
Abstract
Background:
Endocrine gland-derived vascular endothelial growth factor (Prok1) and prokineticin 2 (Prok2) are involved in the organ-specific regulation of angiogenesis, which is a crucial step toward cancer progression in most tumors, including those of thyroid gland. The oncogene BRAF V600E mutation is associated with poor clinical outcome of papillary thyroid cancer (PTC) and can independently predict its recurrence.
Design:
Our hypothesis was that Prok1 and Prok2 expression levels associated with BRAF mutations can be prognostic factors for PTC outcome. Prok1 and Prok2 were examined in PTC, a cell line derived from a human PTC (designated FB-2), euthyroid multinodular goiter (MNG), Graves' disease (GD), and contralateral normal thyroid (NT) tissues from PTC cases. We evaluated BRAF mutation and its relationship with Prok1 expression pattern in PTC.
Methods:
We studied Prok1 and Prok2 mRNAs by real-time polymerase chain reaction and BRAF mutation by mutant allele-specific polymerase chain reaction amplification. Formalin-fixed, paraffin-embedded blocks of PTC and NT were used for the immunohistochemical determination of Prok1 using anti-endocrine gland vascular endothelial growth factor primary antibody.
Results:
Prok1 and Prok2 transcripts were both present in thyroid tissues, and Prok1 was differentially expressed in PTC compared to MNG, GD, and NT. Prok1 mRNA levels were very low in NT and MNG and significantly higher in PTC, FB-2, and GD (p < 0.05). Prok1 protein was almost undetectable in NT but was highly expressed in all PTC samples having an infiltrative pattern of growth and lymph node metastases (p < 0.05). Further, the expression of Prok1 in PTC was associated with 60% of the samples being positive for the BRAF mutation (p < 0.05).
Conclusions:
We found that Prok1 is significantly increased in PTC, and its expression in PTC is related to BRAF mutation. These results suggest that Prok1 could be a new useful marker for thyroid cancer progression. Prok1 therefore could also be a potential target for novel therapeutic strategies, although the lack of functional data suggests caution against generalization of this assumption.
Introduction
Angiogenesis, the formation of new blood vessels from pre-existing vasculature, plays a key role in the development, growth, and metastases of carcinomas (20). Potential stimulators of angiogenesis, such as vascular endothelial growth factor A (VEGF-A), have been identified (21). Overexpression of VEGF has been documented in various malignancies, including PTC (22 –26). The level of VEGF expression appears to be closely correlated with tumor size, extra-thyroidal invasion, and stage, and is increased in PTC having BRAF mutation (26). Two new angiogenic factors that selectively act on the endothelium of endocrine gland (EG) cells have been described and named EG-derived VEGF (also called prokineticin1 and prokineticin2) (27,28). Prok1 and Prok2 act by inducing proliferation, migration, and fenestration of endothelium derived from adrenal capillaries, but not of other endothelium types, such as those derived from aorta, umbilical vein, and dermis (27). These peptides are structurally unrelated to VEGF, regulate diverse biological functions, and are particularly involved in angiogenesis. Prok1 and Prok2 exert their physiological functions through G-protein-coupled receptors named Prok receptor type 1 and Prok receptor type 2 (29 –31). Previously, we found that while prokineticins and their receptors, Prok-R1 and Prok-R2, are expressed at very low level in normal prostate, their levels are increased with prostate malignancy (32). It is still unknown whether prokineticins are present in normal thyroid (NT) and malignant thyroid or whether their level of expression is correlated with tumor malignancy and BRAF mutation.
Thus, in the present study we examined Prok1 and Prok2 expression in PTC using contralateral NT tissue as control, euthyroid goiter, Graves' disease (GD) tissue, and also A-2 thyroid cancer cell line named FB-2. We show in PTC tissue that there is a significant relationship between BRAF mutation and Prok1 expression levels, which has interesting implications for novel treatments of the disease.
Materials and Methods
RNA isolation
Total RNA was extracted from 30 tissue samples of PTC and 30 contralateral NT tissues from PTC cases, 20 euthyroid multinodular goiters (MNG), and 10 GD samples. All the patients were treated at the Endocrine Unit and underwent thyroidectomy at Endocrine Surgery Unit of the Department of Clinical and Experimental Medicine and Surgery, Second University of Naples, Italy. Patients with PTC were subjected to total thyroidectomy and prophylactic neck dissection. Tumor specimens were obtained in accordance with protocols approved by the institutional review board, and informed consent was obtained one day before surgery along with the consent to surgery. Tissue samples were immediately frozen at −80°C after surgery. RNA extracted from the FB-2 (TPC-1), a cell line derived from a human papillary thyroid carcinoma kindly supplied by Prof. Santoro M., Department of Endocrinology and Experimental Oncology, Naples, was included for controls. Total RNA was recovered with TRIZOL kit (Invitrogen). Residual DNA was removed by RNase-free DNase I treatment (Promega). To evaluate the expression of Prok1 and Prok2, real time-polymerase chain reaction (PCR) was performed in which these genes were amplified with glyceraldehyde-3-phosphate dehydrogenase as internal control (32,33). RNAs were reverse transcribed using 5 μg total RNA as previously described (33). To obtain a negative control for the amplification reactions, we carried out an RNA transcription without adding reverse transcriptase. cDNA (400 ng) obtained by reverse transcription (RT) of RNAs was amplified in a total volume of 50 μL containing 10 mmol Tris-HCl, 1.5 mmol MgCl2, 50 mmol KCl (pH 8.3), and 100 ng of 5′-3′ end primers.
The oligonucleotide primer sequences were Prok1 sense (5′CGCGAGTCTCAATCATGCTCCT-3′) and antisense (5′-GGCAAGGCGCTAAAAATTGATG-3′), and Prok2 sense (5′-TTGGCCTGTTTACGGACTTC-3′) and antisense (5′-TGCAAGAGGAGGGAAGAGAA-3′). Sequences used for glyceraldehyde-3-phosphate dehydrogenase are previously reported (33).
PCR products were then separated on a 1.2% agarose gel containing ethidium bromide using a 100-bp DNA ladder (Life Technologies) as size marker.
Real-time quantitative RT-PCR
RNAs were reverse transcribed using 5 μg total RNA as previously described (33). Real-time quantitative PCR was used to determine the amounts of Prok1 and Prok2 mRNA in FB-2, PTC, euthyroid MNG, GD, and contralateral NT tissues from PTC cases, as previously described (32). In these experiments, the amount of specific amplicon present was related to beta2-microglobulin and subsequently to an internal control. Real-time PCR was repeated three times for each sample using oligonucleotides Prok1 [5′-CCACATGTATCCCTCGGTCT-3′ (sense) and 5′-ACCTGGGACTCTGAGCAATG- (antisense)]; and Prok2 3′ [5′-CTTGCCTCTTCCACCTCAAA-3′ (sense) and 5′-TGCAAGAGGAGGGAAGAGAA-3′ (antisense)]. Real-time PCR was also repeated three times for a housekeeping gene, beta 2-microglobulin using the sense and antisense primers, 5′-CCAGCAGAGAATGGAAAGTC-3′, and 5′-GATGCTGCTTACATGTCTCG-3′, respectively. The iQ SYBR Green Supermix kit (Bio-Rad Laboratories) was used in an iCycler iQ Real-Time PCR Detection System (Bio-Rad Laboratories). Data are expressed as the amount of specific PCR products from each gene after normalization based on the housekeeping gene product beta2-microglobulin (which showed no significant difference).
Study population, clinic pathological data, and immunohistochemistry
Thirty-two patients affected by PTC were identified from the Italian University Hospital, “Ospedali Riuniti”—Foggia, Italy. All PTC patients received surgical treatment only with curative intention between 2003 and 2006. The histopathological diagnosis, reports about histological variants, and stage identification of all PTCs were made and carefully reviewed at the Section of Anatomic Pathology, Department of Surgical Science, University of Foggia. Tumor extent, determined from clinical records, was revised and classified according to the 2002 TNM classification (34). Demographical and clinic pathological features of PTC patients are summarized in Table 1.
PTC, papillary thyroid cancer.
Immunohistochemical staining
Four-micrometer serial sections from formalin-fixed and paraffin-embedded blocks were cut and mounted on poly-L-lysine-coated glass slides. Immunostaining was performed by linked streptavidin–biotin horseradish peroxidase technique. After sequential deparaffinization and rehydration, the slides were treated with 0.3% H2O2 for 15 min to quench endogenous peroxidase. Antigen retrieval was performed by microwave heating a first time for 3 min at 650 W, and a second and a third time at 350 W of the slides immersed in 10 mM citrate buffer pH 6. After microwaving, the sections were blocked for 60 min with 1.5% normal horse serum (Santa Cruz Biotechnology) diluted in phosphate-buffered saline buffer before the reaction with primary antibody (Ab). Primary monoclonal anti-EG-VEGF Ab (MAB1209; R&D Systems Inc.) was diluted 1:150 with 0.05 M Tris-HCl buffer pH 7.4 containing 1% bovine serum albumin and was incubated for 3 h as previously described (32). The specificity of the anti-EG-VEGF Ab and its immunohistochemical utilization technique has been previously described in the literature (32). The proliferative index of neoplastic epithelial cells was identified in different sections of each sample using a mouse monoclonal anti-Ki67 Ab (mouse monoclonal anti-Ki67, clone MB67, and Novus Biologicals) (data not shown). After two washes with phosphate-buffered saline, the slides were treated with biotinylated species-specific secondary Ab and streptavidin–biotin enzyme reagent (DAKO), and the color was developed by 3,3′-diaminobenzidine tetra hydrochloride chromogen solution. Sections were counterstained with Mayer's hematoxylin and mounted using the xylene-based mounting medium. Negative control slides without primary Ab were included for each staining. The results of the immunohistochemical staining were evaluated separately by two observers.
Immunostained cells, analyzed at 40 × with an optical microscope (Olympus BX41), were counted in at least 10 high-power fields.
For each case, the cumulative percentage of positive cells among all sections examined was determined. Inter-rate reliability between the two investigators blindly and independently examining the immunostained sections was assessed by the Cohen's K test, and yielded K values higher than 0.70 in almost all instances.
Genomic DNA extraction
Paraffin-embedded tumor samples from 32 PTC patients observed at Foggia Hospital and 18 fresh PTC samples from patients observed at Endocrine Units of the Second University of Naples were used to extract DNA for the exon 15 BRAF mutation analyses. Thus, the total number of PTC samples analyzed for BRAF mutation was from 50 patients. For nucleic acid extraction from paraffin-embedded tissues, 50 μm sections were immersed in xylene for 30 min to remove paraffin, and washed in absolute then 70% ethanol. All samples were subjected to digestion with 0.5% sodium dodecyl sulfate and 0.5 mg/mL proteinase K at 37°C overnight, and then extracted with TRIZOL following manufacturer's instructions. DNA concentrations were determined by absorbance at 260 nm using a BioPhotometer (Eppendorf), and the resulting genomic DNA (50–100 ng/sample) was used as a template.
PCR amplification of exon 15 segment of BRAF
Two primers (forward, 5′-TCATAATGCTTGCTCTGATAGGA-3′; reverse, 5′-GGCCAAAATTTAATCAGTGGA-3′) were used to amplify a 224 bp fragment of exon 15 of BRAF containing the site in which T1799A mutation occurs (35). PCR reactions were performed in 25 μL of buffer containing 1.5 mM MgCl2, 200 mM deoxynucleoside triphosphates, 50–100 ng genomic DNA, 0.5 mM of each primer, and 2.5 U Euro-Taq DNA polymerase (EuroClone). Thirty-five cycles with annealing temperatures optimized at 58°C were used to obtain the PCR product. Amplification products were separated on 1.2% agarose gel and observed by ethidium bromide staining.
Mutant-allele-specific amplification analysis of BRAF mutation
Mutant-allele-specific amplification was used to identify BRAF mutation as previously described (36). Two different forward primers with substitution of a single base at the end of the primer (5′-GTGATTTTGGTCTAGCTACAGT-3′and 5′-GTGATTTTGGTCTAGCTACAGA-3′) were designed to amplify the wild-type allele or BRAF T1799A transversion mutation, respectively. The sequence of the reverse primer was 5′-GGCCAAAATTTAATCAGTGGA-3′. PCRs were performed at 94°C for 2 min followed by 40 cycles of 94°C for 30 s, 52°C for 45 s, and 72°C for 45 s, and subsequent extension at 72°C for 8 min.
PCR products were analyzed in a 3% agarose gel stained with ethidium bromide. The presence of BRAF mutations was determined by direct sequencing of the PCR products.
Statistical analysis
The data were analyzed by the Stanton Glantz statistical software (version 6, Mc Graw Hill, 2007) and GraphPad Prism software version 4.00 for Windows (Graph Pad software,
Results
Prok1 and Prok2 mRNA expression in thyroid tissues
We studied Prok1 and Prok2 mRNA expression by quantitative RT-PCR using thyroid gland tissue derived from 30 PTC samples, 20 euthyroid MNG, and 10 GD tissues, with 30 contralateral NT tissues from PTC cases as controls; FB-2 thyroid cancer cell line samples were also analyzed (Fig. 1). We found that both Prok1 and Prok2 are present in NT and pathological thyroid tissues, as well as in the FB-2 cells (Fig. 1A). As shown in Figure 1B, Prok1 mRNA levels were differentially expressed in normal versus malignant tissues. Extremely low levels were found in NT and MNG samples, whereas in PTC, FB-2, and GD, levels were significantly increased (p < 0.05). In contrast, Prok2 transcripts were expressed at high levels both in control as well as in pathological tissues (Fig. 1B).
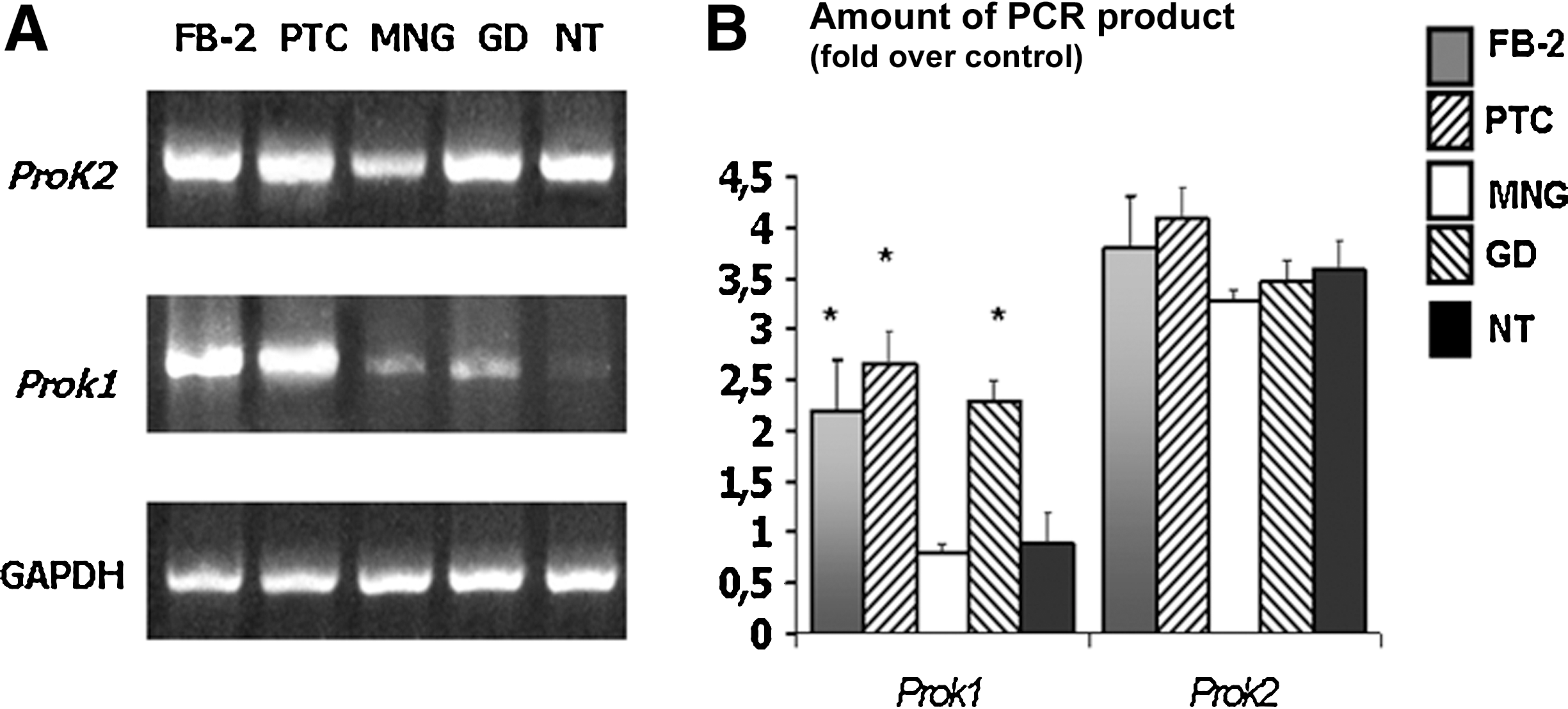
Prok1 and Prok2 mRNA expression in illustrative cases of the FB-2 cell line, papillary thyroid carcinoma (PTC), Graves' disease (GD), multinodular goiter (MNG), and normal contralateral thyroid tissues (NT) from PTC cases.
Prok1 protein levels in NT and PTC thyroid tissues
We observed a strong upregulation of Prok1 protein in PTC. Twenty-nine of 32 PTC cases (90.6%) showed positive immunostaning for Prok1 (Table 2). All conventional type cases of PTC stained positively for Prok1 (Fig. 2), whereas PTC variants showed heterogeneity ranging from negative (75% of follicular variants) to strong immunostaining (one sample of follicular variant shown in Fig. 3, and one of diffuse sclerosing variant). Statistical univariate analysis of Prok1 levels stratified by clinico-pathological findings is summarized in Table 2. In Table 2, the growth patterns of analyzed tumors were classified as expansive in the presence of pushing margins of invasion, and infiltrative in the presence of neoplastic cells (or glands) having irregular and sharply defined borders that infiltrate the perilesional thyroidal tissue. Infiltrative neoplasias were valued cases with nodal metastases and tumors without lymph nodal metastases; no metastases were observed for the expansive PTCs. The immunohistochemical study (Fig. 2) showed that Prok1 was almost undetectable in NT tissues, whereas an overall higher degree of the protein compared to NT was seen in PTC (p < 0.05). We particularly found a trend in Prok1 protein overexpression relative to primary tumor growth pattern and lymph node involvement. The higher mean percentage of Prok1 expression was observed in PTCs with an infiltrative pattern of growth and lymph node metastases (Table 2). Also, a significant trend in Prok1 protein upregulation relative to TNM staging was observed, whereas no statistically significant correlations with sex, age, tumor maximum diameter, and associated pathology was noted. Mean levels of Prok1 protein showed significant differences with respect to histological type (p < 0.05) (Table 2).

Immunohistochemical analysis of Prok1 in NT follicles and in papillary thyroid carcinoma cells (classic variant) at different pathological stages. Representative cases of formalin-fixed, paraffin-embedded PTC tissues were immune-stained for Prok1 as described in the Materials and Methods section. Although specific cytoplasmic Prok1 expression was not detected in NT follicles

Immunohistochemical analysis of Prok1 in a case of follicular variant of PTC from Hashimoto's thyroiditis.
SD, standard deviation; aANOVA, analysis of variance; bStudent-Newman-Keuls test.
BRAF mutation in PTC samples
Paraffin-embedded tumor samples from 32 PTC patients observed at Foggia Hospital and 18 PTC samples from patients observed at Endocrine Units of the Second University of Naples were used to extract DNA for the exon 15 BRAF mutation analyses. The total number of PTC samples analyzed for BRAF mutation was from 50 patients. The V600E mutation was found in 24 of 50 (48%) tumors, 4 examples of which are shown in Figure 4. Correlation between BRAF mutation and Prok1 expression was examined in 32 PTC cases described in Tables 1 and 2. BRAF was mutated in 15 of 32 (47%) classical PTC, and in 1 of 4 (25%) follicular variant PTC. With respect to invasion pattern, we found V600E mutation in all seven samples (100%) of PTC infiltrative with metastatic lymph node involvement and in 11 of 16 (68%) infiltrative with negative lymph node involvement. Thus, the BRAF mutation showed a positive trend of association with extra-thyroidal invasion.

Analysis of BRAF mutation in representative cases of PTC by mutant-allele-specific amplification. Genomic DNA was extracted from micro-dissected sections of representative PTC samples (PTC1-4), and analyzed for BRAF mutation by mutant-allele-specific amplification PCR using mutant or wild-type-specific primers as described in the Materials and Methods section. The 129-bp product was observed for all four samples using both primers. Lane (M) is the base pair ladder.
Prok1 was significantly upregulated in BRAF V600E (+) PTC, compared with BRAF V600E (−) PTC; expression of Prok1 was found in 60% of the PTC samples positive for the BRAF mutation (p < 0.01). These data therefore showed a significant trend in both Prok1 protein upregulation and BRAF mutation in tumors having an infiltrative pattern and lymph node involvement.
Discussion
Our data indicate that Prok1 and Prok2 are expressed in thyroid tissues, and show that Prok1 transcript is differentially expressed in NT and pathological thyroid tissues. Besides the well-known role for angiogenesis in cancer, it has become clear that it is also an integral component of a diverse range of non-neoplastic chronic inflammatory and autoimmune diseases, including GD (37). We find Prok1 mRNA highly expressed in GD tissues, whereas it has recently been reported that VEGF is expressed at very low levels in these tissues (38). Thus, Prok1 that is specific of endothelial cells derived from EGs could likely contribute to pathogenesis of structural changes, activation and proliferation of endothelial cells, as well as to capillary and venule remodeling in GD (27,28). We also observed a significant increase of Prok1 levels in PTC displaying an infiltrative pattern. While Prok2 expression levels are higher compared to Prok1, no significant differences are seen between NT and malignant thyroid tissues, suggesting a role for Prok1 in thyroid angiogenesis and tumor progression. Moreover, we observed a consistent relationship between BRAF mutation and Prok1 protein expression in PTC. Prokineticins and their receptors are involved in a wide spectrum of biological functions and pathologies of various tissue pathologies (39). The complexity and potential redundancy of this system remain unclear, and therefore progress of understanding pathological roles for prokineticins and the development of new target-specific therapies is hindered. The strong angiogenic effects of prokineticins are known, and their aberrant signaling, which may cause hyperplasia and hyper-vascularity in various tissues, has been highly associated with the development of polycystic ovarian syndrome, neuroblastoma, and testicular cancer (39,40). For example, Prok1 overexpression in a colorectal cancer line induces angiogenesis and tumors when implanted into nude mice (41). In ovary carcinoma, Prok1 expression is detected in the early stage and is reduced in advanced-stage of the disease (42). Our previous studies have demonstrated that prokineticins and their receptors are expressed in human prostate, and that their levels increase with prostate malignancy (32). Different studies have also shown an increased expression of VEGF in PTC (26). VEGF is upregulated in BRAF V600E (+) PTC, and this may provoke an increase in tumor growth and vasculature. In differentiated thyroid cancer studies, preliminary trial results using inhibitors of angiogenesis such as sorafenib, motesanib, axitinib, and vandetanib have shown promising effects (43). In particular, the immunoneutralizing antibodies or antagonists of prokineticins may be useful tools for new anti-cancer treatments (44).
In the last five years, more than 200 publications have described the relationship between BRAF V600E and thyroid cancer (45,46). In PTC, the mutation is associated with risk of recurrence or decreased recurrence-free survival (47), and somatic point mutations in the BRAF oncogene gene have been identified as the most common genetic event in PTC (∼44% of PTC cases) (12,48 –51). Indeed, we also find the BRAF mutation in 47% of the PTC cases studied, but in particular, BRAF V600E is detected in 84% of PTC with infiltrative pattern, and in 100% of cases with infiltrative pattern and metastatic lymph nodes at diagnosis. Since BRAF mutation is found in PTC samples displaying significantly higher Prok1 protein expression levels, this relationship strongly suggests that Prok1 plays a role in PTC tumor recurrence, and that it could be useful as a marker for thyroid cancer progression. Although Prok1 could also be a potential target for new therapeutic strategies in treating PTC cases with worse clinical outcomes, further studies will be required to define the exact molecular signaling mechanisms at various stages of tumor progression.
Footnotes
Acknowledgment
The authors express their gratitude to the following grant agency: Progetti di Ricerca di Interesse Nazionale (PRIN) (to D.P.). 2008 LFK7J5_002.
Disclosure Statement
The authors declare that no competing financial interests exist.