
Abstract
Background:
Temporary remission of primary hyperparathyroidism (PHPT) following fine-needle aspiration (FNA)–induced hemorrhage of a parathyroid adenoma is extremely rare. The purpose of this report was to illustrate that parathyroid adenomas can masquerade as thyroid nodules and that these patients must be monitored closely following remission as their hyperparathyroidism may recur.
Patient Findings:
This report describes a patient who presented with a neck mass and was incidentally found to have PHPT. Ultrasound (US) evaluation revealed a lesion that was diagnosed as a thyroid nodule. After a nondiagnostic FNA, she developed a large neck hematoma and her PHPT went into remission. Soon thereafter, her hyperparathyroidism recurred, and she underwent parathyroidectomy and thyroid lobectomy, which confirmed a large parathyroid adenoma.
Summary:
This report illustrates that remission of PHPT can occur because of FNA-induced hemorrhage leading to autoinfarction of a parathyroid adenoma. Following autoinfarction, the patient's parathyroid hormone and calcium levels must be monitored closely as the remission of PHPT may be temporary. Further, although US is a fast, inexpensive, often reliable modality for diagnosing neck masses, it does not always accurately identify parathyroid adenomas.
Conclusion:
Clinicians must be cognizant of the possibility that parathyroid adenomas can masquerade as thyroid nodules on US, especially as most patients with parathyroid adenomas are asymptomatic at presentation.
Introduction
The following report is that of a patient who presented with a neck mass and was incidentally found to have PHPT. US evaluation revealed a lesion that was diagnosed as a thyroid nodule and the subsequent FNA was nondiagnostic. Following the FNA, she developed a large neck hematoma and her PHPT went into remission. Approximately 2 weeks later, her hyperparathyroidism gradually recurred, and she underwent parathyroidectomy and thyroid lobectomy, which confirmed a large parathyroid adenoma.
Patient
The patient was a 63-year-old woman who presented to an outpatient clinic with a new, palpable, neck mass. On presentation, routine blood work revealed a parathyroid hormone (PTH) level of 247 pg/mL (normal, 10–65 pg/mL) and a calcium level of 12.4 mg/dL (normal, 8.4–10.2 mg/dL). Table 1 illustrates all PTH and calcium levels recorded for this patient. US evaluation revealed a 3.9-cm left neck mass, identified as a “thyroid nodule” per the outside clinic report. There were no details regarding the echogenicity or cystic nature of the nodule. The patient underwent US-guided FNA. Five passes were made into the mass with a 20-gauge needle, and two cytological specimens were sent for analysis. The slides were reviewed by the cytology department at an outside hospital. The first sample revealed a cluster of oncocytic cells, consistent with a Hurthle cell lesion; the second sample was unsatisfactory because of the scant cellularity. Following the procedure, the patient gradually developed worsening neck pain and swelling, accompanied by difficulty swallowing liquids, a choking sensation, and a change in her voice. Four days after the FNA, she presented to an outside emergency department, where plain films (Fig. 1A, B) revealed a large mass in the left neck with tracheal deviation anteriorly and to the right, consistent with a hematoma. She was subsequently transferred to our facility, where a computed tomography (CT) scan with contrast enhancement was performed to characterize the hematoma (Fig. 2A, B).
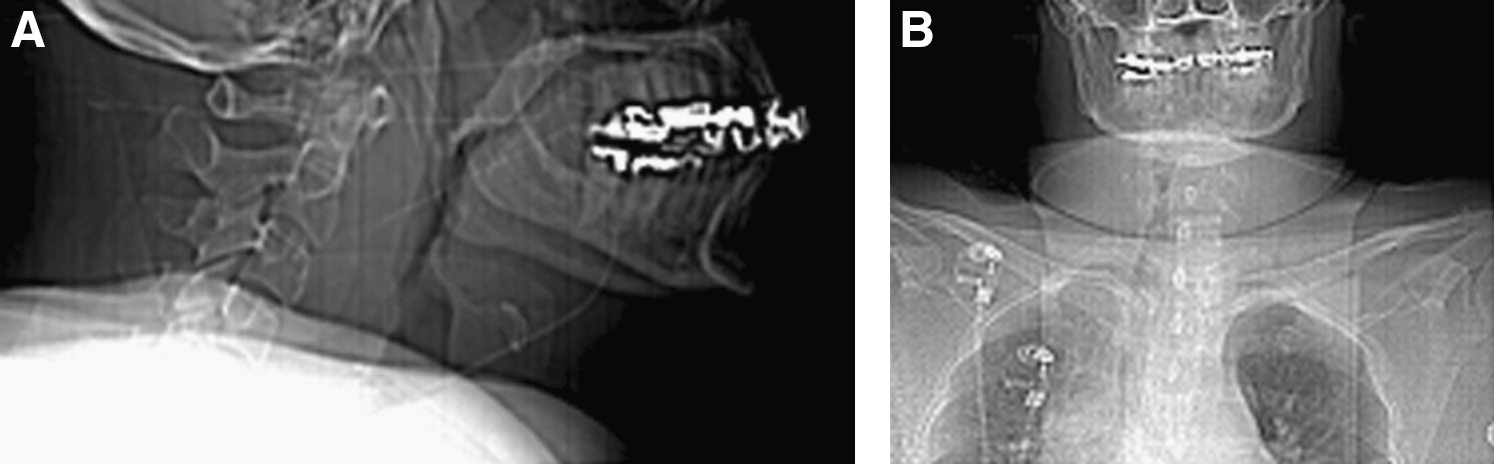
Lateral
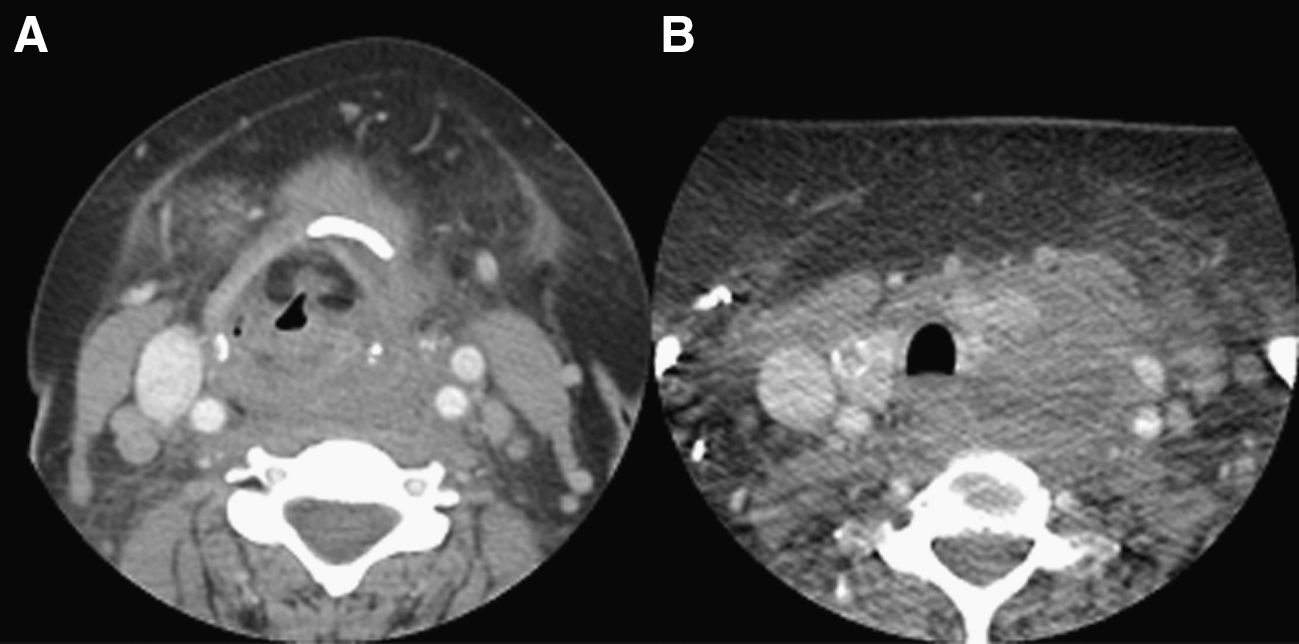
Axial, contrast-enhanced computed tomography scan obtained at 1 week following fine-needle aspiration of a left thyroid mass in a patient with hyperparathyroidism. Image reveals a 4-cm mass in the left neck causing tracheal deviation rightward and anteriorly at level of hyoid bone
PTH, parathyroid hormone; N, normal reference range; FNA, fine-needle aspiration.
The CT scan showed a 4-cm hematoma in the left neck between the thyroid and carotid sheath, extending from the level of the hyoid bone to the thoracic inlet. The larynx and trachea were displaced anteriorly and rightward (Fig. 2A, B), although her airway remained patent. Laboratory testing in the emergency department at 4 days after the FNA was performed revealed a PTH level of 22 pg/mL (normal, 10–65 pg/mL) and a calcium level of 10.4 mg/dL (normal, 8.4–10.2 mg/dL). She denied taking blood thinners at the time, such as warfarin, clopidogrel, aspirin, or nonsteroidal anti-inflammatory medications, and her platelet count was 334,000 cells/L. She was admitted to the otolaryngology service and the hematoma was managed conservatively with a short course of steroids and close monitoring. On hospital day 3, she was discharged home in stable condition.
At her 1-week follow-up appointment, blood work revealed a PTH level of 71 pg/mL (normal, 10–65 pg/mL) and a calcium level of 9.2 mg/dL (normal, 8.4–10.2 mg/dL). Because of the rising PTH level, she underwent a parathyroid sestamibi scan, which revealed faint uptake in the left posterior thyroid region suspicious for a parathyroid adenoma versus inflammation from the resolving hematoma. Because the sestamibi scan and her rising PTH were consistent with a parathyroid adenoma, she underwent a left parathyroidectomy and left thyroid lobectomy approximately 1 month later. Intraoperatively, her PTH level was 122 pg/mL (normal, 10–65 pg/mL). The left thyroid lobe was excised along with a large accessory nodule on the medial aspect of the lobe; specimens were sent for pathology. The PTH dropped from 122 to 31 pg/mL within 15 minutes of the excision. The left superior laryngeal and recurrent laryngeal nerves were identified and preserved, and their integrity was verified by a nerve stimulator. A drain was placed in the wound and the skin was closed. Her postoperative course was uneventful.
The final pathology report revealed an enlarged and hypercellular parathyroid adenoma, weighing 2100 mg and measuring 2.0 × 1.5 × 0.8 cm in size. The parathyroid adenoma had a focus of inflammation, cystic change, fibrosis, and hemosiderin deposition consistent with a prior biopsy site. The left thyroid lobe weighed 10.3 g, was negative for Hurthle cell lesion, and was notable for two benign nodules. There was also a focus of papillary thyroid microcarcinoma, measuring 0.1 cm in greatest dimension. She was followed up closely postoperatively with thyroid US, given the small size of the occult papillary carcinoma. Of note, the FNA sample was retrospectively reviewed at our institution, revealing sheets and acini of oxyphil cells with small round hyperchromatic nuclei and abundant granular eosinophilic cytoplasm. The immunohistochemistry was positive for PTH and negative for thyroglobulin and calcitonin. This cytomorphology and immunohistochemical profile was felt to be compatible with a parathyroid gland aspirate, although thyroid Hurthle cell lesion could not be completely excluded. Therefore, the parathyroid adenoma removed in surgery was thought to represent the mass that was biopsied by US-guided FNA at the outside clinic.
Discussion
Remission of PHPT due to FNA-induced hemorrhage of a parathyroid adenoma is a rare event that, to the best of our knowledge, has not been documented in the literature. Our patient went into remission of PHPT given that her PTH and calcium dropped from 247 to 22 pg/mL and 12.4 to 9.0 mg/dL, respectively, following the FNA (Table 1). This sudden drop in PTH and calcium along with the neck hematoma suggests that the FNA-induced hemorrhage led to remission of her PHPT. Interestingly, the PTH level gradually began to rise at 1 week after the FNA, demonstrating that the adenoma was temporarily affected.
Unlike remission of PHPT from FNA biopsy, spontaneous remission has been well documented (5 –7) and classified into three categories by Nylen et al.: autoinfarction or necrosis of the adenoma without hemorrhage, acute intracapsular hemorrhage, and acute extracapsular hemorrhage (7). In a meta-analysis by Wootten and Orzeck (6), 50 cases of autoparathyroidectomy were analyzed with respect to this classification. These investigators found that the prominent clinical signs of acute extracapsular hemorrhage were ecchymosis, hematoma, and hoarseness; prominent signs and symptoms of both autoinfarction and acute intracapsular hemorrhage included neck swelling and neck pain. Based on this meta-analysis, our patients' clinical scenario was consistent with an acute extracapsular hemorrhage. However, unlike our patient's case, these classifications were based upon spontaneous, or nontraumatic, remission of PHPT. It is unknown how FNA-induced remission affects outcome in these patients or the likelihood of recurrence of PHPT.
Several reports in the literature have described the recurrence of PHPT after spontaneous autoinfarction or hemorrhage of the parathyroid adenoma (10 –12). The patients in these three reports developed recurrence after 4–8 months postremission, diagnosed by PTH levels above the upper limit of normal. The patient in our case report developed recurrence at approximately 2 weeks following the FNA-induced hemorrhage, with a PTH level of 71 pg/mL (upper limit of normal, 65 pg/mL). Over the next 6 weeks, her PTH level rose to a peak of 122 pg/mL on the day of her parathyroidectomy and thyroid lobectomy. Given the short time span of her remission, it is plausible that the FNA-induced extracapsular hemorrhage/hematoma compressed the vascular supply to the tumor, causing a temporary ischemia, which led to the sudden drop in PTH and calcium levels. Resolution of the hematoma likely allowed for revascularization of the adenoma, demonstrated by quickly rising PTH levels at approximately 1 week following the FNA. Therefore, it is recommended that clinicians closely monitor these patients after spontaneous or traumatic autoinfarction or hemorrhage of the parathyroid gland, given the possibility of PHPT recurrence.
Given that the parathyroid glands are fixed to the posterior surface of the thyroid gland, it is difficult to distinguish between a mass of parathyroid versus thyroid origin by US alone. The sensitivity of US in detecting parathyroid lesions or ectopic parathyroid glands is variable, ranging from 60% to 85% (13 –16). Sestamibi scans are a preferred method for diagnosing and locating parathyroid adenomas, with an 82%–88% sensitivity in localizing adenomas of ectopic and normal locations among patients with PHPT (17,18). As illustrated in our case report, the sestamibi scan results were consistent with a parathyroid adenoma, localizing it as adjacent to the left thyroid lobe. Although the sestamibi scan result was complicated by the resolving hematoma in our patient, it was consistent with a parathyroid adenoma in light of her rising PTH and calcium levels.
Rarely, FNA biopsy without hemorrhage or hematoma causes remission of PHPT. Ing and Pelliteri (19) documented a case in which the FNA biopsy of an intrathyroidal parathyroid cyst led to subsequent remission of PHPT for at least 16 months of post-FNA follow-up. These authors posited that the FNA biopsy caused autoinfarction of the parathyroid gland along with aspiration of the cyst fluid, leading to normal serum calcium levels. Our case report is distinct in that the FNA led to hemorrhage around the parathyroid gland, and the remission of our patient's PHPT was more likely due to temporary ischemia than aspiration of tumor cells.
Although FNA biopsies are safe, outpatient procedures, they are occasionally complicated by hematoma formation. FNA-induced hemorrhage or hematoma is typically self-limited and rarely requires hospital admission. There are three reported cases of FNA-related hematomas causing airway obstruction and requiring surgical exploration within hours of the FNA procedure (20 –22). Although our patient did not require surgical intervention, she had to be monitored closely for several days and treated with steroids. Aside from hypertension, she did not have other potential risk factors for hematoma or hemorrhage following FNA, such as an underlying coagulopathy, renal disease, or the use of blood thinners, such as warfarin, clopidogrel, aspirin, or nonsteroidal anti-inflammatory medications.
This case report illustrates several important points. First, remission of PHPT can occur because of FNA-induced hemorrhage leading to autoinfarction of the adenoma. Second, PHPT can recur following autoinfarction. Therefore, the patient's PTH and calcium levels must be monitored closely after autoinfarction as the remission of PHPT may be temporary. Last, although US is a fast, inexpensive, often reliable modality for diagnosing neck masses, it does not always accurately identify parathyroid adenomas. Clinicians must be cognizant of the possibility that parathyroid adenomas can masquerade as thyroid nodules on US, especially as most patients with parathyroid adenomas are asymptomatic at presentation.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.