
Abstract
Background:
Currently bisphosphonates are often administered to patients with osteolytic bone metastases from several neoplasms. Based on favorable experience in other cancers with bone metastases and the lack of effective treatment, we started to use zoledronic acid (ZA), a recently developed synthetic bisphosphonate drug, in the treatment of this disease. In the present study, we retrospectively evaluated the efficacy of ZA for bone metastases from differentiated thyroid carcinoma.
Methods:
The study consisted of 50 patients with bone metastases from differentiated thyroid carcinoma treated at the Cancer Institute Hospital of Tokyo between 1976 and 2008. Among them, 28 patients who did not undergo bisphosphonate therapy were defined as group A and 22 patients who received ZA therapy were defined as group B. The primary efficacy endpoint for ZA treatment was the reduction in the percentage of patients who developed skeletal-related events (SREs), including bone fracture, spinal cord compression, and hypercalcemia. A secondary endpoint was the interval between a presentation of bone metastases and appearance of SREs.
Results:
SREs occurred in significantly lower frequency in group B (3 of 22 patients, 14%) than group A (14 of 28 patients, 50%) (p = 0.007). The use of ZA significantly retarded the onset of the first SRE (p = 0.04). Two group-B patients developed bisphosphonate-related osteonecrosis of the jaw.
Conclusion:
Treatment with ZA was effective in reducing SREs or delaying their appearance in patients with bone metastases from differentiated thyroid carcinoma.
Introduction
Patients and Methods
During a 33-year period from 1976 through 2008, a total of 1687 patients with papillary thyroid carcinoma (PTC, 1554), follicular thyroid carcinoma (FTC, 100), and medullary thyroid carcinoma (MTC, 33) underwent primary thyroid surgery at the Cancer Institute Hospital, Tokyo, Japan, a tertiary oncology referral center. The study population (Table 1) included 6 patients with PTC and 18 with FTC who were diagnosed to have bone metastases at the time of initial presentation (synchronous metastases), and 16 patients with PTC and 6 with FTC who were first diagnosed as having bone metastases during a follow-up period (metachronous metastases). There were also two patients with MTC who were not part of the study group but will be commented on in the discussion. In addition, four PTC patients with bone metastases (one synchronous and three metachronous), who have undergone initial thyroid surgery elsewhere, were referred to us because of treatment of bone metastases. As a result, a total of 50 patients with bone metastases from differentiated thyroid carcinoma were analyzed in the present study. The Japanese Society of Thyroid Surgery determined in 1991 that a finding of “poorly differentiated carcinoma” should be given for differentiated papillary or follicular carcinoma showing trabecular or solid proliferation even in small areas of a resected surgical specimen (8,9). As some patients were treated before 2004, when the 2004 World Health Organization classification of thyroid tumors was established, PTC and FTC with poorly differentiated histologic components were diagnosed as poorly differentiated carcinoma in this study. Among the 50 patients, as for PTC and FTC, 20 cases were histopathologically well-differentiated tumor (40%), 27 cases had poorly differentiated components (54%), and 3 cases were unknown. The first-presented bone metastases lesions were most commonly identified in vertebral bodies (n = 20) and pelvis (n = 12). Multiple skeletal lesions were present from the beginning in 28 patients (56%).
F/U, follow-up; RT, radiotherapy; RAI, radioactive iodine; Surg, surgery.
As ZA was officially approved in Japan as a drug for treating cancer patients with bone metastases in April 2006, 22 patients with bone metastases from thyroid carcinoma have received ZA as of September 2008, which was defined as group B, and the remaining 28 patients who have not undergone the drug therapy was defined as group A. Group A comprised 7 men and 21 women, including 17 PTC and 11 FTC. Mean age at bone metastases presentation was 59 years (range, 32–77 years). Mean duration of follow-up after detection of bone metastases was 45 months (range, 2–288 months). Group B consisted of 7 men and 15 women, including 9 PTC and 13 FTC. Mean age was 60 years (range, 40–73 years) and mean duration of follow-up was 26 months (range, 3–84 months). None of these patients were lost to follow-up.
ZA (Zometa®; Novartis Pharma AG, Basel, Switzerland/Novartis Pharmaceuticals Corporation, East Hanover, NJ) is a new bisphosphonate that has demonstrated greater potency than pamidronate or other commercially available bisphosphonates (10). The patients in group B received treatment with 4 mg ZA via a 15-minute intravenous infusion once a month, ranging from 1 to 33 times (average: 16 times). If necessary, the dose of ZA was reduced according to the renal function (creatinine clearance 60–50 mL/minute: 3.5 mg; 49–40 mL/minute: 3.3 mg; 39–30 mL/minute: 3 mg; <30 mL/minute or creatinine ≥3 mg/dL: stop). The 4 mg dose is approved for clinical use, because of concerns over renal function (6). Renal function was evaluated mainly using serum creatinine values and was monitored before each administration of ZA. These patients consulted dentistry before starting ZA therapy, and when oral infection including periodontitis was discovered, administration of ZA was not performed until dental health was completely obtained. Usually, it was deferred for 3 months after the completion of dental treatment. SREs were assessed at each visit and were defined as bone fracture, spinal cord compression, and hypercalcemia.
The treatments other than ZA for these 50 patients comprised surgical excision of the metastatic bone lesion in 9 patients (18%), external beam radiotherapy (RT) in 35 patients (70%), and radioactive iodine (RAI) therapy in 26 patients (52%). A combination of multiple therapies was used in 26 patients (52%), whereas 8 patients (16%) did not undergo any of these treatments. Among the 22 patients in group B, surgical excision has been undergone by 4 patients (18%), RT by 17 (77%), and RAI therapy by 11 (50%), whereas 3 patients (14%) have not received any other therapy. In the present study, most of these treatments were performed before starting ZA therapy because ZA came to be available in 2006. We recently started applying ZA therapy as soon as bone metastases were detected and simultaneously consulted orthopedists to decide on treatments to apply together with ZA.
The primary efficacy endpoint was the proportion of patients who experienced at least 1 SRE during the period of this study. The proportion of patients with SREs was compared between these two groups using chi-square test. Secondary efficacy endpoint was the interval from detection of bone metastases until the appearance of an SRE and was compared using the log-rank test. The events that occurred before the detection of bone metastases were not counted as SREs. As RT to bone and surgery to bone were used to palliate severe bone pain or treat skeletal fractures and spinal cord compression, these treatments were meaningful surrogate endpoints for pain and disease progression. Therefore, some other studies mentioned RT and surgery as SREs (11). Many patients in the present study, however, had already undergone RT or surgery before the ZA therapy started, as mentioned earlier, and thus, in the present study, neither RT nor surgery was counted as an SRE to study the efficacy of ZA.
This retrospective study has been approved by the institutional cancer board.
Results
Overall outcome
Of the 50 patients with bone metastases, 22 (44%) survived, 27 (54%) died of the disease, and 1 (2%) died from other disease. The cause of disease-specific death was distant metastases in all cases. Among the 50 patients, 30 (60%) showed distant metastases at other sites besides the bone. Bone metastases were detected by symptoms of skeletal pain (n = 28), mass bone lesions (n = 4), paralysis or numbness (n = 4), or bone fracture (n = 2). The remaining 12 patients (24%) initially had no symptoms related to bone metastases and were found to have bone metastases on postoperative RAI whole-body scanning (n = 6), routine imaging study (X-ray, computed tomography, and magnetic resonance imaging) (n = 4), bone scintigraphy (n = 1), and increased serum thyroglobulin concentration (n = 1).
Statistical analysis
In group A, bone fracture occurred in 2 patients, hypercalcemia in 1, and spinal cord compression in 13. As a result, 14 of 28 patients (50%) experienced one or two SREs during the observation period. In group B, 3 of 22 patients (14%) experienced an SRE (bone fracture in 1, spinal cord compression in 2). Statistical analysis revealed that treatment with ZA significantly reduced (Table 2) the proportion of patients with SRE during this trial period (p = 0.007, chi-square test).
SRE, skeletal-related event.
Treatment with ZA also delayed the onset of skeletal complications, significantly extending the time to first SRE (p = 0.04, log-rank test). The SRE-free 3-year survival rate without SRE after detection of bone metastases was 50% in group A and 86% in group B (p = 0.002, log-rank test) (Fig. 1).
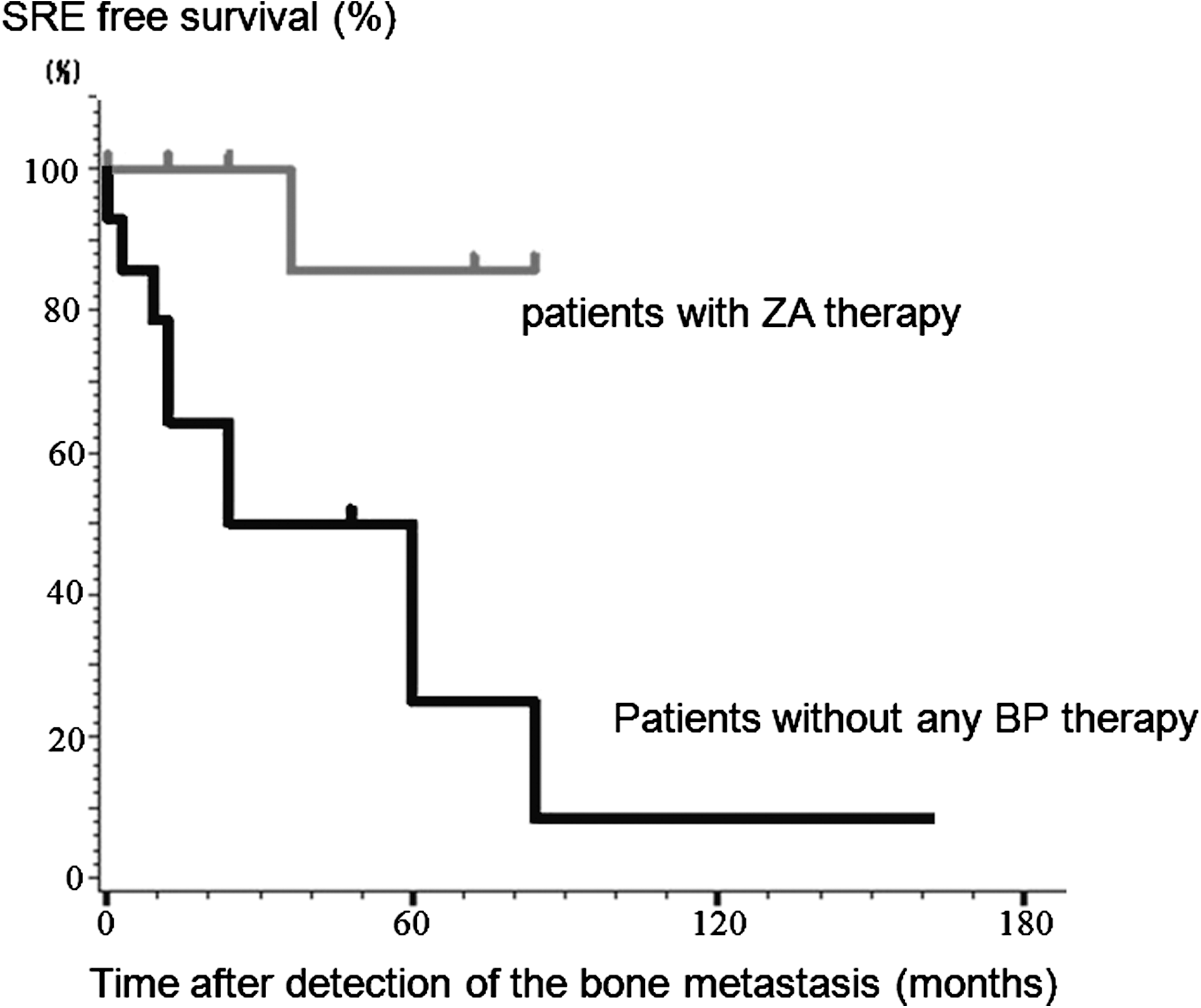
Survival curve of patients without skeletal-related events (SREs).
None of the treatments other than ZA (surgery, RAI therapy, and external beam RT) were associated with the proportion of patients with SRE or time to first SRE (p > 0.05).
Adverse events
The most common treatment-related adverse event was a transient flu-like syndrome with fever. This syndrome was associated only with the first administration of the drug, which then was attenuated and disappeared with subsequent administrations. We observed two patients (9%) with bisphosphonate-related osteonecrosis of the jaw (BRONJ) in group B. One patient underwent osteoplastic necrotomy and marginal excision of the jaw coupled with reconstruction with titanium plate, in combination with antibiotic therapy (Fig. 2). The other patient recovered by conservative dental treatment with antibiotics. No other serious adverse events, such as functional disorder of the kidney or liver, were observed.

Bisphosphonate-related osteonecrosis of the jaw. Breakdown of the surface bone and radiolucent change were observed (arrow).
Discussion
Certain actions are considered responsible for the beneficial effect of bisphosphonates in patients with bone metastases. The drug localizes in areas of the bone that are undergoing inflammation or resorption, inhibiting the formation of osteoclasts from precursor cells and/or their activity, triggering apoptosis of the osteoclasts, and thus decreasing osteoclast-mediated bone resorption (12). Recently, bisphosphonates have been administered to patients with osteolytic bone metastases caused by several neoplasms. ZA has produced significant reductions in skeletal complications among patients with bone metastases from breast cancer, prostate cancer, and a variety of other tumor types (6,13). In nonsmall cell lung carcinoma and other solid tumors, patients treated with 4 mg ZA were reported to have a 31% lower annual incidence of SREs compared with patients with placebo (6). The clinical response in bone metastases from breast and lung cancer during ZA treatment is inversely correlated to skeletal events (14). Preliminary studies suggest that bisphosphonates may prevent cancer-treatment–induced bone loss because of reduced estrogenic signaling caused by hormonal therapy (7), and moreover, they may even slow the progression of bone lesions or prevent metastases (15). In breast cancer, ZA therapy is associated with longer overall survival (16). Concerning thyroid carcinoma, 2 of 10 cases reportedly showed >50% decreases in bone metastatic lesions, and 5 patients achieved stabilization of bone lesions during the drug therapy (17). However, data on thyroid carcinoma are still limited, and we believe that this is the largest scale study of ZA therapy for bone metastases from thyroid carcinoma to date. The analysis of endpoints assessing SREs revealed that patients with bone metastases from differentiated thyroid carcinoma treated with ZA experienced fewer SREs and went significantly longer without experiencing a skeletal complication. It appears that monthly infusion of ZA is well tolerated and improves QOL. We have not noted antitumor activity as evidenced by decreasing size of bone metastases, however (15,17). ZA treatment should be continued until occurrence of treatment-related adverse events or a substantial decline in performance status (14), and through the use of other agents such as corticosteroids at the same time, or along with RT and surgical therapy, outcomes and QOL can be improved in patients with bone metastases (18).
We experienced two cases of BRONJ in the present study. BRONJ is defined as exposed necrotic bone in patients who have received bisphosphonates without history of RT to the jaws, which persists for at least 8 weeks. It is a serious adverse event, is difficult to treat, and adversely affects QOL (19). The cumulative prevalence of BRONJ ranges from 0.8% to 12% (20). Because the jaws have a greater blood supply than other bones and a faster bone turnover rate related to their daily activity and the presence of teeth, bisphosphonates are highly concentrated in the jaws (21). The cause of our BRONJ cases may be gingival inflammation, which occurred despite regular dental exams every 3 months. The range of treatments includes conservative management and surgical resection. The majority of patients undergo sequestrectomy (22). According to the staging and treatment strategies proposed by the American Association of Oral and Maxillofacial Surgeons, in the patients with exposed/necrotic bone following pain, infection, pathologic fracture, extraoral fistula, or osteolysis extending to the inferior border, whose BRONJ is defined as stage 3, mobile segments of bony sequestrum should be removed by surgery (20). Complete prevention of this complication is not possible currently, but pretherapy dental care should be continued indefinitely in an attempt to reduce its prevalence (21). We have observed no serious adverse events other than BRONJ to date. In the literature, the most common adverse events during ZA treatment were bone pain, nausea, anemia, emesis, constipation, and dyspnea (6). This may be because the majority of patients in large randomized, placebo-controlled trials of ZA consisted of those with nonsmall cell lung carcinoma and renal cell carcinoma (6,23). In thyroid cancer, the use of multiple therapies including RT, RAI therapy, and surgery, as well as the nature of the disease, may have minimized these adverse events.
Pyridinoline-crosslinked carboxy terminal telopeptide (ICTP), which seems to represent an indicator of pathologic bone resorption processes, offers a good serum metabolic marker for monitoring the therapeutic response of breast cancer that metastasizes to bone (24). Since 2004, ICTP levels of patients with differentiated thyroid carcinoma have been checked in our institution, revealing one patient's bone metastases; however, in about 60% of thyroid cancer patients, ICTP has not been a reliable indicator of bone metastases or amelioration of the symptoms of bone metastases (1).
One limitation of the present study might be bias introduced by the fact that the two groups of patients were treated at different times. As ZA came to be available in Japan in 2006, the group B mainly consisted of relatively new patients, whereas group A mainly consisted of patients who were treated before 2006. However, the therapeutic strategy for patients with thyroid carcinoma has not dramatically changed during these several decades. The other limitation might be the relatively short duration of follow-up after detection of bone metastases, especially in group B (26 months; range: 3–84 months). It has been reported that about 5% of the oncologic patients who had received bisphosphonate therapy for an average period of 4.4 years developed BRONJ, although majority of the patients in their study had been treated with pamidronate for multiple myeloma (25). More studies are needed to assess any long-term effect as well as adverse events of ZA in the treatment of bone metastases from differentiated thyroid carcinoma.
There have been a few studies on the effect of bisphosphonates in the treatment of bone metastases from MTC, and pamidronate was not effective in two MTC patients (17). We also have studied only two patients with bone metastasis from MTC (one with ZA therapy and one without) and both of them have not experienced any SRE.
In conclusion, these data suggest that ZA represents a safe, well-tolerable, and effective treatment for the palliation of differentiated thyroid carcinoma patients with symptomatic bone metastases. Further investigation will be required to determine whether the effects of ZA on bone metastases from differentiated thyroid carcinoma can translate into an overall disease-specific survival benefit as in the case of breast cancer (16).
Footnotes
Disclosure Statement
The authors have no conflicts of interest, potential conflicts, or financial relationships.