
Abstract
Background:
The management of patients with severe thyrotoxicosis in the absence of a functional gastrointestinal tract represents an uncommon but significant clinical challenge associated with a high mortality rate. This article offers a literature review and discussion of the available management options in this setting.
Summary:
Treatment of severe thyrotoxicosis in patients unable to ingest medications by the oral route should focus on normalization of thyroid hormone levels utilizing conventional medical therapy for thyrotoxicosis, administered via non-oral routes. This includes thionamides, beta-blockers, iodine containing solutions, and glucocorticoids. When conventional medical therapy fails, plasmapheresis should be considered as a temporary therapeutic bridge until conventional therapies can be instituted effectively or emergent surgery performed.
Conclusion:
Although a rare scenario, the management of patients with severe thyrotoxicosis in the absence of a functional gastrointestinal tract represents a challenging clinical situation. Endocrinologists and critical care physicians should be apprised of the available treatment modalities which must be instituted swiftly in order to avoid a catastrophic outcome.
The Clinical Problem
Gastrointestinal manifestations of severe thyrotoxicosis are well recognized but have not been emphasized in medical textbooks. Harper et al. conducted a retrospective chart review of 25 patients hospitalized for thyrotoxicosis and found that abdominal symptoms were included as a chief complaint in 36% of cases; 44% vomiting, 28% nausea, and 20% abdominal pain (7). Vomiting as a chief presenting complaint of thyrotoxicosis has been well documented (8 –12). The mechanism via which hyperthyroidism causes vomiting, however, is unclear; both a direct effect of thyroid hormone on gastrointestinal motility (9) and thyroid hormone stimulation of a chemoreceptor trigger zone in the central nervous system (8) have been proposed. Increased adrenergic activity could also explain thyrotoxic vomiting, and therapy with B-blockers leads to rapid resolution of vomiting in some thyrotoxic patients (10 –12). Mild to moderate diarrhea is seen in up to 25% of patients with hyperthyroidism (13) and is likely due to increased intestinal motility and reduced small bowel transit time (14). Adrenergic hyperactivity is implicated, because B-blockade leads to correction of transit time and resolution of diarrhea in some thyrotoxic patients (15). In addition, diarrhea may be related to a hypersecretory state within the intestinal mucosa (16).
Management Strategies
Treatment of severe thyrotoxicosis in patients unable to take oral medications should focus on normalization of thyroid hormone levels utilizing conventional medical therapy, administered via nonoral routes as outlined in Table 1. Medical therapy consists of decreasing the synthesis, release, and peripheral effects of thyroid hormone and includes the use of thionamides, iodide, β-blockers, and corticosteroids (17). When conventional medical therapy fails, plasmapheresis (PP) and/or surgery should be considered (17). A suggested treatment algorithm is outlined in Figure 1.
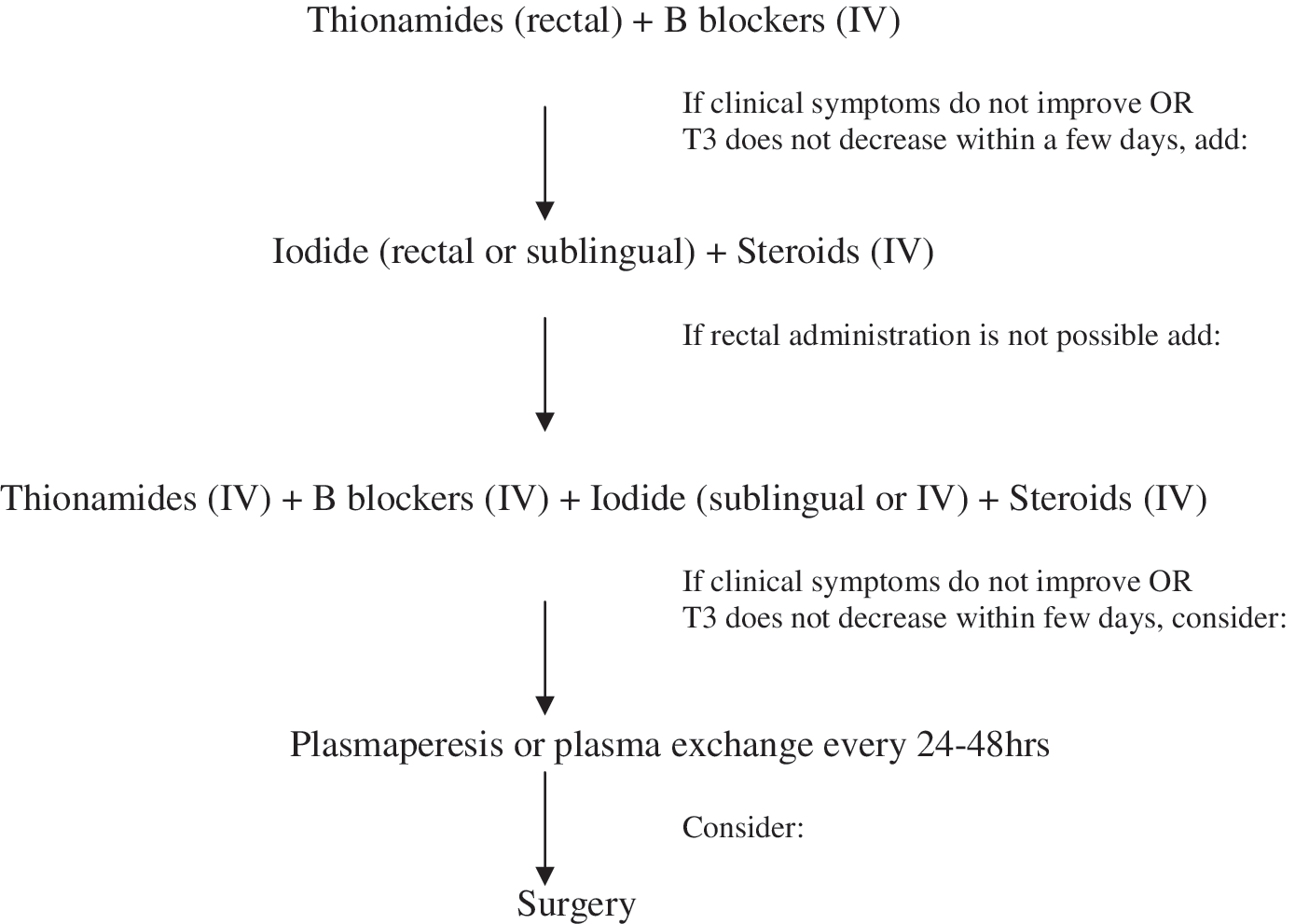
Treatment algorithm for severe thyrotoxicosis in patients unable to take per oral.
Mode of administration is not routinely available and should be prepared from the oral form.
Loading dose of 250–500 μg/kg can be given before the infusion.
SSKI, saturated solution of 5% potassium iodide.
Medical therapy via a nonoral route
Thionamides
Thionamides represent the mainstay of medical treatment of thyrotoxicosis. These drugs begin to inhibit thyroid hormone synthesis within 1–2 hours of oral administration. Alternative routes for thionamide administration include rectal, parenteral, and, in animals, transdermal administration.
Rectal administration of thionamides has been demonstrated to represent an effective treatment option for patients who cannot take oral therapy (1 –5,18). Rectal formulations of antithyroid drugs include enemas or suppositories (1 –5,17 –20). Nabil and colleagues used a suppository formulation of methimazole (MMI) (18). The authors dissolved 1200 mg of MMI in 12 mL of water with two drops of span 80 (sorbitan oleate; sorbitan(z)-mono-9-octadecenoate) mixed with 52 mL of cocoa butter (18). Zweig et al. similarly formulated a suppository of propylthiouracil (PTU) and treated subjects successfully with 400 mg of PTU every 6 hours (2). Yeung and colleagues used an enema preparation of PTU and administered 600 mg by Foley catheter inserted into the rectum (5). Retention was achieved by clamping the catheter and inflating the balloon. Walter et al. similarly used an enema formulation containing 400 mg of PTU and administered it successfully every 6 hours (1). Jongjaroenprasert and colleagues compared the use of a PTU enema preparation with a suppository preparation (19). The authors concluded that enema preparations provided greater bioavailability than the suppositories, but both preparations had a comparable therapeutic effect. Rectal suppository formulations may be more comfortable for the patient and are less labor-intensive for the nursing staff compared to retention enemas (2).
A few authors have examined serum thionamide levels after rectal versus oral administration. Nabil et al. (18) compared MMI rectal suppositories with oral administration of the drug in six normal subjects and found no difference in serum MMI levels between the two routes. Bartel et al. (20), however, found that serum PTU levels were lower when administered via suppositories compared with oral administration, although rectal administration did show clinical efficacy.
Parenteral administration of thionamides
Literature describing the use of parenteral thionamides for the treatment of thyrotoxicosis is limited. There are, however, a few reports demonstrating the efficacy of intravenous (IV) thionamides in patients with thyroid crisis and gastrointestinal tract dysfunction in whom oral and rectal thionamide administration was prohibited (21 –25). Parenteral MMI is commercially available in a few European countries such as Germany, the United Kingdom, and Poland (22,25,26) but not in the United States (24). IV thionamides, however, can be prepared by sterile pharmacies. The relative insolubility of PTU at a physiologic pH makes its use as an IV agent difficult and has consequently limited its use in this form. In one report, however, IV PTU, prepared by dissolving tablets in isotonic saline with an alkaline pH (pH 9.25) and administered at a dose of 576 mg/day (50 mg/mL), was efficacious (23). Hodak and colleagues prepared IV MMI by reconstituting 500 mg of MMI powder with 0.9% sodium chloride solution to a final volume of 50 mL and administered it as a slow IV push over 2 minutes. With this method, the authors successfully treated two thyrotoxic patients intolerant of oral and rectal thionamides for 7 and 9 days (24). Parenteral MMI has been used at doses up to 180 mg/day for as long as 14 continuous days (21,22,24,25).
Transdermal MMI has been used effectively for the treatment of hyperthyroidism in animals. In one study, 13 newly diagnosed cats with hyperthyroidism were treated with a transdermal formulation of MMI. Clinical improvement as well as a significant decrease in thyroxine (T4) was noted in all cats. Only one cat showed a cutaneous adverse reaction along with a marked thrombocytopenia (27). Transdermal MMI has not been used to treat hyperthyroidism in humans. However, topical MMI is used as a therapy for skin hyperpigmentation in humans. In one case report, topical MMI (5%) applied once daily for 6 weeks was used to successfully treat a patient with hyperpigmented lesions on his face, without affecting the serum level of thyroid hormones (28). The effect of topical applications of 100 mg of 5% MMI (equivalent to 5 mg MMI oral formulation) on thyroid function was assessed in 15 patients with epidermal melasma (29). No significant changes in serum thyroid-stimulating hormone (TSH), free thyroxine (FT4), or free triiodothyronine were detected after 6 weeks of therapy. Pharmacokinetics of a topical formulation of MMI (5%) applied once to facial skin was compared with a 5 mg oral dose of MMI in six volunteers. MMI was measured beginning at 15 minutes and for up to 24 hours after oral administration. MMI was not detected in the serum after topical application over this 24-hour period. It is possible that the application of higher doses of topical MMI and/or application for longer duration are necessary to achieve significant serum levels and a therapeutic effect similar to that noted in animals.
Beta-blockers and antiadrenergic agents
Beta-blockade represents an important therapeutic intervention in the treatment of thyrotoxicosis. Fortunately, there are many IV beta-blocker preparations that can be used in patients with severe hyperthyroidism with compromised oral intake. However, these drugs should be used with caution in the setting of hypotension, bronchial asthma, or congestive heart failure. Nevertheless, control of tachycardia may result in an improvement of cardiac function in the latter condition. Propranolol can be given intravenously, 1 mg/min until several milligrams have been administered or adequate beta-blockade has been achieved (30). An alternative regimen is esmolol, utilizing a loading dose of 250–500 μg/kg, followed by an infusion at 50–100 μg/kg per minute (31). IV infusion of landiolol, an ultrashort-acting β1 blocker, successfully controlled tachycardia during the perioperative and postoperative periods in two patients with uncontrolled hyperthyroidism until they could be transitioned to long-acting oral beta-blockers and antithyroid drugs (32).
When beta-blockers are contraindicated, the antiadrenergic agent reserpine (2.5–5 mg every 4 hours) can be administered intramuscularly to counteract the peripheral effects of thyroid hormone. However, reserpine should be used only when beta-blockers are contraindicated and in the absence of hypotension or central nervous system depression (33).
Iodine-containing solutions
Iodine-containing solutions are known to block the release of T4 and triiodothyronine from the thyroid gland (17). The administration of iodide, however, should be delayed for at least 1 hour after thionamide administration to prevent the iodide from being used as a substrate for new hormone synthesis (17). In patients with severe hyperthyroidism who cannot take medications orally, alternative routes of iodine administration can be used. IV sodium iodide can be used at a dose of 0.5–1.0 g every 12 hours (21). However, IV iodide, including sodium iodide, is no longer available in most countries including the United States (17). It has been suggested that 10 drops of Lugol's solution can be directly added to IV fluids because it is sterile (34). Rectal administration of inorganic iodide is also an effective, readily available, and less-expensive alternative to parenteral iodides (3 –5). Alternatively, the iodide solution can be administered sublingually. In one case report, 0.4 mL of a saturated solution of 5% potassium iodide given sublingually three times daily along with rectal PTU proved to be an effective therapeutic combination in a patient with thyroid storm and duodenal obstruction (4). Measurement of urinary free iodine indicated that 70% of the sublingually administered iodide was absorbed (4).
Glucocorticoids
The use of glucocorticoids in patients with severe hyperthyroidism or thyroid storm has been shown to improve outcome (35). Glucocorticoids reduce T4-to-triodothyroinine conversion in the periphery and may have a therapeutic effect on the underlying autoimmune/inflammatory process in Graves' disease (17,36). Treatment with glucocorticoids is recommended for patients with severe thyrotoxicosis, particularly when manifesting hypotension, because of the possibility of concomitant undiagnosed adrenal insufficiency or relative insufficiency due to accelerated production and degradation owing to the hypermetabolic state (17,35,36). Further, these agents are readily available in IV form and are available to be used in such challenging clinical situations where enteral therapy is not possible. The recommended dosing of glucocorticoids in such patients is summarized in Table 1 (17).
Alternative therapeutic interventions
When standard therapies such as those suggested above cannot be administered or are unsuccessful, plasmapheresis (PP) and/or emergent surgery deserve consideration.
PP and therapeutic plasma exchange (TPE) are effective alternative therapies for the treatment of thyrotoxicosis and thyroid storm. Both procedures can effectively reduce circulating thyroid hormone levels within 3 days (37 –39). Thyroid hormones are bound to plasma proteins. In both PP and TPE, the patient's plasma is separated and removed from other blood components. In TPE, the patient's plasma is replaced with a solution such as colloid (e.g., albumin and/or plasma) or a combination of crystalloid/colloid solution, whereas in PP, the removed plasma is not replaced (40). Plasma or human albumin solutions that are given during TPE provide new binding sites for circulating free hormones and may limit the bioavailability of free thyroid hormones (39). In addition, removal of circulating TSH receptor stimulating antibodies could be another possible mechanism leading to improvement in thyrotoxicosis (41). It was noted that the clinical improvement of thyrotoxicosis is more significant than the improvement of thyroid hormone levels after PP/TPE (37,39). The effect of PP/TPE on thyrotoxicosis is transient, lasting approximately 24–48 hours. Definitive therapy such as surgery is necessary once the patient's clinical condition improves (42,43). PP or TPE can therefore be used as a preoperative intervention to rapidly normalize thyroid hormone levels and lower operative risks of thyroid and nonthyroid surgery (37 –39). PP/TPE has also been used to successfully treat thyroid storm in the postoperative period after thyroidal as well as nonthyroidal surgical procedures (44,45). PP/TPE should be considered when other treatment options outlined above are either ineffective or contraindicated. Complications of PP/TPE include hypotension, hemolysis, anaphylactic or allergic reactions, coagulopathy, vascular injury, and infection (46).
Surgery
Emergent thyroidectomy is hazardous in the setting of severe thyrotoxicosis or thyrotoxic crisis and is associated with a high procedural risk (47). It is a standard clinical practice to postpone elective surgical procedures until normalization of thyroid function tests (TFTs). However, there are a few reports of successful thyroidectomy in patients with severe thyrotoxicosis when all medical therapeutic interventions have failed (48 –50). Additionally, there are a few reports of successful nonthyroidal emergency surgery in the setting of thyrotoxic crisis (32,39,51). One should consider surgical intervention in severe life-threatening thyrotoxicosis as a last option when all standard therapies have failed. PP, as mentioned earlier, can be instituted preoperatively to improve thyroid function and decrease the surgical risk (37 –39).
Illustrative Case
A 34-year-old man known to have Graves' disease for many years and treated with MMI 20 mg daily, but poorly compliant with treatment and follow-up, presented with sudden onset of epigastric abdominal pain. On presentation, he was hemodynamically unstable, and his temperature was 38.6°C, blood pressure 88/50 mm Hg, and pulse rate 120 per minute and regular. Notable findings on exam included bilateral exophthalmos and a diffuse large goiter approximately 60 g in weight. The abdomen was tender to palpation with rebound tenderness and significant guarding. Bowel sounds were absent. TFTs were TSH <0.16 μU/mL (reference value: 0.2–4.5 μU/mL), FT4 30.5 pmol/L (reference value: 12–22 pmol/L), and triiodothyronine 12.49 pmol/L (reference value: 2.8–6.8 pmol/L). An upright abdominal Roentgenogram revealed free air under the diaphragm. The patient was admitted to the intensive care unit (ICU), administered nothing per os, and supported hemodynamically with vasopressors and antibiotics. PTU 400 mg every 6 hours was administered rectally by retention enema. On the day of admission, after stabilization of the patient's medical condition, he was taken to the operating room for an emergent laparotomy. A perforated duodenal ulcer was found and repaired. Despite aggressive medical therapy that included rectal PTU, vasopressors, IV fluids, and antibiotics, on postoperative day 2, the patient's condition deteriorated, pulse rate increased to 150 per minute, blood pressure dropped to 85/48 mm Hg, and TFTs worsened (FT4 increased to 60, and TSH <0.001 μU/mL). PTU was increased to 600 mg every 6 hours, and hydrocortisone 100 mg IV every 8 hours was initiated. Beta-blockers were contraindicated because of profound hypotension. Clinical improvement was noted. Five days postoperatively, the patient developed severe diarrhea due to Clostridium difficile and was unable to retain PTU. Antibiotic therapy with IV metronidazole was instituted. FT4 remained high and IV thionamide was requested but not prepared by the hospital pharmacy. Iodine therapy followed by emergency thyroidectomy was considered but not implemented in anticipation of resolution of the diarrhea with antibiotic therapy. Five days after the development of diarrhea, the patient suffered a cardiac arrest and expired during resuscitation.
It is clear that there were many additional therapeutic options, as discussed above, which were unfortunately not implemented in this case. Although the case illustrates a very challenging clinical scenario, the swift implementation of additional measures such as iodine therapy (rectal or sublingual), IV thionamide therapy, PP/TPE, or emergency thyroidectomy as outlined in this review may have afforded the opportunity for a better outcome.
Conclusion
Although a rare scenario, the management of patients with severe thyrotoxicosis in the absence of a functional gastrointestinal tract represents a challenging clinical situation. Treatment is based on conventional medical therapy administered via a nonenteral route. When available, PP/TPE should be considered as a temporary therapeutic bridge until conventional therapies can be instituted effectively or surgery can be performed.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.