
Abstract
Background:
For some endocrine and nutritional biomarkers, for example, cortisol and vitamin B12, significant associations between 24-hour renal analyte excretion and the respective 24-hour urine volume (U-Vol) have been reported. Therefore, our objective was to investigate whether 24-hour U-Vol (a marker of fluid intake) is also a relevant influencing factor of absolute daily iodine excretion.
Methods:
Urinary iodine excretion rates were measured in repeatedly collected 24-hour urine samples of (i) 9 healthy women participating in a controlled diet experiment with constant iodine intake and (ii) 204 healthy free-living adolescents (aged 13–18 years) who performed the respective urine collection during 2003–2008. Associations between U-Vol (L) and renal iodine excretion (μg/24 h) were investigated cross sectionally (multiple linear regression model, PROC GLM) and longitudinally (repeated-measures regression models, PROC MIXED). The major iodine sources in the adolescent's diet (iodized salt, milk, fish, eggs, and meat) were controlled for.
Results:
Urinary iodine excretion was significantly associated with 24-hour U-Vol in all performed fully adjusted regression models. A 1-L increase of U-Vol predicted an additional 15.0 μg/day (adolescents, 95% confidence interval: [9.8, 20.0], p < 0.0001) and 16.5 μg/day (women, 95% confidence interval: [9.2, 23.7], p = 0.0002) increase in iodine excretion. The longitudinal analysis in adolescents revealed a stronger relation of iodine excretion with U-Vol in girls than in boys (β = 17.1 vs. β = 10.5).
Conclusion:
A high fluid consumption, and thus a high U-Vol, could lead to an additional renal iodine loss that obviously cannot be compensated by the iodine contents of non-milk-based beverages, reported to amount to ∼4 μg/L, on average. For specific research questions using the biomarker 24-hour urinary iodine excretion, U-Vol should therefore be considered as a potential confounder.
Introduction
For assessing the nutritional iodine status of a population, urinary iodine excretion is applied as a biomarker, because >90% of iodine intake appears in excreted urine (3 –6). Urinary iodine measurements are performed either in spot urine samples (iodine concentration; μg/L), or in 24-hour urine samples (iodine excretion; μg/24-h), whereby the latter is generally regarded as reference standard for estimating individual iodine intake (7). One main limitation of analyzing spot urine samples, which are preferentially collected in larger population-based studies, is the inevitable dependency on urine volume (U-Vol) level and the corresponding dilution effect (7 –9). In contrast, when 24-hour urine samples are taken to determine iodine status, U-Vol level has hitherto been considered to be irrelevant. However, there are some nutritional and endocrine biomarkers, for example, vitamin B12, cortisol, and cortisone, for which it is well known that a high fluid intake and a corresponding high U-Vol promotes their absolute excretion (10 –12).
To our knowledge, until now, no study has investigated, in how far a corresponding association may also exist for the biomarker renal iodine excretion. Therefore, we aimed to examine the impact of U-Vol (an index of fluid intake) on the urinary excretion of iodine in 24-hour urine samples in a controlled diet experiment and in a longitudinal sample of healthy free-living adolescents. By exactly keeping the iodine intake constant in the diet experiment and by considering the dietary intakes of the main iodine providers in the adolescent's diet, we were able to exclude any relevant dietary causes of variability of urinary iodine output, and could thus examine the independent effect of U-Vol on iodine excretion.
Materials and Methods
Subjects, diet, and urine collections are reported separately for study 1 and study 2. The remainder of this section refers to both studies.
Study 1: subjects, diet, and urine collections
Nine healthy women (24–59 years) participated in the experimental diet study. Over a 5-day period (while maintaining their usual life-style), all women ingested a constant lacto-vegetarian whole-food diet with all foods weighed and prepared in the institute's own kitchen, to ensure an identical nutrient intake during the whole period. All subjects received the same basal energy intake; in case of individually higher or lower energy requirements [calculated on the basis of the individual basal metabolic rate (13) and physical activity level], basal energy intake was adapted by varying amounts of butter or olive oil included in regular lunch. To exclude any variations in iodine intake, because of varying preferences for salt intake, dinner and lunch were prepared salt-free and each subject received an exactly weighed amount of 2 g iodized salt per day (iodine content, 20 μg/g) for flavoring that had to be completely utilized. Fluid intake (allowed were tap water, coffee, and tea) was not restricted, but subjects were advised to maintain a relatively constant fluid intake over the 5-day period.
Twenty-four-hour urine collections (each started immediately after lunch) were performed on days 3, 4, and 5. The volume of each 24-hour collection was carefully recorded.
Study 2: subjects, dietary records, and urine collections
The second investigation was conducted in a study sample selected from the Dortmund Nutritional and Anthropometric Longitudinally Designed (DONALD) Study, an ongoing longitudinal (open cohort) study gathering information about diet, development, and metabolism between infancy and adulthood in healthy subjects (6,14). The DONALD Study is exclusively observational, noninvasive (until the age of 18), and approved by the Ethics Committee of the University of Bonn (Germany). All examinations are performed with parental, and later on with the children's written consent.
The selection of the study population was carried out on the basis of beforehand clearly defined inclusion and exclusion criteria: adolescents at the age of 13–18 years who had completely collected ≥one 24-hour urines along with corresponding dietary records during 2003–2008 were included. One exclusion criterion for an incompletely collected urine sample was a body weight-related 24-hour-creatinine excretion rate <0.1 mmol/(kg · day) (14). Plausibility of dietary records was estimated by calculating the ratio of reported total energy intake to predicted individual basal metabolic rate [estimated by the method of Schofield (13)]. Dietary records with a ratio below the age- and sex-specific cut-off values (15) were excluded. Two hundred fifteen adolescents met the criteria, providing 514 urine samples and corresponding dietary records. From those, 32 urine samples (and corresponding dietary records) had to be excluded because of no or irregular use of iodized table salt, iodine containing drug use, or intake of iodine containing supplements by the adolescents during the time of the respective urine collection. Another two urine samples and the corresponding dietary records were excluded due to unrealistic high values of U-Vol (>4.5 L/day) or iodine excretion (>650 μg/day). Therefore, 204 adolescents with 480 collected 24-hour urines and related dietary records remained for the present investigations.
To estimate the individual food and nutrient intake, 3-day weighed dietary records were used. On three consecutive days the weight of all consumed foods and beverages was recorded using a digital food scale to the nearest 1 g. Out-of-home consumed food was estimated by semi-quantitative recording (e.g., numbers of glasses and cups). Energy and nutrient intakes, including food fortification and nutritional supplements, were calculated as individual means of the three recorded days by using our nutrient database LEBTAB (16). As salt intake could not be quantitatively recorded in the dietary records, it was estimated from urinary sodium measurements.
The urine collection of the DONALD participants was generally carried out on the third day of the 3-day weighed dietary records. The procedures for the 24-hour urine collections have been described in detail previously (6).
Anthropometric measurements
These were conducted on the first day of the diet study and at time of dietary recording in the DONALD Study, respectively. Standing height was measured with a stadiometer (Harpenden, Coymych, United Kingdom) to the nearest 0.1 cm, and weight was measured on an electronic scale (Seca 753E; Seca Weighing and Measuring System, Hamburg, Germany) to the nearest 0.1 kg. From these measurements, body mass index (BMI) and body surface area (BSA) (only in adults) were calculated, the latter according to the formula of Du Bois and Du Bois (17). For adolescents, additionally, sex- and age-independent BMI standard deviation scores (BMI-SDS) were calculated by using the German national reference data (18).
Urinary measurements
In the 24-hour urine samples iodine concentration was determined by a modified Sandell-Kolthoff method after acid wet-washing of the samples (19). Twenty-four-hour sodium excretion was measured by flame atomic absorption spectrometry with a Perkin Elmer 1100 Spectrometer (Perkin Elmer, Überlingen, Germany). For determing completeness of the urine collection, creatinine concentration was quantified in all samples by the Jaffé method with the use of a creatinine analyzer (Beckman-2; Beckman Instruments, Inc., Fullerton, CA).
Statistical analysis
All calculations were performed with SAS procedures (version 9.1.3; SAS Institute, Cary, NC). Significance was defined as p < 0.05.
Descriptive data are given as means ± SD or medians with interquartile ranges when appropriate. Sex differences were tested with an unpaired t-test or Wilcoxon rank sum test, respectively.
To investigate the effect of 24-hour U-Vol on 24-hour renal iodine excretion in the diet experiment, a repeated-measures regression analysis model (PROC MIXED) (adjusted for BSA, creatinine excretion, and the sequential day of urine collection) was used. By including the repeated statement in the statistical routines, the lack of independence between repeated observations on the same person was accounted for. To avoid correlated measurement errors between dependent (iodine excretion) and independent variable (U-Vol) that were both measured in the same urine sample, the regression model was additionally adjusted for creatinine excretion (20).
In study 2 the association between 24-hour U-Vol and 24-hour renal iodine excretion was initially investigated cross sectionally (i.e., only data belonging to the time of first 24-hour urine collection within 2003–2008 were used) by using a multiple linear regression model (PROC GLM). Before the multi-regression analysis, volume-by-sex and volume-by-age interactions were checked, using analysis of covariance. Since no significant interactions were observed, the subsequent cross-sectional analysis was performed nonstratified with the total sample of 204 adolescents. The regression model was a priori adjusted for sex, age, BMI-SDS, and season (as the time points for the collection of urine samples and corresponding dietary records during the year were not fixed). To control for the important iodine providers in the adolescents's diet, sodium excretion, milk, egg, meat, and fish consumption were included as independent variables, and left in the model if p < 0.15. As both the dependent variable (iodine excretion) and some of the independent variables (U-Vol, sodium excretion) were measured in the same urine sample, the regression model was additionally adjusted for creatinine excretion to avoid correlated measurement errors (20). All dietary intake and urinary excretion variables (except creatinine) were corrected for total energy intake by division of individual intakes or excretion rates by individual energy intake.
Second, the association between U-Vol and renal iodine excretion was investigated longitudinally by using a mixed linear regression model (PROC MIXED), including all repeated measurement data of the 204 adolescents, that is, 480 urines as observations. By including the repeated statement in the statistical routines, the lack of independence between repeated observations on the same person was accounted for. In the longitudinal analysis volume-by-sex interactions were observed and therefore the subsequent analysis was conducted sex stratified (for reasons of comparability, longitudinal analysis was also done nonstratified). A priori adjustment variables were sex (total sample), age, BMI-SDS, season, and year of data collection (as trend). All other PROC MIXED model components were identical to the above cross-sectional analysis.
Results
Study 1
All 9 female subjects completed the 5-day diet experiment; therefore, 27 urine samples were available for analysis. Anthropometric, dietary, and urinary characteristics of the study sample are presented in Table 1. The experimental diet provided a total daily iodine content of 109.2 μg/day, 40 μg from iodized salt and the remaining 69.2 μg from the prepared foods [calculated by the German Nutrient Database BLS (21) and actual milk-iodine measurements (22)]. PROC MIXED repeated-measures regression analysis (adjusted for BSA, creatinine excretion, and day of urine collection) of 24-hour U-Vol on urinary iodine excretion revealed a significant positive association: a 1-L increase in U-Vol predicted an average 16.5 μg increase in iodine excretion (95% confidence interval [CI]: [9.22, 23.67], p = 0.0002) (Fig. 1).

Unadjusted association of 24-hour urine volume (U-Vol) (L) with urinary iodine excretion (μg/d) during a 5-day constant and isocaloric diet in women (n = 9) (each point represents individual means of the 3 collected 24-hour urine samples). Repeated measures regression model (PROC MIXED, adjusted for body surface area, creatinine excretion, and day of urine collection) yielded a β-value of 16.45 (95% CI [9.22, 23.67], p = 0.0002) for this association.
All such values are arithmetic means ± SD.
Arithmetic mean of all three urine collections.
BMI, body mass index; SD, standard deviation; U-Vol, urine volume.
Study 2
Characteristics of the DONALD Study sample at the time point of their first 24-hour urine collection within 2003–2008 are presented in Table 2. With regard to the dietary parameters, boys and girls differed significantly in total energy, milk, and meat intakes, but not in the respective energy corrected intakes. The same was true for the urinary parameters (i.e., sex differences between absolute values disappeared after energy correction), except U-Vol. The WHO reference for an adequate iodine status (median urinary iodine concentration >100 μg/L) was only met in males.
All such values are arithmetic means ± SD. Sex differences were analyzed by using unpaired t-test.
All such values are medians (P25; P75). Sex differences were analyzed by using Wilcoxon rank sum test.
Only whey-based milk products.
Meat and meat products.
Only salt water fish products.
Eggs and egg products.
SDS, standard deviation scores; UIC, urinary iodine excretion.
The PROC GLM cross-sectional analysis showed a significant association between 24-hour U-Vol and iodine excretion (β = 14.31, 95% CI: [4.94, 23.67], p = 0.003) (Table 3). Further significant predictors of urinary iodine excretion were milk intake and sodium excretion (as a biomarker for sodium intake) (p < 0.0001). The longitudinal analysis (both the unstratified and sex-stratified analysis), confirmed the cross-sectional results; 24-hour U-Vol was significantly associated with urinary iodine excretion. However, the association was stronger in girls than in boys (β = 17.1, 95% CI: [10.45, 23.75], p < 0.0001 vs. β = 10.5, 95% CI: [1.05, 19.50], p < 0.05) (Table 4). Further significant contributors to iodine excretion (in both girls and boys) were milk intake and sodium excretion (p < 0.0001); fish intake showed significance in the total sample that remained significant in the stratified analysis only for boys.
Results of the cross-sectional multiple linear regression analysis (PROC GLM), adjusted for sex, age, season, BMI-SDS, and creatinine excretion. In the final multivariate analysis model, only those dietary variables remained that yielded p-values <0.15.
CI, confidence interval.
Results of the longitudinal multiple linear regression analyses (PROC MIXED) adjusted for sex (total sample), age, season, time (trend), BMI-SDS, and creatinine excretion. Only those dietary variables remained in the model that yielded p-values <0.15 for the total sample.
Discussion
Our studies, both in adults (diet experiment) and in adolescents (cross-sectional and longitudinal analysis), revealed a clear impact of 24-hour U-Vol level on absolute 24-hour urinary iodine excretion, independently of the respective dietary iodine intake. This effect appears to be more prominent in girls than in boys. A 1-L increase in U-Vol predicted an additional average increase in daily iodine excretion of 16.5 μg and 15.0 μg in adult women and adolescents, respectively. This obvious iodine excretion-stimulating effect of higher U-Vol demonstrates the necessity of considering U-Vol as a confounder in specific epidemiological data analyses on 24-hour urinary iodine output.
A strength of our present analysis was the ability to exclude any known relevant diet-related influences on the variability of renal iodine excretion. In the diet experiment all subjects ingested the same and constant amounts of iodine over the whole period; in the studied adolescents, the detailed knowledge on the consumed amounts of foods enabled us to allow for the main dietary iodine providers in the building of the regression models [according to Remer et al. (6)], and thus to focus on the impact of U-Vol on iodine excretion in particular. The fact that only milk and salt intake appeared as consistently significant dietary contributors to iodine excretion, but not fish, egg, and meat intake, can most likely be explained by the small average amounts of them ingested. However, the good accordance of the calculated values for the effect strength of milk intake on iodine excretion (β = 0.08–0.09; indicating an 80–90 μg increased iodine excretion per 1 L milk intake) with the results of actual laboratory analyses of various cow-milk samples [mean iodine content of German cow milk: 93 μg/L (22)] confirms the accuracy of our 3-day weighed dietary record-based calculations.
Our present analysis demonstrates for the first time that water loading (increased drinking in the physiological range) stimulates iodine excretion. How this U-Vol effect on iodine output may occur can only be speculated, as, to date, the mechanism and regulation of renal iodine excretion is not completely understood. Initially, tubular iodine reabsorption was assumed to mainly occur passively (23 –25). This passive solute reabsorption is directly linked to the rate of water reabsorption (23), because of the permanent strive for a diffusion equilibrium. Therefore, a high rate of tubular water reabsorption (with reduced fluid intake) likewise leads to a higher rate of iodine reabsorption that in turn inevitably leads to a lower renal iodine excretion (along with the reduced U-Vol). During high fluid intake (and corresponding high U-Vol) water reabsorption in the collecting duct is less pronounced, thus resulting in a higher iodine excretion. A similar relationship was already indicated by first experimental data of Bricker and Hlad (25) on the behavior of renal iodine clearance in the presence of osmotic diuresis (suggesting tubular reabsorption of iodide to be a function of a concentration gradient, created by the reabsorption of water from the glomerular filtrate).
By now, besides this passive mechanism of iodine reabsorption, the facilitated diffusion transporter pendrin is also known to be in part responsible for tubular iodine reabsorption (26). Pendrin exerts its main function in the thyroid for the transport of iodide from cytoplasm to follicle lumen, but is also expressed in the kidney, where it occurs mainly in the collecting duct in β-intercalated cells (27). In an animal experiment, Kim et al. demonstrated that pendrin may play an important role for renal iodine reabsorption, especially during high water intake (26). The abundance of pendrin increased with greater water consumption, and therefore increased the driving force for renal iodine reabsorption (26). Thus, when comparing the renal passive with the pendrin-mediated iodine reabsorption mechanism, a higher fluid intake exerts its effects on iodine excretion just the opposite way around, suggesting pendrin to possibly constitute a kind of compensation mechanism for an increased iodine loss during a very high fluid intake. However, our results strongly suggest that the pendrin mechanism cannot fully compensate the passive iodine loss with higher U-Vol. Perhaps the pendrin mechanism allows compensation only up to a certain level of fluid intake. When this level is exceeded, a higher fluid intake may lead to an uncompensated higher iodine output, caused by the above-described reduced passive reabsorption (Fig. 2).
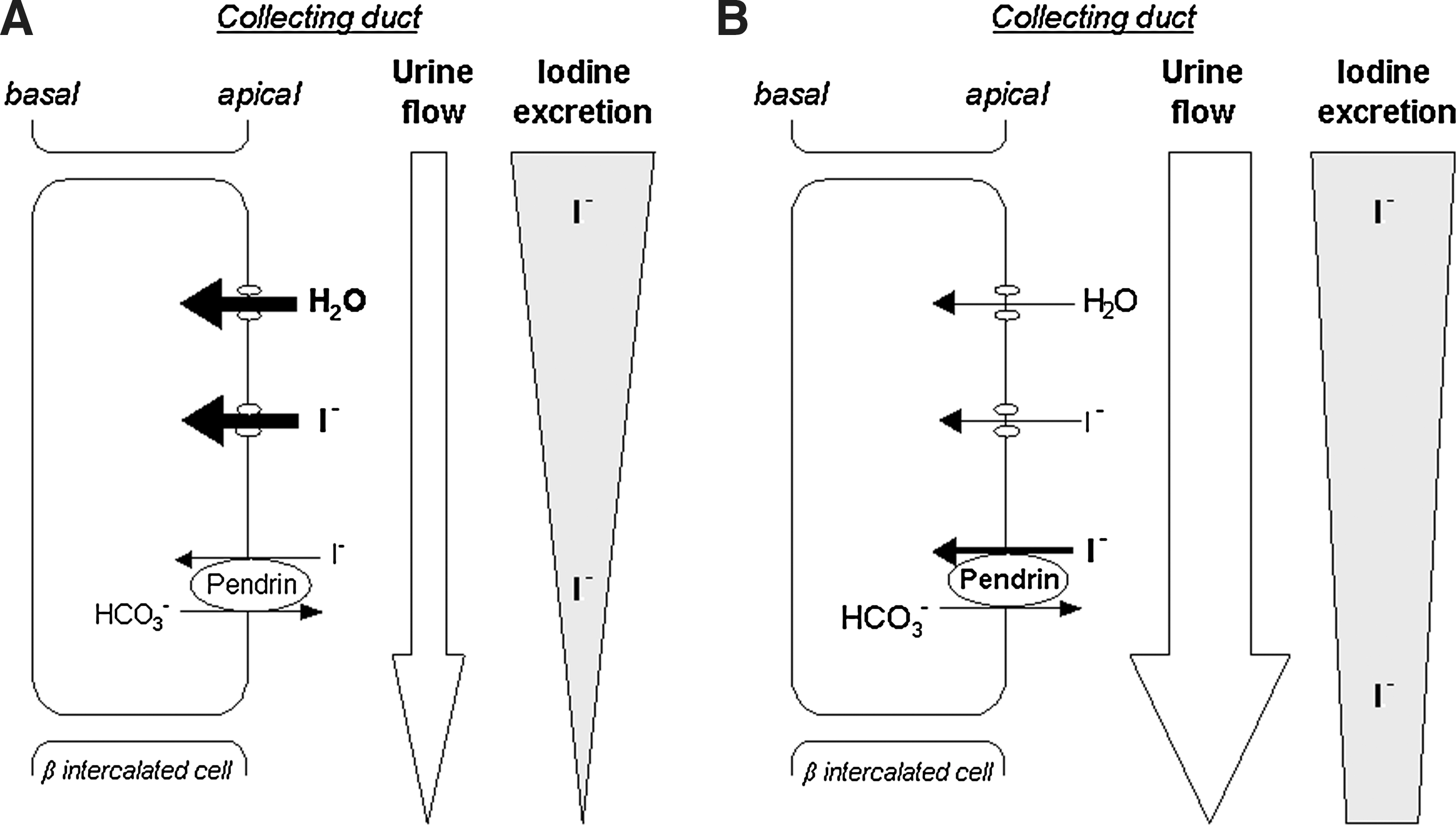
Suggested mechanism of iodine reabsorption in the collecting duct during
The obviously greater effect of 24-hour U-Vol on iodine excretion in girls than in boys (β = 17.1 vs. β = 10.5) may be explained by the typical sex differences in hydration balance (28,29). Boys normally show higher sweating rates than girls, mainly caused by higher physical activity levels (29 –31). As sweat can contain considerable amounts of iodine (about 37 μg/L) (32 –34), a physically very active male adolescent, with a suggestive sweat loss about 1.5 L, may lose up to 56 μg iodine through sweat, a fraction that does not contribute to the renal excreted amounts of iodine anymore. A higher sweating rate in boys additionally leads to lower U-Vol, and therefore perhaps to a higher stimulation of renal water and iodine reabsorption mechanisms, resulting in lower renal iodine losses. However, the sex differences in the U-Vol effects may also be simply due to statistical reasons. Higher values of energy-related U-Vol in girls, because of a higher consumption of water-rich foods and a lower physical activity, come along with a higher range of variability. This in turn facilitates the identification of a significant association in a statistical regression model.
Because most of the consumed drinks contain only small amounts of iodine, that is, 3–4 μg/L [tap water: 3.8 μg/L (35); mineral water: 1.8 μg/L (36); juices: <5 μg/L (37)], our analyses reveal that a high fluid consumption leads to an additional iodine loss through urine that is not compensated by the iodine intake of the fluids itself. For example, the additional consumption of 1 L tap water would contribute about 4 μg to iodine intake, but would result at the same time in an additional urinary iodine output of ∼15 μg. This implies an approximate hydration-status-dependent iodine loss of 11 μg with each additionally excreted liter of urine.
In conclusion, we could clearly show that 24-hour urinary iodine excretion rate is directly affected by U-Vol. Therefore, two main issues emerge from our analyses. First, as U-Vol may be very variable within a population, as well as between different populations (7), the correct interpretation of determinants of 24-hour urinary iodine excretion in statistical and epidemiological studies requires taking U-Vol as a potential confounder into account. Second, especially in those children, adolescents, and adults who show a relatively high water intake, an additional iodine loss exists. This further underscores the importance of promoting an adequate intake of iodine-rich foods.
Footnotes
Acknowledgments
The authors are very grateful to the staff of the Research Institute of Child Nutrition for carrying out the anthropometric measurements, and for collecting and coding the dietary records, and especially thank Monika Friedrich and Brigitte Nestler for expert laboratory assistance. The present examination was supported in part by the Federal Ministry of Food, Agriculture and Consumer Protection (BMELV) via the Federal Agency for Agriculture and Food (BLE). The DONALD Study is funded by the Ministry of Science and Research of North Rhine Westphalia, Germany.
Disclosure Statement
The authors declare that no competing financial interests exist.