
Abstract
Background:
Sorafenib has shown promise in the treatment of patients with advanced or metastatic thyroid carcinoma. However, the optimal dose has not been established and data on Chinese population are not available. We conducted a study to assess the responses to sorafenib at a low dose of 200 mg twice daily in patients with progressive radioiodine-refractory pulmonary metastases from papillary thyroid carcinoma (PTC).
Patients and Methods:
Eligible patients received sorafenib 200 mg orally twice daily. Responses were assessed using Response Evaluation Criteria in Solid Tumors and adverse events were assessed periodically. The end points included response rate and progression-free survival.
Results:
Nine patients with radioiodine-refractory PTC were enrolled in the study and treated for a minimum of 13 weeks. The objective partial response rate was 33%. The stable disease rate was 44%. The mean progression-free survival was 42 weeks (95% confidence interval, 29.5 to 53.9). Two patients showed disease progression, and one of them died at 4 months after beginning of treatment. There was a marked and rapid change in the serum thyroglobulin level after start of treatment, with a mean decrease of 60% within 12 weeks, consistent with radiographic findings. Although the types of toxicities were consistent with other sorafenib trials, their severity was relatively mild. None of the patients discontinued sorafenib or reduced their dose because of treatment-related adverse events.
Conclusion:
Sorafenib at a dose of 200 mg twice daily has a potential therapeutic effect and is well tolerated in Chinese patients with PTC and radioiodine-refractory pulmonary metastases. Further study is warranted with a larger cohort of patients.
Introduction
Alternatively, systemic therapies using a variety of single- and combination-agent regimens have been used to treat patients with metastatic disease unresponsive to or unsuitable for surgery, RAI, or chronic suppression of thyrotropin (TSH). Doxorubicin, the only U.S. Food and Drug Administration-approved therapy, has low response rates, short duration of responses, and cardiotoxicity associated with prolonged treatment, making it a poor option (5).
Recently, a growing understanding of molecular oncology has allowed the development of targeted agents in different types of advanced thyroid carcinoma, offering great hope (6). For example, tyrosine kinase inhibitors have emerged as significant targets for novel cancer therapies (7). Sorafenib is an oral, small-molecule tyrosine kinase inhibitor targeting VEGFRs, RET/PTCs, and BRAF-mediated events (8). Sorafenib (400 mg, bid) has been used in selected patients with thyroid carcinoma. However, the optimal dose has not been completely established for thyroid carcinomas in the Chinese population (9). We, therefore, conducted a preliminary study to assess the response to sorafenib at a low dose of 200 mg twice daily in Chinese patients with radioiodine-refractory pulmonary metastases from PTC.
Methods
Patients
PTC patients with radioiodine-refractory pulmonary metastases after total or nearly total thyroidectomy were eligible to be enrolled in the study. Specifically, they had tumor lesions identified by the presence of circulating thyroglobulin (Tg) and anatomic examinations and they had no radioiodine uptake on post-RAI treatment scans. These were performed when the patients were on a low-iodine diet and had appropriately elevated serum TSH. All patients who were enrolled had evidence of disease progression within 12 months prior to initiation of treatment despite taking enough thyroid hormone to reduce their serum TSH to ≤0.1 mU/L. Other eligibility criteria included Eastern Cooperative Oncology Group performance status of <2, life expectancy >3 months, leukocyte count ≥3000 cells/μL, absolute neutrophil count ≥1500 cells/μL, platelets >100,000 cells/μL, hemoglobin ≥9 g/dL, serum creatinine ≤1.5 × upper limit of normal (ULN), serum bilirubin ≤1.5 × ULN, serum AST ≤2.5 × ULN, alkaline phosphatase ≤2.5 × ULN, and prothrombin time-international normalized ratio/partial thromboplastin time ≤1.5 × ULN. Premenopausal women were required to have negative pregnancy tests, and all patients of childbearing potential were required to use contraception. None of the patients had brain metastases.
Approval for the protocol was received from the ethics board before the beginning of the study. All subjects gave written informed consent for participation in the study.
Gene screening
Paraffin-embedded tumor tissues from the surgeries for the primary tumor or metastasis were collected and the presence of PTCs was confirmed by pathological examination. After deparaffinization, tissue fragments were subjected to manual punching microdissection and subsequent extraction of total RNA. Reverse transcription–polymerase chain reaction (RT-PCR) was carried out to detect RET/PTC rearrangements and BRAF mutation, as previously reported (10 –12). Moloney Murine Leukemia Virus-RT kit (SUPERSCPIPT; Life Technology, Grand Island, NY) was used for complementary DNA synthesis, according to the manufacturer's protocols. The PCR was carried out with the thermal cycler PE480 (Perkin-Elmer Corp., Norwalk, CT). The resultant PCR products were then separated and purified, followed by DNA sequencing analysis using the OmniBase DNA Cycle Sequencing Kit (Promega Corp., Madison, WI).
Study design
This was an open-label, single-institution study of oral sorafenib in patients with RAI-refractory PTC with pulmonary metastases. Sorafenib was administered at a dose of 200 mg orally twice a day. A cycle was defined as 4 weeks. Screening evaluations, including medical history, demography, review of prior treatment, physical examination, and laboratory evaluations, were completed within 1 week before the start of administration of the drug. Serum TSH, Tg, and antithyroglobulin antibody (TgAb) levels were measured using a chemiluminescent immunoassay system (Immulite; Diagnostic Products Corp, Los Angeles, CA).
After beginning treatment, patients were observed at 4-week intervals. At each visit, a history and physical examination were performed, and a complete blood count (CBC), chemistry panel, TSH, Tg, and TgAb were tested. Patients were assessed for new symptoms, compliance with study medications (pill count), and concomitant medications. Response was assessed radiographically at 12-week intervals.
Study end points
The study end points, objective partial response (PR) rate and stable disease (SD), were measured based on the findings on CT using Response Evaluation Criteria in Solid Tumors (RECIST), which were confirmed by a study-designated radiologist (Y.S.) from Shanghai Chest Hospital. Additional end points included progression-free survival (PFS; based on RECIST), clinical progression, or death. Adverse events were assessed at each visit with an interval of a treatment cycle (4 weeks) by using Common Terminology Criteria for Adverse Events (version 3.0).
Statistical analysis
Three months after the last patient started treatment, statistical analysis was performed. Estimates of PFS (defined as time from starting study drug to progression or death, whichever occurred first) with associated 95% confidence interval were obtained using the Kaplan–Meier method, which was realized using SPSS version 11.0.
Results
Patients
Between February 2007 and May 2008, a total of 143 PTC patients with pulmonary metastases after total or nearly total thyroidectomy were treated with radioiodine in our department. Thirty two (22%) of 143 patients were found to be radioiodine refractory. Nine (28%) consecutive patients with PTC (7 men, 2 women; age range, 33–76 years; mean age, 57 years), who were considered to have progressive pulmonary metastases resistant to radioiodine treatment, were enrolled in the study. None of them had received chemotherapy or other kinase inhibitors prior to the sorafenib treatment.
Table 1 summarizes the baseline data obtained within 1 week prior to the beginning of sorafenib treatment for all the patients entered into this study. Their body weights ranged from 53 to 81 kg, with an average of 64 kg. The average serum Tg, TgAb, and TSH levels were 6970 ng/mL, 54.7 IU/mL, and 0.05 mIU/L, respectively. Gene screening revealed RET/PTC1 rearrangement in one patient, RET/PTC2 rearrangement in one patient, and BRAF mutation in three patients.
Tg, thyroglobulin; TgAb, thyroglobulin antibody; TSH, thyrotropin.
Efficacy
Patient response to sorafenib at the low dose of 200 mg twice daily was assessed using RECIST at 3 months after the last patient started treatment. The objective PR rate (defined as decrease in sum of longest diameter measurements ≥30% by RECIST) for the patients on the study was 33% (3/9). The SD rate (defined as change in sum of longest diameter measurement between −30% and +20% by RECIST) was 44% (4/9). Two patients (22%) showed disease progression (defined as increase in sum of longest diameter measurements ≥20% by RECIST), and one of them died at 4 months after beginning the treatment. Figure 1 shows the Kaplan–Meier curve for all the nine patients; the mean PFS was 42 weeks (95% confidence interval, 29.5 to 53.9). No patient died before disease progression.

Kaplan–Meier estimate of progression-free survival for papillary thyroid carcinoma patients with radioiodine-resistant pulmonary metastases on study. Mean progression-free survival was 42 weeks.
One patient (patient 4), who was given sorafenib at a relatively early stage when the pulmonary lesions were described as “micro-nodules scattered throughout the lungs” by CT scan and the Tg level was 30.3 ng/mL, showed a favorable PR to the treatment within 16 weeks. When the fourth treatment cycle ended, the serum Tg level declined steadily to 0.9 ng/mL. Also, chest CT revealed a dramatic improvement, compared with that obtained within 1 week before the initiation of the treatment (Fig. 2).
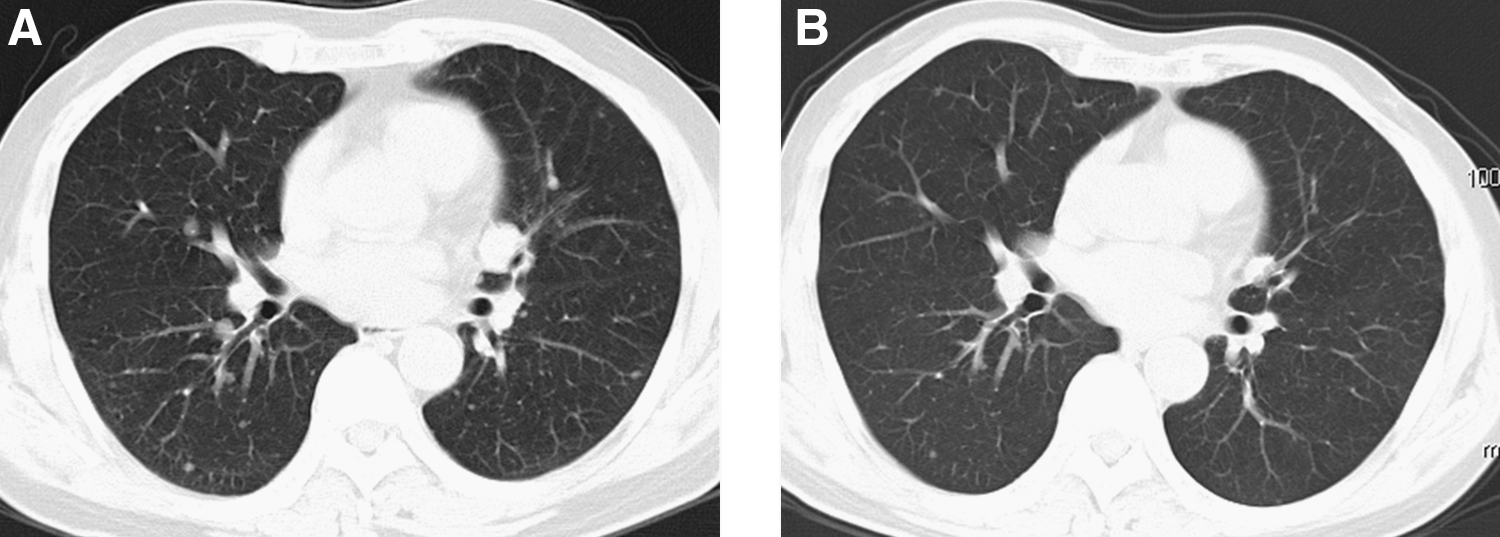
Computed tomography (CT) scan of the chest shows micronodules scattered throughout the lungs within 1 week before the initiation of sorafenib treatment, when serum thyroglobulin level was 30.3 ng/mL
The serum Tg level showed a marked and rapid decline within 4 weeks of the start of treatment and then continued to decrease in the following 8 weeks. There was a mean decrease of 60% within 12 weeks of starting treatment (Fig. 3). For patients with PR, this continuous antitumor activity was also demonstrated by radiographic findings (Fig. 4, patient 1). The average baseline and on-study TgAb levels for all patients were not elevated.
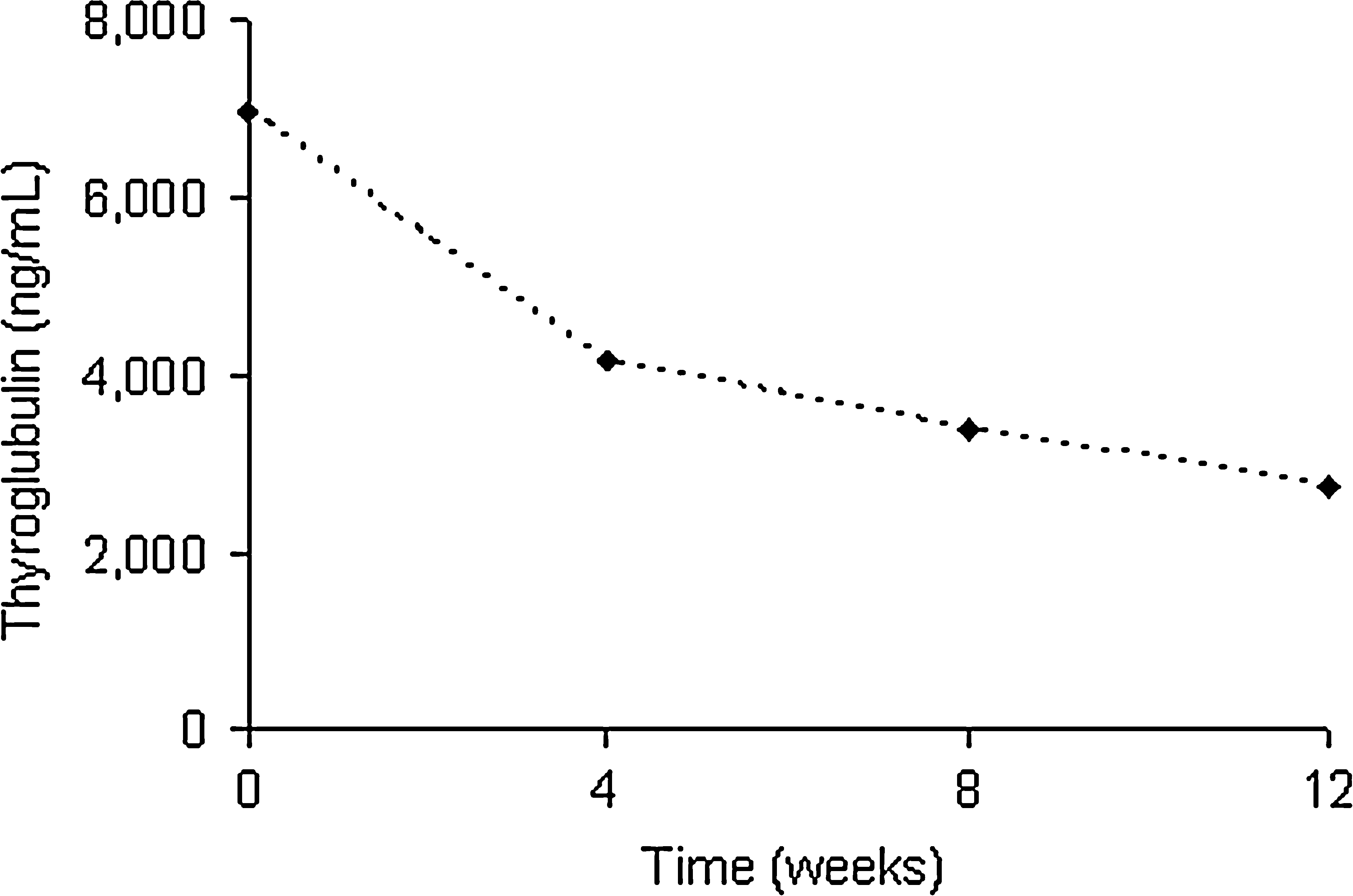
Serum thyroglobulin level shows a marked response within 4 weeks and then continues to decrease in the following 8 weeks, with a mean decrease of 60% within three cycles of treatment (n = 9).
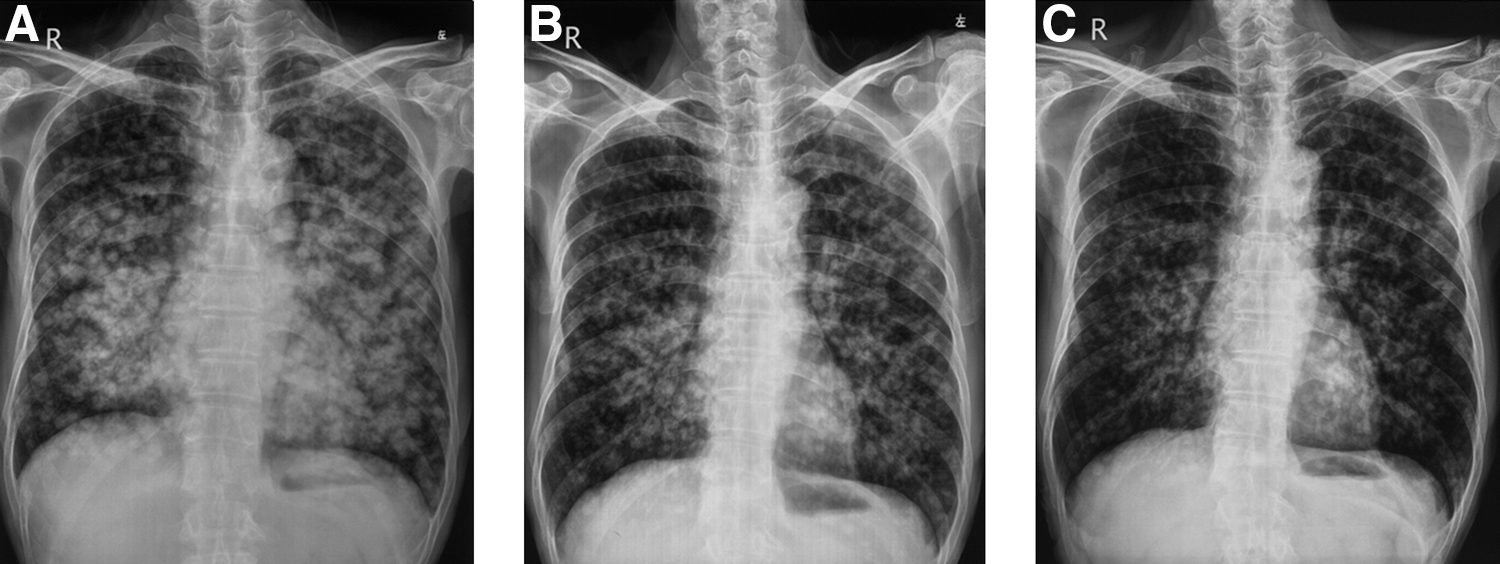
Radiographic examinations of a 62-year-old man (patient 1) show continuous antitumor activity of sorafenib treatment
Adverse events
The prevalences of rash, hand–foot skin reaction, and alopecia were 44%, 56%, and 100%, respectively. Fatigue, weight loss, and musculoskeletal pain occurred in 67%, 44%, and 22%, respectively, of the nine patients. Four patients (44%) had diarrhea. Two patients (22%) were noted to have hypertension during the treatment course and they were given antihypertensive agents. All the treatment-related adverse events were classified as grade 1 or 2 and none of the patients discontinued treatment because of treatment-related adverse events. No dose adjustments for toxicity were required. Baseline and during-study liver and kidney function tests were normal and there were no increased or decreased thyroid hormone requirements.
Discussion
The incidence rates of all sizes of DTCs increased in both men and women in the United States between 1988 and 2005. This was thought to be due to increased diagnostic scrutiny and changing environmental influences, perhaps impacting molecular pathways (13). To date, surgery plus RAI therapy has remained the standard treatment for early and locally advanced differentiated thyroid cancer. Radioiodine continues to be the initial treatment for distant metastatic disease and can produce 5-year overall survival rates of about 50% (14). However, in those with iodine-resistant disease, the therapeutic effect of RIA is poor, and therefore, this treatment is not recommended for this group of patients. Over the past few years, an increase in cell pathway-targeting agents has been greeted with enthusiasm by oncologists treating thyroid cancer (15).
In a review of four phase I trials of sorafenib in 173 patients with advanced refractory solid tumors, on testing varying doses and administration schedules, the optimal therapeutic dose was found to be 400 mg twice daily (16). However, no thyroid cancer patients were studied. Subsequently, two phase II study trials were performed in patients with metastatic and advanced thyroid cancer by using a dose of 400 mg orally twice a day (17,18). Both phase II studies showed sorafenib-relevant antitumor activity and supported further investigation of this agent in thyroid cancer patients. However, it should be noted that dose reductions were required in about half of the patients because of severe adverse events. Recently, Waguespack et al. described an adolescent with progressive PTC and RIA-resistant lung metastases who was successfully treated with low doses of sorafenib (19). In this study, a dramatic improvement was achieved after the first course, which was initiated at a starting dose of 200 mg twice daily and decreased to 200 mg daily because of side effects. Notably, the second treatment course of sorafenib 200 mg every other day was equally successful in achieving a clinical response.
Encouraged by these results, we designed this study to explore response to sorafenib at this low dose, 200 mg twice daily, in a group of patients. We found a clinical benefit (PR + SD) of 77%, which is comparable to those reported by the above two phase II trials. Therefore, it seems that a dose of 200 mg twice daily is a feasible approach in Chinese patients with RAI-refractory lung metastases from PTC. A mean PFS of 42 weeks is relatively shorter than a median PFS of 79 weeks and 15 months reported by the above two phase II trials (17,18). However, in the Eastern Cooperative Oncology Group trial of doxorubicin-containing regimens, PFS for patients with metastatic RAI-nonavid DTC was estimated at only 2 months (20). Thus, the PFS of 42 weeks noted with sorafenib in the present study is a considerable improvement in outcome.
Serum Tg, a key tumor marker for monitoring DTC, decreased substantially in patients receiving sorafenib at the low dose employed in our study. Tg measurements are interfered by TgAb, but our study patient was TgAb negative. The precipitous decrease in serum Tg in our study suggests a definitive therapeutic effect, at least in patients with PR.
During the past two decades, there have been significant advances in our understanding of the molecular events associated with thyroid cancer. An important candidate gene that has been extensively studied is the RET proto-oncogene (21). The oncogenic rearrangements of RET have been identified in PTC in different populations (22 –26). Moreover, elevated serum VEGF levels have been found and inhibition of VEGFR signaling has been shown to inhibit the growth of thyroid tumors in xenograft models, thereby providing a strong rational for targeting VEGFR in this disease (27,28). More recently, more data indicate that VEGFR contributes to RET kinase activation, signaling, and growth stimulation and may therefore be an attractive therapeutic target in RET-induced neoplasms (29). We found that RET/PTC rearrangements could be detected in 22% (2/9) of the enrolled PTC patients, who had a good response to sorafenib in our low-dose protocol. One patient who attained a PR was given sorafenib at a dose of 200 mg twice daily when the maximum tumor size was <1 cm (Fig. 1), indicating that such therapy may induce a better response if initiated at a relatively early stage. In this case, although an objective tumor response could not be determined by RECIST because of the micronodular nature of lesions, the patient could be considered to attain a PR in our opinion. The optimal criteria for clinical trial enrollment should be reconsidered in patients with diffuse micronodular disease, who are likely to achieve great benefit from participation in this treatment.
BRAF plays a key role in the mitogen-activated protein kinase signaling pathway, and an acidic substitution at a single amino acid residue, V600E, occurs frequently in PTC. BRAF V600E has been found in 29%–69% of patients and has been associated with aggressive features including extrathyroidal extension and advanced stage (30). Also, RAS mutation and RET/PTC rearrangement associated with some thyroid cancers also result in aberrant signaling through BRAF, making RAF signaling a logical target in thyroid carcinoma. In our study, the BRAF mutation was found in 33% patients, and there was no overlap between RET/PTC rearrangement and BRAF mutation in any of the tumors. Although most of the patients achieved a favorable response in our study, two patients who had the BRAF mutation showed disease progression and one of them died during treatment, indicating that the therapeutic effect of sorafenib (200 mg, bid) is poor on them. This can be partially explained by the fact that PTC cells carrying a BRAF mutation are more resistant to sorafenib than PTC cells carrying RET/PTC rearrangement (31,32). This can also be explained partially by a novel mechanism that the BRAF V600E oncogene induces transforming growth factor beta secretion leading to sodium iodide symporter repression and increased malignancy in thyroid carcinoma (33).
It has been reported by other studies that sorafenib at a dose of 400 mg twice daily is fairly well tolerated. Dose reductions, however, are necessary to improve tolerance in about half of patients. A few patients had to discontinue treatment as a result of adverse events (17,18). In our study, although the adverse events were consistent with those of other sorafenib trials, their severity was relatively mild. Hepatic and nephric toxicities were not found. None of the patients discontinued treatment as a result of treatment-related adverse events. No dose adjustment was made as needed for toxicity.
A beneficial effect of TSH suppression resulting from oral administration of thyroxine (LT4) has been supported by many studies in patients with persistent disease at National Thyroid Cancer Treatment Cooperation Study Group (NTCTCSG) stages III and IV. The doses of LT4 usually range between 2 and 2.5 μg/kg daily and should be adjusted precisely and individually, so that the serum TSH could be maintained below 0.1 mU/L. In our study, although 44% of patients experienced weight loss, it was relatively mild and adjustment of their LT4 dose was not necessary. This is not consistent with the report by Gupta-Abramson et al. (17), but consistent with the findings by Kloos et al. (18).
Conclusion
Sorafenib at a dose of 200 mg twice daily has a therapeutic effect and is reasonably well tolerated in Chinese patients with radioiodine-refractory pulmonary metastases from PTC. Its overall clinical benefit rate is 77%, with a mean PFS of 42 weeks and an acceptable safety. Prospective controlled randomized studies with more patients and longer observation times are greatly needed.
Footnotes
Acknowledgments
This study was sponsored by the National Natural Science Foundation of China (30700187), Shanghai Rising-Star Program (08QA14040), and the Public Health Bureau of Shanghai Municipality (2006Y34).
Disclosure Statement
The authors declare that no competing financial interests exist.