
Abstract
Background:
Hyalinizing trabecular tumors of the thyroid (HTT) is a rare entity. Most behave as benign neoplasms, but their cytological features are challenging and can be similar to those of papillary thyroid carcinoma (PTC). The aim of this study was to compare the ultrasonography (US) readings of HTT with the cytology and frozen section readings.
Methods:
We retrospectively analyzed the US and cytology features in 10 patients (mean age, 47.5 years, range 26–81; M:F, 1:9) seen between March 2006 and November 2009 who had a histopathological diagnosis of HTT. The US findings were categorized according to the size, shape, margin, echogenicity, echotexture, presence of hypoechoic halo, and microcalcifications. Preoperative fine-needle aspiration cytology, frozen section results, and surgical treatment were reviewed. US features of HTT were compared with those of other tumors including follicular adenomas, follicular variant of PTCs, and conventional PTC.
Results:
Out of the 10 patients in our series, 7 underwent total thyroidectomy, and 3 had lobectomy. The sizes of the HTTs ranged from 0.6 to 4.2 cm (mean, 1.77 cm). The most common US features were solid texture (10/10), oval to round shape (10/10), a well-defined aspect (10/10), hypoechoic character (8/10), heterogeneous character (7/10), the presence of a hypoechoic halo (8/10), and no microcalcifications (10/10). The US diagnosis was indeterminate in all but one case and that was read as a benign lesion. As far as the shape and margin US features were concerned, HTT was considered to be most similar to follicular adenomas and follicular variant of PTC, but not to classical PTC. The cytology reading was PTC in 6 of 10 cases, suspicious for PTC in 2, and a HTT versus PTC in 2. The histological diagnosis of frozen sections, when performed, was PTC in three, HTT in three, medullary thyroid carcinoma in two, and deferred in one.
Conclusion:
HTT often appears similar to follicular neoplasm on US, but it can be misjudged on cytology as PTC, even in frozen sections. HTT should be included in the list of discordant US—cytology readings of thyroid tumors. This rare tumor might be suspected more often preoperatively by careful attention to cytology in the context of the US reading.
Introduction
Materials and Methods
Patients
The institutional review board approved this retrospective study, and the need for informed consent was waived. The medical record database at our institution was searched for patients with a diagnosis of HTT between March 2006 and November 2009. During this period, 5111 patients at our institution underwent surgery for thyroid lesions. Among them, 4651 patients (91%) were diagnosed after thyroid surgery as PTC, and 10 (0.2%) patients with nodules were diagnosed as HTT (1 male and 9 female; age range, 26–81 years; mean age, 47.5 years). To compare US findings of HTT with other groups, 30 consecutive patients with 30 follicular adenomas (FA), 30 consecutive patients with 30 follicular variant of PTCs (FVPTCs), and 30 consecutive patients with 30 conventional PTCs were added to the study. These 90 patients were diagnosed at our institution after lobectomy or total thyroidectomy over 4, 22, and 1 month periods, respectively. The sonographic findings of thyroid nodules were retrospectively reviewed, and clinical information was obtained from the medical records.
Ultrasonography
US was performed as a baseline study before surgery. Experienced radiologists scanned the thyroid with HDI 5000, or iU22 scanners (Philips Medical Systems, Bothell, WA) equipped with a commercially available 7- to 12-MHz linear transducer. Retrospective review of the US images was performed by two radiologists (J.H.S. and B.K.H.) with 6 and 11 years of experience in thyroid imaging. They reached consensus readings and did not know the histopathological readings. Their US readings included information on the shape (ovoid to round, taller-than-wide, or irregular), margin (circumscribed, spiculated or microlobulated, or ill-defined), echogenicity (markedly hypoechoic, hypoechoic, or isoechoic), echotexure (homogeneous or heterogeneous), presence of hypoechoic halo (thin rim of decreased echogenicity surrounding the neoplasm), calcifications, or cystic change of nodules. The size of nodules was that recorded in the initial US report which was a part of their clinical care. Color Doppler imaging was not routinely used.
The radiologists made a final diagnosis for each nodule as being malignant, indeterminate, or benign based on widely accepted US criteria for a malignancy. Malignant US characteristics were a taller-than-wide shape, a spiculated margin, marked hypoechogenicity, and the presence of microcalcifications or macrocalcification (7). The lesion was considered a malignancy if at least one malignant finding was present. The inclusion criteria for a benign nodule were cyst, predominantly cystic nodule (≥50% cystic), and a spongiform (or honeycomb) nodule. US “indeterminate” nodules were defined as those having neither benign nor malignant features.
Cytopathology
All 10 patients with HTT had undergone US-guided fine-needle aspiration biopsy (FNA) of their thyroid nodule. FNAs were performed using 23-gauge needles with or without local anesthesia. The aspirates were expressed onto frosted-end glass slides, then immediately fixed in 95% alcohol, and stained with hematoxylin and eosin and Papanicolaou stain. Nine of the 10 patients with HTT had a frozen section of thyroid tissue during their thyroid surgery. The cytology, pathology, and final histopathology readings used for the study were those that were a part of their clinical care.
Statistical analysis
The frequencies of US features were compared for HTTs and other tumors (FA, FVPTC, and PTC) using Fisher's exact test with permutation or Dunnett's test for the comparison of multiple groups to the HTT group. A value of p < 0.05 was considered statistically significant. Analyses were carried out using the SPSS version 17 software for Windows (SPSS Inc., Chicago, IL).
Results
Clinical and imaging findings are summarized in Tables 1 and 2. Three patients with HTT presented with hoarseness, palpable nodule, or neck swelling. The other seven nodules were detected during screening US in five patients with asymptomatic disease and two patients with Graves' disease, respectively. The size of the HTT nodules varied from 0.6 to 4.2 cm (mean, 1.77 cm). All 10 nodules were solid, oval to round, well defined, and did not have calcifications by US (Fig. 1). Eight of the 10 were hypoechoic and had a hypoechoic halo, and seven were heterogeneous. The other two and three nodules were isoechoic and homogeneous, respectively (Fig. 2). None of the 10 HTT nodules were given a diagnosis of malignancy by the US reading. Rather, 9 were considered indeterminate, and 1 was considered benign (Fig. 3). Color Doppler US was available in one patient and showed nonspecific hypervascularity within the tumor.

Case 4. Hyalinizing trabecular tumor in a 32-year-old woman. Transverse
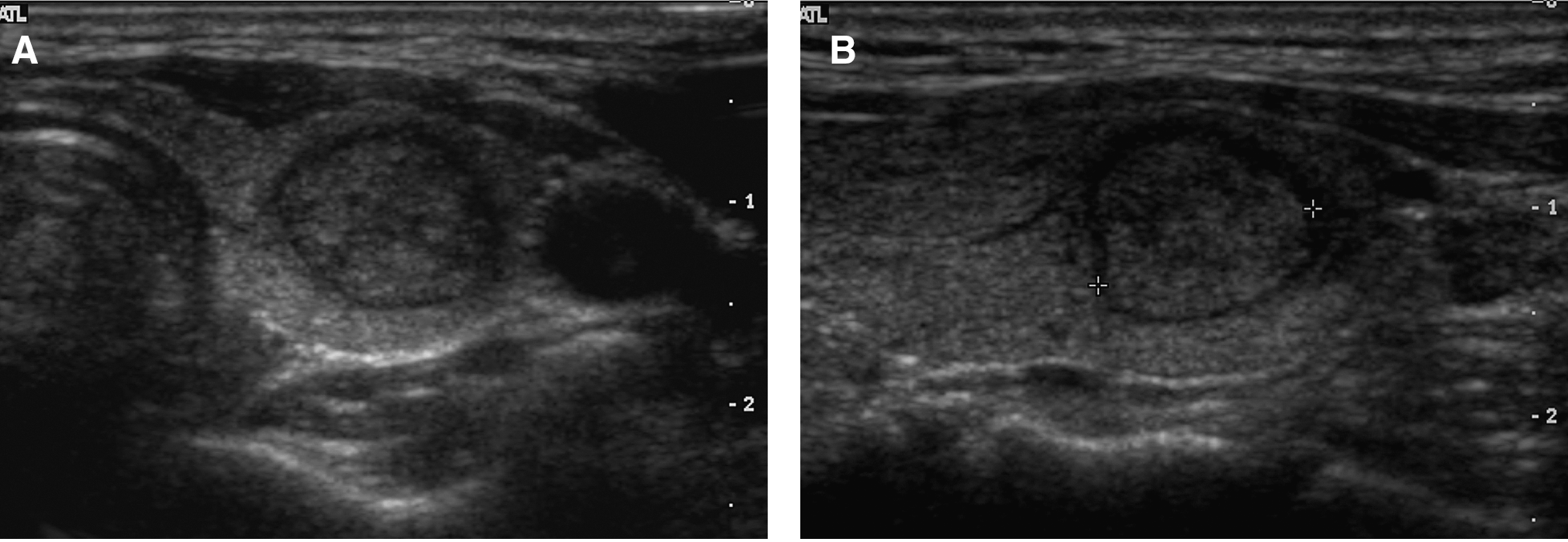
Case 5. Hyalinizing trabecular tumor in a 52-year-old woman. Transverse

Case 10. Hyalinizing trabecular tumor in a 52-year-old woman showing a lobulated shape. Transverse
CLT, chronic lymphocytic thyroiditis; CND, central neck dissection; FNAB, fine needle aspiration biopsy; HTT, hyalinizing trabecular tumor; LL, left lobectomy; MTC, medullary thyroid carcinoma; NH, nodular hyperplasia; PTC, papillary thyroid carcinoma; RL, right lobectomy; TT, total thyroidectomy.
US, ultrasonography.
The comparisons of US findings among tumors classified as HTT, FA, FVPTC, and PTC are summarized in Table 3. Compared with HTT, PTC showed a more frequent taller-than-wide shape (36.7%, 11/30 vs. 0%, 0/10) (p = 0.0166) as well as spiculated margin (60.0%, 18/30 vs. 0%, 0/10) (p < 0.0001), with both differences being significant. PTC had a trend toward having marked hypoechogenicity (33.3%, 10/30 vs. 0%, 0/10) (p = 0.0899) and calcifications (33.3%, 10/30 vs. 0%, 0/10) (p = 0.0555) more frequently, but these differences between PTC and HTT were not significant. A hypoechoic halo was significantly less common in PTC (13.3%, 4/30) than HTT (80%, 8/10) (p < 0.001). The US diagnosis of malignancy was significantly more common in PTC (63.3%, 19/30) than in HTT (0%, 0/10) (p < 0.001).
Fisher's exact test with permutation.
Dunnett.
Dunnett using rank.
Fisher's exact test with permutation and Bonferroni's method.
FA, follicular adenoma; FV, follicular variant of papillary thyroid carcinoma.
In the comparison between FVPTC and HTT, the presence of calcification was significantly more common in FVPTC (50%, 15/30) than in HTT (0%, 0/10) (p < 0.01). The US features relating to shape, margin, and echogenicity that are relevant to malignancy, and the US diagnosis of malignancy itself, were similar in FVPTC and HTT (p = 0.225, 0.201, 1, and 0.424, respectively). The US findings for HTT were similar to those of FA, except in the presence of cystic change, which occurred exclusively in FA (0%, 0/10 vs. 60%, 18/30, p < 0.002).
All 10 patients with HTT underwent US-guided FNA. All aspirates were adequate for cytological examination. Cytology was read as PTC in 6 of 10 cases, suspicious for PTC in 2, and HTT versus PTC in 2. Two patients underwent US-guided FNA twice. One patient had lymphocytic thyroiditis at initial cytology and was suspicious for PTC at 2-month follow-up cytology (case 2). Another patient's initial cytology was suggestive of medullary thyroid carcinoma and had the diagnosis of HTT versus PTC when the FNA was repeated 4 years later (case 4). Four HTT nodules had studies for the BRAFV600E mutation on FNA samples, as all were negative.
Nine of the patients with HTT had frozen sections performed during thyroid surgery. The diagnosis was PTC in three, HTT in three, medullary thyroid carcinoma in two, and deferred in one. Two of the three patients in whom the frozen section diagnosis was HTT had a lobectomy, and the patient whose frozen section diagnosis was deferred had a lobectomy. The remaining seven had a total thyroidectomy with central neck dissection. No lymph node metastasis was histologically documented at the time of thyroidectomy or in the preoperative imaging. Five of 10 patients had chronic lymphocytic thyroiditis, and three had nodular hyperplasia as associated pathologies. One patient with HTT had three micro PTCs in the contralateral lobe (diameter of 0.5, 0.2, and 0.1 cm). All five patients who were followed up with thyroid US (range 7–30 months; mean period; 16.8 months) had no recurrent disease after surgery. The tumors were located in the left lobe in six and the right lobe in four.
Discussion
There are some limitations of this study, as it was retrospective and included, because of its rarity, only 10 patients. Nonetheless, to the best of our knowledge, this is the first study to compare the US findings in HTT with those of other common forms of thyroid nodules and also with the FNA cytology and frozen section findings.
By US, HTT is similar to FA and does not have findings that are considered indicative of malignancy. In contrast, by FNA cytology and frozen section, a substantial percentage of HTT nodules can be misdiagnosed as PTC.
On gross pathology, most HTTs are spheroidal, oval, or slightly irregular in shape, circumscribed or encapsulated, and firm to soft. The fresh cut surface shows a solid, slightly bulging, delicately lobulated tumor with a yellow, pink, orange, or white color (6). Our series of 10 HTTs also had these common US features in that all were of an oval-to-round and well-defined nature. They were also all solid and did not have calcifications. Most (80%) had a hypoechoic halo (80%), were hypoechoic (80%), and had a heterogeneous echotexture (70%). None were malignant nodules by US criteria. Nine were indeterminate, and one was benign.
These sonographic features in HTT are similar to the US features of the FVPTC and other follicular cell-derived lesions such as nodular hyperplasia, FA, and follicular carcinoma (7 –13). In our study, US features including shape, margin, echogenicity, presence of calcification, echotexture and hypoechoic halo, as well as US diagnosis of malignancy, were not significantly different between HTT and FA. A cystic change in a nodule was more common for FA (60%) than for HTT (0%). However, the majority of nodules with a cystic change were predominantly solid (<50% cystic), and this feature does not have an influence on the US diagnosis of malignancy. US findings for HTTs were also not significantly different compared to FVPTC, except in the presence of more frequent calcifications for FVPTC (50%) relative to HTT (0%). HTTs had a different shape and margin than PTCs, and most PTCs were read as malignant on US.
Our cytological diagnosis was PTC in most patients (80%). Features that have been reported to be suggestive of HTT in the FNA smears are a bloody background, cohesive aggregates of cells around hyaline material, and cells with abundant cytoplasm giving a low nuclear to cytoplasmic ratio (14). Since tumor cells contained the well-formed nuclear cytological features of PTC, smears of the lesions have been commonly interpreted as PTC or suggestive of that diagnosis (5,15,16). The cytological diagnosis of PTC is based on classic nuclear abnormalities, such as ground-glass chromatin, nuclear grooves, intranuclear inclusions, psammoma bodies, and pseudopapillary structures (5,17). Follicular lesions with similar US features to HTT can be discriminated from conventional PTC on the basis of set pathological criteria: increased cellularity with a small uniform follicular organization, scant or absent colloid, and follicular cells having small nuclei with regularly distributed chromatin or having enlarged nuclei with sparse or irregularly distributed chromatin (17 –21). Therefore, the diagnosis of HTT should be considered before thyroid surgery, combining the US features with cytology that is similar to a follicular neoplasm.
In our series and the literature, almost all cases of HTT have benign behavior. In our patients, there were no lymph node metastases or capsular invasions at the time of thyroidectomy in our patients. Five of our patients had follow-up US, and none had recurrent disease or metastasis after a mean of 16.8 months. In the first report of HTT, Carney et al. described 11 cases. None of these had microscopic evidence of invasion, and none recurred or developed metastases during a mean follow-up of 10 years (3). In a recent study of 119 HTTs collected over a 20-year period, 118 did not have evidence of aggressive behavior (capsular, vascular, and parenchymal invasion), local recurrence, or metastases. There was vascular and capsular invasion as well as pulmonary metastases in only one tumor (6).
HTT is frequently associated with other abnormalities in the thyroid gland, most commonly lymphocytic thyroiditis, but has also been seen with papillary and follicular neoplasms as well as multinodular goiter (4,22). We found associated thyroid pathology in 8 of our 10 patients, including chronic lymphocytic thyroiditis, nodular hyperplasia, and PTC. It has been suggested that HTT may represent a peculiar form of PTC based on its nuclear features, immunohistochemical profile, and RET/PTC arrangements (23 –25). However, no BRAF mutations, which are specific for PTC, have been reported in these tumors (26) nor did we find BRAF mutations in the four nodules tested in our series.
In conclusion, HTT often appears similar to follicular neoplasm on US, but it can be misjudged as on cytology as PTC and even in frozen sections. HTT should be included in the differential diagnosis of imaging-cytological discordance. Definitive preoperative diagnosis of HTT should be the goal of further research. Currently, its management may be improved by careful analysis of combined US and cytology findings.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.