
Abstract
Background:
The impact of varying degrees of extrathyroid extension (ETE), especially microscopic ETE (METE), on survival in thyroid carcinomas (TC) has not been well established. Our objective was to analyze ETE at the molecular and histologic levels and assess the effect of its extent on outcome.
Methods:
All cases of TC with ETE but without nodal metastases at presentation (NMP) were identified over a 20-year period and grouped into gross and METE. Twelve papillary thyroid carcinomas (PTCs) without ETE and NMP were also analyzed. Cases with paraffin tissues were subjected to mass spectrometry genotyping encompassing the most significant oncogenes in TC: 111 mutations in RET, BRAF, NRAS, HRAS, KRAS, PIK3CA, and AKT1, and other related genes were surveyed.
Results:
Eighty-one (10%) of 829 patients in the database had ETE and no NMP. There was a much higher frequency of poorly differentiated and anaplastic carcinomas (12/29, 41%) in patients with gross ETE than in those with METE (3/52, 6%) (p < 0.01). There was a higher disease-specific survival (DSS) in patients with METE than in those with gross ETE (p < 0.0001). Except for an anaplastic case, no recurrences were detected in 45 patients with METE, including 23 PTC patients followed up for a median of 10 years without radioactive iodine therapy. Within patients with gross invasion into trachea/esophagus, tumors with high mitotic activity and/or tumor necrosis correlated with worse DSS (p < 0.05). Fifty-six cases with ETE were genotyped as follows: BRAFV600E, 39 (70%); BRAFV600E-AKT1, 1 (1.8%); NRAS, 1 (1.8%); KRAS, 1 (1.8%); RET/PTC, 3 (5%); wild type, 11 (19.6%). Within PTCs, BRAF positivity rate increased the risk of ETE (p = 0.01). If PTC follicular variants are excluded, BRAF positivity does not correlate with ETE status within classical/tall cell PTC.
Conclusion:
(i) PTCs with METE without NMP have an extremely low recurrence rate in contrast to tumors with gross ETE. (ii) High mitotic activity and/or tumor necrosis confers worse DSS even in patients stratified for gross ETE in trachea/esophagus. (iii) BRAF positivity correlates with the presence of ETE in PTC, but this relationship is lost within classical/tall cell PTC if follicular variants are excluded from the analysis.
Introduction
The clinical importance given to ETE is apparent in the staging systems that upstage patients to T3 in the tumor-node-metastasis American Joint Committee on Cancer staging system, and intermediate risk of recurrence in the American Thyroid Association system for even minor ETE present in the absence of other high-risk pathologic features (worrisome histology, primary tumor size, lymph node metastases, or vascular invasion) (5,6). This upstaging often results in recommendations for routine use of radioactive iodine (RAI) ablation in patients with any degree of ETE.
However, in the vast majority of studies on the subject, ETE has been categorized as present or absent lumping together gross ETE with even very minimal microscopic ETE (METE) seen only after very careful histologic review of the entire tumor specimen. Very few articles have addressed the prognostic significance of differing degrees of ETE (e.g., microscopic vs. gross) (7). Therefore, to better understand the impact of varying degrees of ETE on the risk of recurrence and disease-specific survival (DSS), we undertook a detailed clinicopathologic and molecular analysis of patients with follicular cell-derived TCs without concurrent locoregional or distant metastases but with ETE. In many of these patients, the decision regarding the need for RAI ablation would largely hinge on the clinical importance attributed to the ETE.
Materials and Methods
Patient population and inclusion criteria
The institutional database was searched for all cases with a diagnosis of TCs treated at Memorial Sloan-Kettering Cancer Center between January 1980 and December 2002. The slides from the cases included in the study were examined by two head and neck pathologists with special interest in thyroid neoplasia (R.A.G. and M.R.). The pathologists were blinded to the clinical outcome of all patients studied. The TCs were classified according to the last World Health Organization classification of endocrine tumors except for PTC, tall cell variant, and poorly differentiated TCs (8). The latter tumor was defined as a carcinoma displaying high mitotic activity (≥5 mitosis/10 high-power fields, 400×) and/or tumor necrosis, and showing follicular cell differentiation at the morphologic or immunohistochemical level. Tall cell variant was characterized as a papillary carcinoma composed of >50% of tall cells. The latter cell type was defined as having a height at least twice its width with an oncocytic cytoplasm. The term “high grade” in this article encompasses poorly differentiated TC and anaplastic TC.
All carcinomas of follicular cell origin with ETE but without lymph node metastasis at presentation were included in the study. In addition, a control group of TCs of follicular cell origin without ETE and lacking nodal metastases at presentation (NMP) was randomly selected from this database. The study was approved by the Institutional Review Board of Memorial Sloan-Kettering Cancer Center.
Histopathologic analysis
The largest dimension of the tumor was recorded as dictated during gross examination. The mitotic rate of the tumor was determined by counting 10 contiguous high-power fields (400×) using an Olympus microscope (U-DO model BX-40; Olympus America, Inc., Melville, NY). Using that microscope type, these 10 high-power fields correspond to 2.4 mm2. Mitotic counts were performed in a focused fashion, examining areas that appeared to show greater proliferative activity. Tumor necrosis was defined by a comedo-like appearance composed of degenerating cytoplasm and punctate, karyorrhectic nuclear debris. The presence of fibroblastic stromal reaction, hemorrhage, or an identifiable needle track in the necrotic area was attributable to reaction induced by prior fine-needle aspiration, and was therefore not regarded as spontaneous tumor necrosis. The tumor was categorized as completely encapsulated if its entire circumference was surrounded by a fibrous capsule. When present, the numbers of foci of capsular and vascular invasion were noted. Only complete penetration of the capsule by tumor was regarded as capsular invasion as described by Lang et al. (9). The presence of vascular invasion was noted only when such foci were present within or beyond the capsule in accordance with criteria outlined by the Armed Forces Institute of Pathology fascicle (10). Only when the invasive focus protruded into the lumen of the vessel in a polypoid fashion covered by endothelial cells, or when attached to the vessel wall or associated with thrombus formation was it considered true vascular invasion. Areas of vascular invasion that were closely adjacent to one another were counted as separate foci. Capsular invasion was subdivided into focal (<4 invasive foci) and extensive (≥4 foci). Angioinvasion invasion was categorized as significant (≥4 invasive foci and/or extrathyroid vascular invasion) and not significant (<4 invasive foci and no extrathyroid vascular invasion). ETE was defined as tumor cells invading beyond the thyroid capsule into perithyroid soft tissue or organs. ETE was subdivided into (i) microscopic focal: presence of 1–2 microscopic foci of ETE measuring ≤1 mm each. No gross ETE (ii) microscopic established: presence of >2 microscopic foci of ETE (≤1 mm in size each) or any foci >1 mm in size. No gross ETE (iii) Gross ETE: gross invasion of extrathyroid tissue/organs identified by the surgeon during the operative procedure (Figs. 1 and 2). For that purpose, all operating room reports were reviewed. The type of perithyroid tissue or organ invaded by the tumor was recorded (e.g., adipose tissue, skeletal muscle, recurrent nerve, trachea, and esophagus). The status of the resection margins was reported as positive (tumor presents at the surgical margin) or negative (no tumor at surgical margin).

Eighty-five-year-old woman with a 2.8-cm classical papillary carcinoma with tall cell features BRAF mutated that has grossly invaded skeletal muscle and trachea. The patient died with disease.
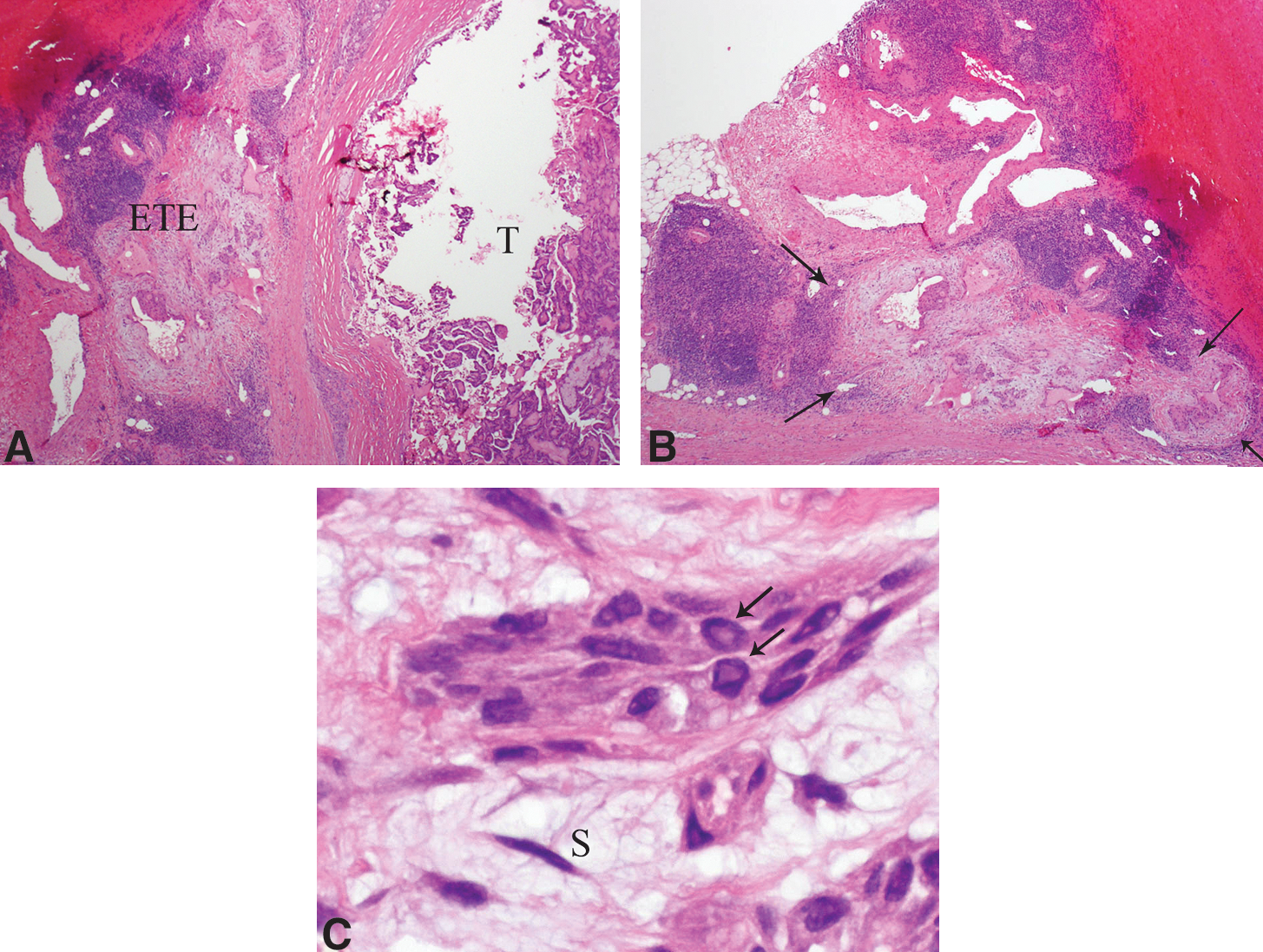
Fifty-four-year-old woman with a 1-cm classical papillary carcinoma showing microscopic extrathyroid extension (ETE). The patient is alive with no evidence of disease 9.3 years after diagnosis despite lack of radioactive iodine therapy.
Clinical parameters
The patient's electronic medical records were reviewed for the age at diagnosis, type of surgery, and adjuvant treatment including RAI therapy. The current disease status was based on a combination of physical examination, biochemical serum markers (thyrotropin and thyroglobulin), RAI dosimetry, cross-sectional imaging, and/or positron emission tomography scanning. The date of initial surgery and last date of follow-up were recorded. The status at last follow-up was recorded as follows: no evidence of disease, alive with disease, dead of other causes, and dead of disease.
Genotyping by mass spectrometry
Four sections of 10 μm from each formalin-fixed, paraffin-embedded tissue block were subjected to DNA extraction using the PUREGene Genomic DNA purification kit (Gentra, Inc., Minneapolis, MN). Mutation detection was performed as described previously (11). We used mass spectrometry Sequenom-based genotyping assay (Sequenom Mass Array; Sequenom, San Diego, CA), which is especially suited for high-throughput genotyping, to interrogate 111 known mutations in 16 different genes: BRAF, RET, NRAS, HRAS, KRAS, PIK3CA, MAP2K1, AKT1, MET, IKBKB, PIK3R5, PRKCZ, RHEB, RPS6KA3, RPS6KB1, and FRAP1. As the mass spectrometry genotyping assays for codons 12 and 13 of HRAS were not informative, we designed primers for this region and sequenced all the tumors that were wild type for BRAF, RAS mutations, or for RET/PTC rearrangements (11).
Screening for RET/PTC and PAX8-PPARγ rearrangements
We used tumor cDNA as template for quantitative polymerase chain reaction (PCR) to analyze for unbalanced expression of exons 10–11 relative to 12–13 of RET, which flank the rearrangement site in intron 11. Samples with 12–13 > 10–11 expression were screened for specific RET recombination events using primers bracketing the fusion point of RET/PTC1, RET/PTC2, and RET/PTC3, respectively, as previously described (11,12). We screened for the PAX8-PPARγ fusion by reverse transcriptase (RT)-PCR, using primers for the different possible transcripts of PAX8-PPARγ as previously described (13). PCR products were resolved by electrophoresis in a 2% agarose gel and selected cases were sequenced. RET and PAX8-PPARγ rearrangements were analyzed for tumors that were wild type for RAS and BRAF.
Statistical analysis
Two-tailed Fisher exact test was used to assess the relation between categorical variables. Survival probabilities were estimated by the Kaplan–Meier method and compared using the log-rank test (GraphPad Prism 5.01; GraphPad, San Diego, CA) A probability (p) value <0.05 was considered as significant. Adverse outcome was defined as the presence of disease at last follow-up whether the patient was alive or dead. The time interval to adverse outcome was calculated from the date of initial surgery to last follow-up. DSS was defined as the presence or absence of death of disease at last follow-up. The time interval to DOD was calculated from initial surgery to last follow-up. Multivariate analysis was performed using a Cox regression model and log rank statistics. This statistical analysis was carried out using SPSS for windows version 11.01(SPSS, Inc., Chicago, IL).
Results
Clinicopathologic data on patients with ETE
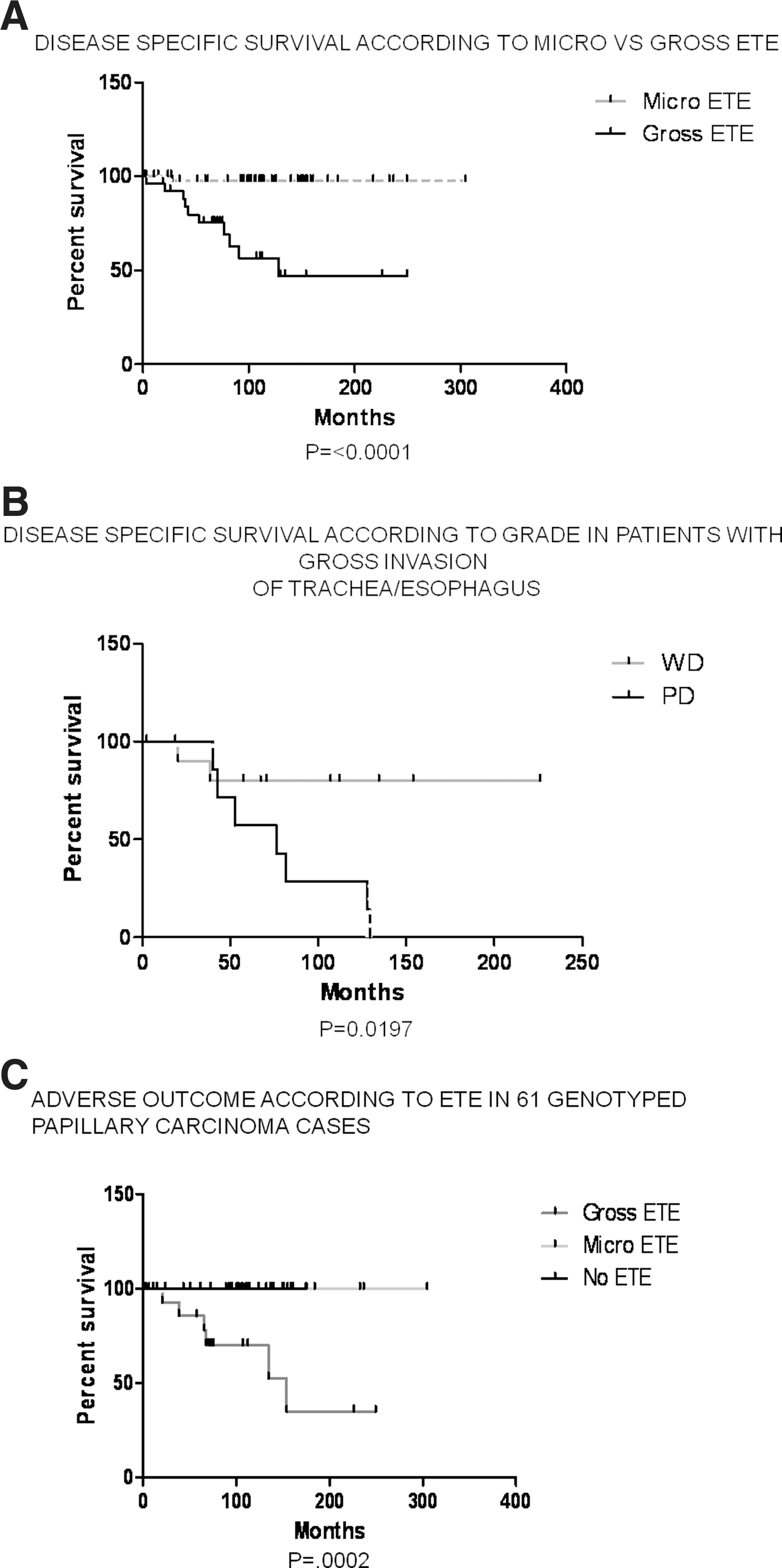
Out of 829 carcinomas of follicular cell origin in the database, 332 (40%) harbored ETE. Eighty-one (10%) of the 829 tumors displayed ETE without NMP and were therefore included in the study. Tables 1 and 2 shows the clinicopathologic features of the tumors, including their histotype according to various extent of ETE. Patients with gross ETE were older and had larger tumor, a higher rate of positive margins, and more significant vascular invasion than those with METE (p < 0.05). Carcinomas with gross ETE were of a higher proliferative grade (i.e., poorly differentiated and anaplastic) and were more often treated with RAI than their counterparts with METE (p < 0.05). More importantly, carcinomas with gross ETE had a more adverse outcome and worse DSS than patients with METE (p < 0.0001, Fig. 3A). Only 1 out of 46 patients with METE relapsed (Table 3). This was a 70-year-old woman with a 2.1-cm anaplastic carcinoma who displayed microscopic established ETE into skeletal muscle and died of disease 2 years and 2 months after diagnosis. All other cases with METE and adequate follow-up did not recur, including 24 patients who did not receive adjuvant RAI therapy followed up for a median of 9.7 years (Fig. 2). There was no survival difference between patients with microscopic focal and those with microscopic established ETE. In patients with gross ETE, the type of the invaded structure (muscle vs. trachea/esophagus) did not have an impact on adverse outcome or DSS (p = 0.2).However, the presence of a large tumor, significant angioinvasion, and higher grade significantly decreased DSS in this group of cases (p < 0.05). Also within patients with gross ETE, there was a trend toward adverse outcome (i.e., presence of disease at last follow-up) for those patients with large size, older age, and significant angioinvasion (p = 0.06, 0.08, and 0.05, respectively), while higher grade conferred adverse outcome in a statistically significant manner (p < 0.05). In a multivariate model including grade, tumor size, and vascular invasion, grade was the only independent predictor of adverse outcome in patients with gross ETE. For high grade, the hazard ratio (95% confidence interval) [HR (95% CI)] was 3.8 (1–14) (p = 0.04). For large tumor size, HR (95% CI) was 1.8 (0.4–7.8) (p = 0.45). For significant vascular invasion, HR (95% CI) was 1.2 (0.3–4.5) (p = 0.76).
ETE, extrathyroid extension; FVPTC, follicular variant papillary thyroid carcinoma; micro, microscopic; PD, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma.
Fisher exact test, two-tailed values.
Exact tumor size was available in 26 patients with gross ETE.
Significant VI defined as extensive VI or angioinvasion of extrathyroid vessel.
Margin status unavailable in one patient with microscopic focal ETE.
The exact nature of the surgery could not be determined in one case with gross ETE.
RAI status was available in 20 cases with focal microscopic ETE, 29 with microscopic established ETE, and 28 with gross ETE.
Adverse outcome was defined as the presence of disease at last follow-up. Adequate follow-up data were available on 18 cases with focal microscopic ETE, 28 with microscopic established ETE, and 27 with gross ETE.
RAI, radioactive iodine; TT, total thyroidectomy; VI, vascular invasion.
The only patient with adverse outcome had anaplastic carcinoma. All other cases did not recur.
Within 19 patients with gross invasion into trachea/esophagus, higher grade correlated with adverse outcome and worse DSS (p = 0.048 and 0.02, respectively, Fig. 3B). Within the same cohort of patients, large tumor size was able to confer adverse outcome and worse DSS (p = 0.035 and 0.014, respectively). In a multivariate model including grade and large tumor size, none was an independent predictor of adverse outcome. For high grade, HR (95% CI) was 2.3 (0.5–10.1) (p = 0.28). For large tumor size, HR (95% CI) was 4.0 (0.7–25.0) (p = 0.13).
Clinicopathologic data on control PTC group without ETE
This group had a median age of 52.5 years and consisted of nine women and three men. The tumors were classified as papillary microcarcinoma (n = 1), encapsulated follicular variant PTC (FVPTC) (n = 6), classical PTC (n = 4), and PTC tall cell variant (n = 1) with a median tumor size of 3.0 cm. Nine of 12 carcinomas were encapsulated (75%). Margins were positive for carcinoma in 2 (17%) of 12 cases. Of the 11 cases with available RAI status, 6 received RAI therapy and 5 did not. Seven patients underwent a one- or two-stage total thyroidectomy, whereas four patients had a lobectomy and one patient an isthmusectomy. Out of the 11 patients with adequate follow-up, 1 patient recurred and all were alive with no evidence of disease at last follow-up (Median follow-up: 10.6 years).
Genotyping analysis
Fifty-six cases with ETE and all control PTC cases (n = 12) without ETE had paraffin blocks available for genotyping. Tables 4 and 5 depict the genotyping results according to histotype in those patients with and without ETE. The vast majority of cases with ETE (72%) had BRAFV600E mutations, whereas the control PTC without ETE had a BRAFV600E positivity rate of 42%. Table 6 displays the clinicopathologic features according to BRAFV600E status in patients with PTC whether displaying or lacking ETE. There was a trend toward older age in patients with BRAF-mutated PTC compared to their non-BRAF-mutated counterparts (p = 0.077). BRAF-mutated PTC were less often encapsulated than non-BRAF-mutated tumor (p = 0.01). ETE was higher in BRAF-mutated PTC (38/43, 88%) than in non-BRAF-mutated carcinoma (11/18, 61%; p = 0.029). In patients without gross ETE, there was a trend toward higher METE in BRAF-mutated neoplasms (25/30, 83%) than in non-BRAF-mutated tumors (9/16, 56%; p = 0.08). When the analysis was restricted to classical and tall cell PTC, there was no significant difference in the ETE positivity rate between BRAF-mutated (34/39, 87%) and non-BRAF-mutated tumor (8/8, 100%; p = 0.57). BRAF-mutated PTC had more adverse outcome and worse DSS than non-BRAF-mutated PTC, but this correlation did not reach significance (p = 0.11 and p = 0.44, respectively). Within the genotyped PTC cases, patients with gross ETE had more adverse outcome than those with METE/absent ETE (p = 0.0002). There was no difference in survival between patients with METE and those lacking ETE (Fig. 3C).
Fisher exact test, two-tailed values.
The tumor size was not available in one case.
Significant VI defined as extensive VI or angioinvasion of extrathyroid vessel.
RAI therapy status was not assessable in two cases.
Outcome data were unavailable in four cases.
Discussion
The above data demonstrates the need for stratification of ETE into gross and microscopic. In contrast to common belief, not all ETE is associated with adverse prognosis. Indeed, METE did not confer a significantly worse survival in our patient population. In our group of 61 genotyped PTC, there was no difference in survival between those patients with METE and those lacking ETE. The only patient with METE who had an adverse outcome had an anaplastic carcinoma. These results are congruent with those of Ito et al., who did not find a survival difference between PTC with minimal ETE compared to those with absent ETE (7). These authors had a higher recurrence rate in their minimal ETE group in comparison to ours (7.8% vs. none in our PTC cohort). This could be due to the fact that our analysis was restricted to cases without NMP, whereas Ito et al. (7) included patients with nodal disease at diagnosis. A unique aspect of our study is the finding that nonanaplastic TCs with METE do not recur even if treated by surgery alone without RAI therapy. Indeed, all 24 patients with METE but no RAI therapy did not recur despite a median follow-up of 9.7 years (Table 3). We also did not find any difference in survival between patients with microscopic focal ETE and those with microscopic established ETE. It is important to mention that microscopic focal ETE (at least as defined in our study) is subject to significant interobserver variability even among our own group. This is due to the fact that the capsule of the thyroid can be incomplete, and fat and skeletal muscle can be found inside the thyroid parenchyma, whereas non-neoplastic follicles can be seen in perithyroid soft tissues (14). While METE appears to have no effect on prognosis, gross ETE significantly decreased the prospects for survival. More than half of our patients with gross ETE had an adverse outcome (59%). Gross ETE was also significantly associated with all the known poor prognostic clinicopathologic variables such as older age, large tumor size, significant angioinvasion, positive margins, and high grade (i.e., poorly differentiated and anaplastic carcinomas). Within patients with gross ETE, the type of tissue/organ invaded by the carcinoma (muscle vs. trachea/esophagus) did not impact outcome, whereas tumor size, significant angioinvasion, and grade decreased DSS significantly. Furthermore in multivariate analysis, grade was the only independent predictor of adverse outcome (i.e., presence of disease at follow-up) in patients with gross ETE. The adverse effect of grade and tumor size on survival remained significant even when the analysis was restricted to patients with gross invasion into trachea/esophagus. It is noteworthy that all high-grade tumors in that particular subgroup were poorly differentiated TCs defined on the basis of high mitotic activity and/or tumor necrosis (i.e., proliferative grading) rather than on solid growth (architectural grading) (3). The fact that proliferative grading is able to stratify TCs of a very similar pT category (gross ETE into trachea/esophagus) demonstrates the high value of grading TCs on the basis of high mitotic rate and tumor necrosis. The poor survival of these poorly differentiated carcinomas related to the inability of these high-grade tumors to concentrate RAI. Indeed, poorly differentiated TCs defined on the basis of high mitotic activity and/or tumor necrosis have been shown to constitute the majority of RAI refractory Fluoro-oleoxy glucose-positron emission tomography-positive TCs (15). In contrast, the relatively better outcome of well-differentiated tumor with gross ETE may be attributed to better avidity for RAI.
While the prognostic value of ETE has been extensively analyzed, there are relatively fewer studies on its molecular aspects. The presence of BRAFV600E mutation has been shown to be associated with ETE and poorer outcome in PTC by some authors (16,17). Other investigators, however, did not find a correlation between BRAFV600E mutation and ETE in PTC (18). In our PTC population, there was a statistically significant correlation between BRAFV600E mutation and the presence of ETE, confirming the findings of Adeniran et al. and Xing et al. (16,17). This relationship was, however, lost when the analysis was restricted to classical/tall cell variant of PTC. This is due to the fact that many PTC without ETE are encapsulated FVPTC that harbor no or very few BRAF mutations (16). Indeed, none of our encapsulated FVPTC displayed ETE or BRAF mutations. The only FVPTCs that harbored BRAFV600E mutation were infiltrative FVPTC displaying ETE. The statistically significant correlation between BRAF mutation and lack of tumor encapsulation in our study reflects the strong association between BRAF mutation and infiltrative forms of PTC (i.e., classical, tall cell PTC). Although more studies are needed, our results seem to indicate that BRAF is not independent from tumor subtype in predicting ETE in PTC. More importantly, the fact that BRAF correlates with ETE and infiltrative variants of PTC suggests that it has an important role in local invasion and therefore constitutes a potential target for therapy. Toward that goal, the molecular basis of invasiveness in BRAF-mutated tumors is being studied. Mesa et al. have shown that cell lines harboring BRAFV600E preferentially increase expression of metalloproteinases (19). The latter enzymes known to promote tumor invasion have been found in highly infiltrative TC such as the tall cell variant of PTC (20). Knauf et al. have shown that BRAFV600E induces epithelial–mesenchymal transition (a key phenomenon in tumor invasiveness) in thyroid cells from BRAF transgenic mice (21).
The above data may have important clinical implications. The current American Joint Committee on Cancer staging system staging should be reconsidered in regard to PTC patients with METE. As stated by Ito et al., PTC with METE measuring <4 cm may not need to be upstaged into the pT3 category but rather characterized as pT2 neoplasms (7). Countless number of patients with small carcinomas (especially microcarcinomas) with METE could be spared unnecessary adjuvant RAI therapy with its side effects. Finally, proliferative grading of TCs provide important prognostic information even in patients with gross ETE and should be included in the pathology report.
Disclosure Statement
The authors declare that no competing financial interests exist.