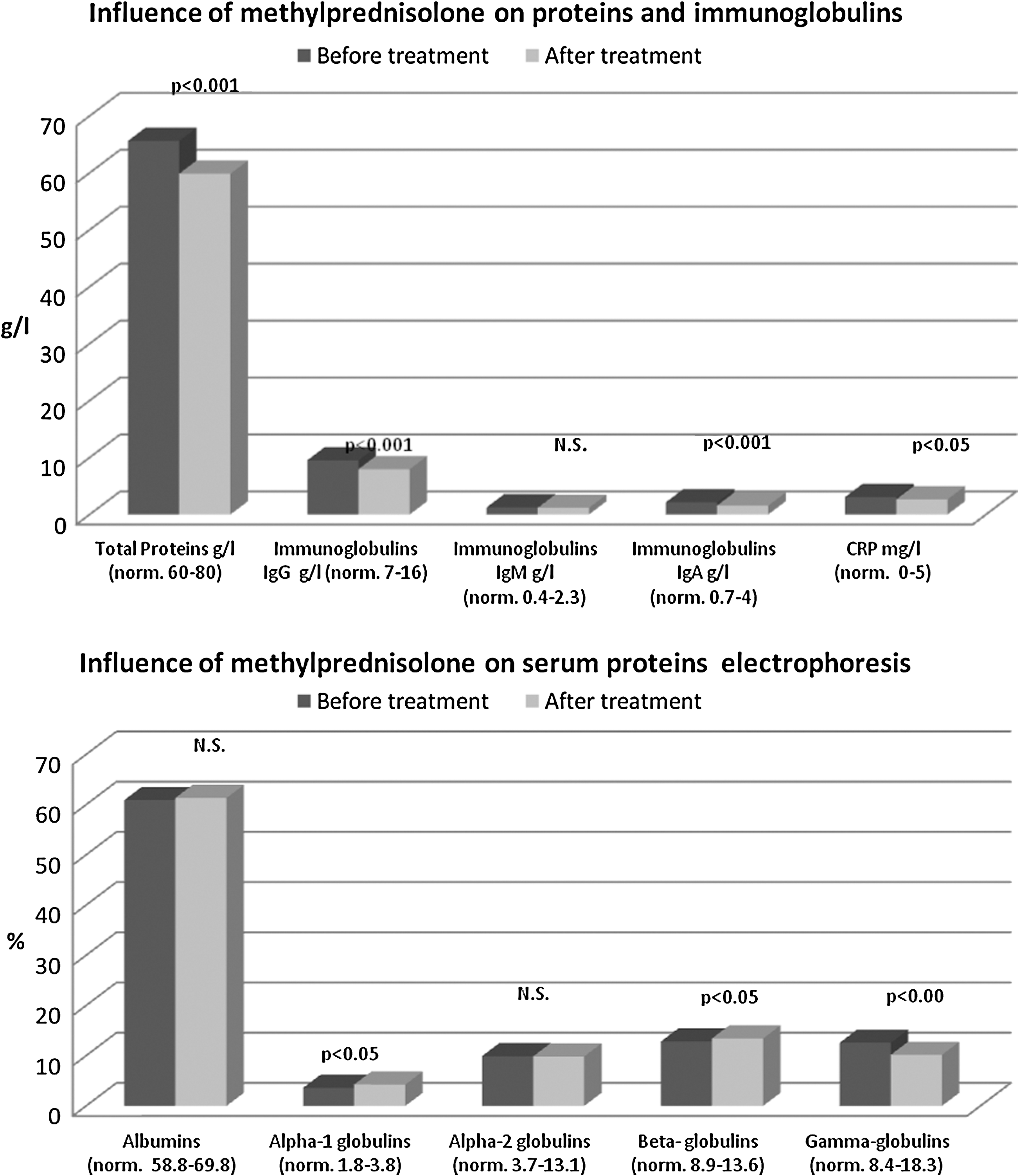
Influence of methylprednisolone on proteins, immunoglobulins, and serum proteins electrophoresis.
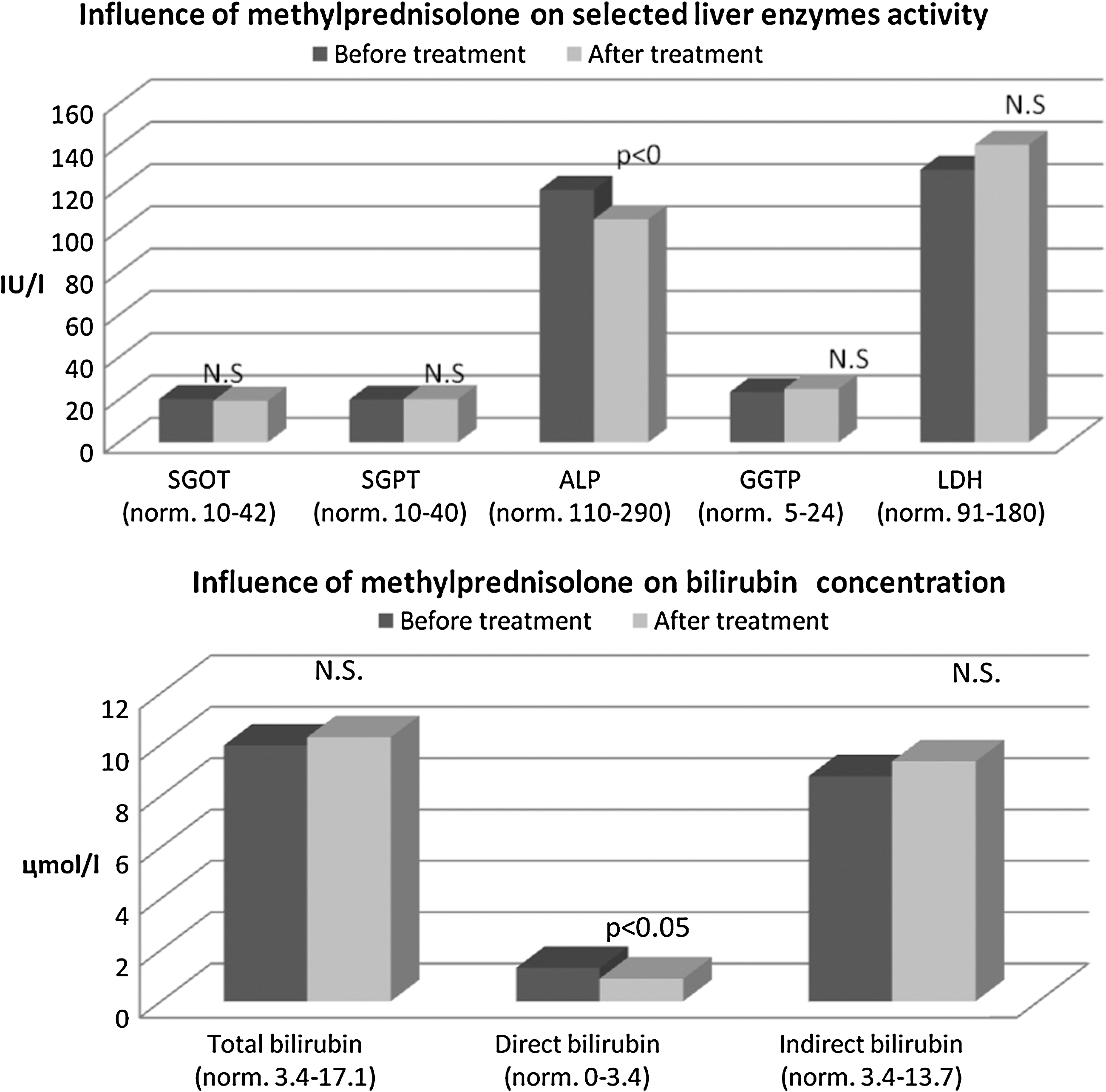
Influence of methylprednisolone on selected liver enzymes activity and bilirubin concentration.
APTT, activated partial thromboplastin time; INR, International Normalized Ratio; PT, protrombin time; N.S., non significant.
HDL, high-density lipoproteins; LDL, low-density lipoproteins; AFP, alpha-fetoprotein; CEA, carcinoembryonical antigen; Ca 19-9, carbohydrate antigen 19-9.
mPRED treatment and viral hepatitis markers
Although none of the 30 patients in the study had a history of viral hepatitis, 8 had been vaccinated against viral hepatitis type B (Table 3). Tests for anti-HBs were negative in patients who had not been vaccinated against hepatitis type B and ranged from 20 to >1000 mIU/mL in patients who had been vaccinated against hepatitis type B. Six patients tested positive for Anti-HBe antibodies before mPRED treatment. In two of these patients, this test became negative after mPRED treatment. In two of the six patients who tested positive for anti-HBe antibodies, the tests for anti-HBc in the IgG class was positive both before and after mPRED treatment. In one patient who tested negative for anti-HBe antibodies both before and after mPRED treatment, there was a positive test for anti-HBc IgG both before and after mPRED treatment. Other markers of A and C viral hepatitis were negative in all patients. Tests for ANA and AMA were negative both before and after mPRED treatment.
HB, Hepatitis B; HCV, Hepatitis C antibody; HAV, Hepatitis A antibody.
Discussion
Although many side effects of glucocorticoid therapy are well known, there have been a few studies of liver function parameters with high-dose mPRED pulse therapy. Severe hepatotoxic effects of glucocorticoids are rare, but may be irreversible and lead to death. Marino et al. reported on a group of 800 patients with GO who had been treated with high doses of mPRED and noted severe liver lesions in seven patients (0.9%). Three of these patients died of fulminate liver failure (20).
When hepatic dysfunction has developed with glucocorticoid treatment, a mixed hepatocellular-cholestatic histopathology is generally observed. Before using pharmacological doses of glucocorticoids, patients should have determinations of serum SGTP, SGOT, ALP, and GGTP activity; and, if these are increased, then glucocorticoids are for the most part contraindicated. If other tests, such as bilirubin, serum proteins, neoplastic markers, or lipids, are abnormal, then it is important to determine whether this is due to intrinsic hepatic dysfunction or extra-hepatic causes, as the former would also be a contraindication to glucocorticoids.
There are likely several mechanisms of liver damage during glucocorticoid therapy. These include a direct toxic effect of glucocorticoid on hepatocytes, which is probably dose dependent, and hypersensitivity-mediated reaction (25 –28). The possibility of the latter reaction is an important reason for obtaining liver function tests before glucocorticoid treatment and closed monitoring of these tests during treatment. Other possibilities are activation of an autoimmune process (18,19) and finally perhaps, activation of latent viral infection (29,30).
Autoimmune liver diseases are rare. There are two main autoimmune liver pathologies: autoimmune hepatitis and primary biliary cirrhosis (31 –34). Marino et al. (18), Salvi et al. (19) described isolated cases of fulminant liver failure after mPRED therapy as a result of reactivation of an autoimmune process. Considerations relating to this problem are complicated. In the case report by Marino et al. (18), liver failure was apparently provoked by a high dose of glucocorticoids; however, on the other hand, small oral doses of the same glucocorticoid helped to improve the patient's liver function. The data in our study are probably not pertinent to this problem, because none of our patients had ANA or AMA.
Regarding the possibility of reactivation of a latent viral infection, the report of Mensing (29) is pertinent. This report described fulminate liver failure after mPRED pulse therapy in a latent HBs-antigen carrier. In Poland, there are about 300,000 HBs-antigen carriers and ∼600,000 HCV carriers, respectively. Based on this report, it would seem important to determine whether patients who are candidates for mPRED treatment should be tested for latent viral infection. The most commonly used viral markers are HBs antigen, anti-HBs antibodies, anti-HBe antibodies, total and IgM anti-HBc antibodies, anti-HCV antibodies, anti-HAV IgG, and IgM antibodies. Regarding viral hepatitis type B, there are many possible antigen constellations together with the presence or absence of various types of antibodies. Due to wide use of vaccinations against hepatitis type B, the presence of anti-HBs antibodies may mean either immunization after the vaccination or presence of infection in the past; so, in cases where there is a high level of such antibodies, the patient history is crucial. New infection is always connected with the presence of IgM anti-HBc antibodies and is an evident contraindication to glucocorticoid therapy.
The results of the current study may act as a guide when considering this problem. In 7 of our 30 patients, there were tests that might have indicated a history of hepatitis B infection in the past. None of these patients were HBs or HBe positive. Six patients tested positive for anti-HBe; in two of them, there was also a positive test for anti-HBc IgG. In another patient, there was a positive test for anti-HBc IgG. Therefore, there were seven patients who probably had hepatitis B infection in the past, even though none of them recalled this history and hepatic ultrasound scans did not suggest liver pathology. Importantly, tests for anti-HBc IgM were negative in these seven patients, thus suggesting that there was no new, active infection/viral replication would have been a contraindication to mPRED therapy. The notable finding of the current study is that relatively high doses of mPRED for GO were not associated with reactivation of hepatitis B. In fact, in two patients with positive tests for anti-HBe antibodies, these tests become negative after mPRED treatment. We conclude that the risk of reactivating hepatitis B in patients without active infection is low with intravenous mPRED pulse therapy. Data regarding other viruses that cause hepatitis would be of interest.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.
*
In 1969, the American Thyroid Association adopted the formal classification of Ocular Graves' disease, represented by the mnemonic NOSPECS. The disease process passes through 6 stages: (0) No signs or symptoms present; (I) Only symptoms of ocular irritation (dryness, tearing, foreign body sensation); (II) Soft tissue involvement (periorbital edema); (III) Proptosis; (IV) Extraocular muscle involvement (ophthalmoplegia); (V) Corneal involvement (dense punctate epitheliopathy, infilitration, and ulceration); (VI) Sight loss with or without visual field compromise secondary to compressive optic neuropathy. However, because the disease is recognized as variable, the formal classification was revised in 1974 to range from no manifestations to mild, moderate, or severe manifestations.