
Abstract
Background:
Substantial controversy exists over the role of prophylactic neck dissection for patients with papillary thyroid carcinoma (PTC). We hypothesized that a therapeutic strategy of performing a routine intraoperative frozen section of the ipsilateral central lymph node (CLN) after elective ipsilateral CLN dissection (CLND) for all unilateral PTC and then performing a contralateral CLND if the frozen section is positive for malignancy would reduce morbidity compared to a therapeutic strategy of routine bilateral CLND.
Methods:
In a group of 419 patients with PTC undergoing thyroidectomy during study the period, the 203 patients who had unilateral PTC and no evidence of adenopathy on ultrasonography were prospectively enrolled in our nonrandomized study that was performed between March 2009 and February 2010. Patients underwent a total thyroidectomy if tumor size was over 1 cm or extrathyroidal was detected on ultrasonography. Patients underwent a subtotal or near-total thyroidectomy if tumor size was <1 cm and additional benign tumor existed on contralateral lobe. There were 25 patients who had a unilateral CLND with a subtotal or near-total thyroidectomy, and 178 patients who underwent a unilateral or bilateral CLND with a total thyroidectomy.
Results:
There was no difference in the rate of major complications between unilateral CLND group and bilateral CLND group. The rate of transient hypocalcemia was 31.8% in the unilateral CLND group and 45.7% in the bilateral CLND group (p = 0.084). The rate of voice change was 7.6% in the unilateral CLND group 4.3% in the bilateral CLND group (p = 0.438). The ratio of malignant to all nodes retrieved was 0.5/7.88 in the unilateral CLND group and 5.13/17.20 in the bilateral CLND group. There was 78.3% sensitivity and 100% specificity for frozen biopsy of ipsilateral CLN to predict contralateral CLN metastasis. A positive ipsilateral CLN frozen biopsy was significantly associated with contralateral CLN metastasis (p < 0.001), as was younger age (p = 0.002) and existence of extrathyroidal extension (p = 0.031), each on univariate analysis.
Conclusions:
In patients with unilateral PTC, routine ipsilateral CLND with intraoperative reading of the frozen section can be employed to assess the risk of contralateral CLN metastasis. This information should be of value in deciding whether to perform contralateral CLND or not.
Introduction
Despite the excellent overall prognosis for patients with papillary thyroid carcinoma (PTC), many of these patients will develop nodal metastases in the central neck (level VI) or lateral neck (levels II, III, and IV) at the time of presentation or during the course of follow-up. Most endocrine surgeons agree that compartment-based nodal dissection is an appropriate and effective treatment for enlarged lymph nodes (LNs) that are identified on preoperative imaging or physical examination, or during intraoperative inspection and palpation (4).
However, substantial controversy exists regarding the role of prophylactic neck dissection for patients with PTC. The central neck LNs (level VI) are located in the region bordered laterally by the carotid sheath, medially by the trachea, superiorly by the hyoid bone, and inferiorly by the suprasternal notch (5).
It is generally accepted that therapeutic neck dissection of grossly involved LN should be carried out in PTC patients. However, elective neck dissection in clinically node-negative necks remains controversial because of the lack of hard proof of its survival benefit to justify subjecting the patient to the increased rate of complications associated with the procedure (6).
In patients with PTC and high risk of central LN metastasis whose clinical preoperative evaluation failed to detect any LN involvement, an elective central lymph node dissection (CLND) may prevent loco-regional recurrence and distant metastasis, in spite of increasing morbidity.
Currently, some investigators recommend selective central neck dissection for high-risk patients (7,8), but others suggest elective bilateral or unilateral central neck dissection (9). Routine central CLND is supported by other international guidelines (10). The European Thyroid Association notes that routine central CLND may also provide useful and accurate pathologic N-staging information that may guide subsequent treatment and follow-up (11). This approach may enhance the effect of radioiodine ablation therapy by removing potentially positive nodes, may prevent central-neck recurrence, and may improve survival compared with historical controls (12,13).
Recently, Sadowski et al. reported that when routine bilateral CLND was done, only 4.7% of patients without ipsilateral CLN metastasis had a metastatic contralateral CLN (14).
We hypothesized that our therapeutic strategy, which is performing a routine intraoperative frozen section of the ipsilateral CLN after elective ipsilateral CLND for all unilateral PTC and then deciding whether to perform contralateral CLND or not, is an efficient method for reducing unnecessary contralateral CLND and its attendant morbidity.
Materials and Methods
Patients and tumor specimens
In a group of 419 patients with papillary carcinoma undergoing thyroidectomy during study period, 203 patients who had unilateral PTC and no evidence of adenopathy on ultrasonography were prospectively enrolled in our nonrandomized study between March 2009 and February 2010. Patients included in this study had clinically node-negative necks who were found to have unilateral PTC preoperatively by fine needle aspiration or intraoperatively on frozen section, and treated with total or subtotal thyroidectomy and elective unilateral CLND and then underwent contralateral CLND if the result of the frozen section of the involved-side CLN showed malignacy. Patients who underwent therapeutic neck dissection for clinically positive nodes in the lateral or central neck compartments, or who had thyroid surgery for a benign condition and were unexpectedly diagnosed with papillary carcinoma in the final pathologic result and therefore did not undergo CLND were excluded. Patients with a PTC involving the isthmus or bilateral lobes were also excluded due to the inherent difficulty in determining laterality of the central LN. Clinically characterized node-negativity was defined as the neck having no palpable cervical LNs during physical examination, or showing no suspicious metastatic LN in imaging studies such as ultrasonography and computed tomography. Consequently, a total of 203 consecutive unilateral PTC patients with clinically node-negative necks who underwent total or subtotal thyroidectomy with elective CLND were enrolled in this study (Fig. 1). Patients underwent a total thyroidectomy if tumor size was over 1 cm or extrathyroidal was detected on ultrasonography. Patients underwent a subtotal or near-total thyroidectomy if tumor size was <1 cm and additional benign tumor existed on contralateral lobe. There were 25 patients who had a unilateral CLND with a subtotal or near-total thyroidectomy and 178 patients who underwent a unilateral or bilateral CLND with a total thyroidectomy. For all patients, frozen section for elective CLND was done and all nodes sampled were examined. Then, if the result of the ipsilateral CLN frozen section was malignant or if grossly involved contralateral nodes were found intraoperatively, we performed contralateral CLND. The present study was approved by the Institutional Review Board of the Seoul St. Mary's Hospital, Catholic University of Korea.
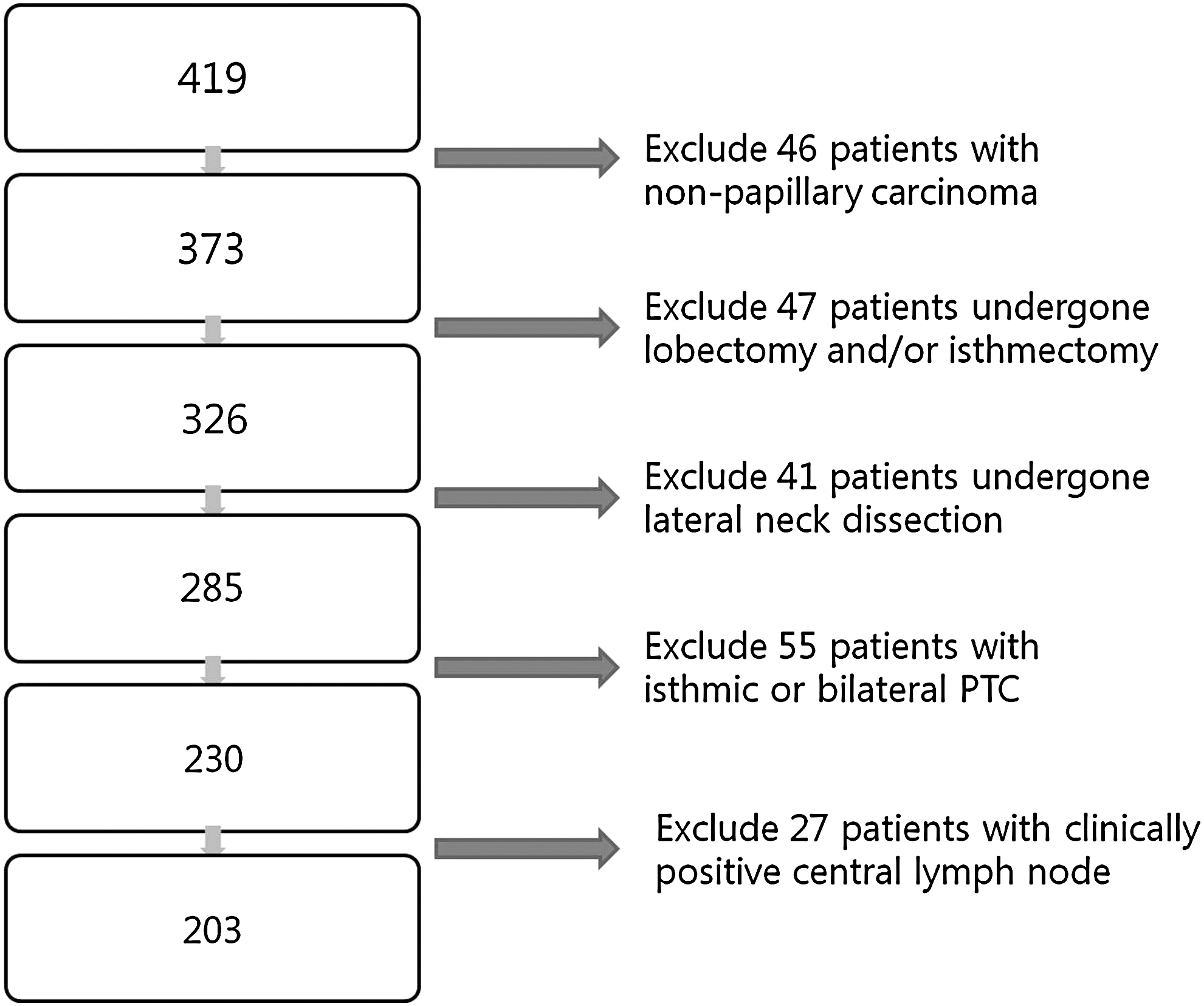
Scheme of patient selection method in this study. PTC, papillary thyroid carcinoma.
CLN dissection
CLND was extended superiorly to the hyoid bone, inferiorly to the innominate vein, laterally to the carotid sheaths, and dorsally to the prevertebral fascia. The thymus was commonly preserved by separation from the central nodes. After unilateral CLND was finished, the neck specimen was divided into two portions and labeled as follows: pretracheal and ipsilateral paratracheal. We defined the pretracheal and paratracheal region ipsilateral to the tumor location as the ipsilateral central compartment and the paratracheal region contralateral to the tumor location as the contralateral central compartment. The labeled specimens were sent to the Department of Pathology for frozen section analysis, and if the result of the frozen section of the involved-side CLN showed malignancy, we performed contralateral CLND. Particular attention was made to preserve the parathyroid glands, with parathyroid autotransplantation being carried out as required and not as a principle. All surgery for patients enrolled in the present study was done by a single experienced thyroid surgeon.
Evaluation of postoperative complications
All patients were clinically evaluated for signs and symptoms of hypocalcemia and voice change after surgery. Complications included transient hypocalcemia (defined as serum calcium <8.0 mg/dL within 24 hours of operation), permanent hypocalcemia (defined as serum calcium <8.0 with associated low parathyroid hormone level requiring both oral calcium and vitamin D administration >6 months after operation), transient hoarseness (subjective patient complaint, confirmed by clinician examination between 0 and 6 months after operation), and permanent recurrent laryngeal nerve injury (hoarseness >6 months after operation, confirmed with laryngoscopy showing ipsilateral vocal cord dysfunction).
Statistical analysis
Statistical analysis was performed using SPSS version 12 software. Univariate analyses for the relationships between central LN metastasis and clinical factors such as age, sex, and the clinicopathologic characteristics of the primary lesion were performed using the Pearson Chi-square test or Fisher exact test. We defined statistical significance based on a p-value of <0.05 (two-tailed).
Results
From March 1, 2009, to January 27, 2010, a single surgeon from our thyroid surgery practice performed 419 thyroidectomies. Of the 419 operations, after excluding patients who had non-papillary carcinoma, undergone lobectomy or lateral neck node dissection, bilateral, or isthmus cancer, 203 were unilateral clinically CLN-negative papillary carcinoma with initial operations removing the unilateral or bilateral central neck LNs (Fig. 1). The mean age of objective patients was 48.2 ± 12.12 years (range 19–76), and the male-to-female ratio was 1:3.95. The number of patients undergoing total thyroidectomy was 178 (87.7%), 22 underwent subtotal thyroidectomy 22 (10.8%), and 3 underwent near total thyroidectomy (1.5%). LN metastasis was found in 93 patients (45.8%), the average number of metastasized nodes was 3.38 (unilateral vs. bilateral; 0.5 vs. 5.13), and the average number of excised nodes was 9.99 (unilateral vs. bilateral; 7.88 vs. 17.20). The mean size of primary thyroid tumors was 0.92 cm (range, 0.1–3.7 cm).
Postoperatively, there were 71 patients (34.9%) with transient hypocalcemia, and 14 patients (6.9%) with changed voice. However, all of them recovered to a symptom-free state within 6 months. Consequently, there were no cases of permanent hypocalcemia or permanent recurrent laryngeal nerve injury.
Clinicopathologic features according to the extent of CLND
We compared data from patients in the unilateral CLND group with data from patients in the bilateral CLND group. The demographic profiles of the two groups were different, with the patients undergoing only unilateral CLND being older. Patients undergoing bilateral CLND consisted of 15 men (32.6%) and 31 women (67.4%), and the patients undergoing unilateral CLND consisted of 26 men (16.6%) and 131 women (83.4%). Capsular invasion and extrathyroidal extension were higher in the bilateral CLND group. Also, the bilateral CLND group had significantly higher T and N stages. However, no significant differences in transient hypocalcemia and voice change were noted in either group (Table 1).
CLN, central lymph node; CLND, central lymph node dissection.
Predictive analysis for frozen biopsy of CLN
All patients enrolled in the present study had an intraoperative frozen biopsy after ipsilateral CLND. Cases with a malignancy reading of the frozen biopsy were confirmed to be malignant by permanent pathologic examination, and only 18 cases with a benign result on frozen biopsy were malignant in permanent pathologic examination. Eight (44.4%) of 18 were proven to have micrometastasis. Sensitivity, specificity, and accuracy of intraoperative ipsilateral CLN frozen biopsy was 78.3%, 100%, and 91.1%, respectively. Also, the positive predictive value was 100%, and the negative predictive value was 87% (Table 2).
Clinicopathologic factors in relation to contralateral positive CLN
Contralateral CLN metastasis was significantly higher in those of younger age (<45) and those with the presence of extrathyroidal extension and result of malignancy in CLN frozen biopsy in univariate analysis (p-value was 0.002, 0.031, and <0.001, respectively). However, there were no statistically significant differences between sexes in the status of capsular invasion in the T stage (Table 3).
Discussion
There is controversy in the literature regarding the recommended extent of surgical treatment of the CLN compartment (Level VI) in PTC (7,15). Arguments for prophylactic CLND fall into several categories; it may decrease recurrence and mortality rates, improve accuracy in staging (e.g., convert Nx to N1a upstaging patients over 45 years of age to American Joint Commission on Cancer stage III from stage I), achieve low or undetectable thyroglobulin levels, facilitate radioactive iodine (RAI) treatment, and avoid reoperative surgery.
There are no randomized controlled data to support the concept that routine CLND impacts the recurrence or survival rates of DTC. Nonetheless, recent population-based studies have shown that regional LN metastasis among patients with thyroid cancer impacts mortality (16 –18). Additionally, it is becoming accepted that the completeness of surgical resection is associated with less recurrence and improved survival (19). Comprehensive central compartment node dissection may improve survival and reduce the risk of recurrence as compared with historic controls (12). In a retrospective cohort, Sywak et al. (20) showed that patients undergoing total thyroidectomy with CLND versus total thyroidectomy alone demonstrated lower postoperative thyroglobulin levels.
The major argument against prophylactic CLND is a possibly increased risk of operative complications. As stated, the overall outcomes for DTC are excellent, and there is a concern that overtreatment would lead to a higher rate of two debilitating complications of central neck operations, permanent hypoparathyroidism, and nerve injury. However, Alvarado et al. (21) compared 170 patients (group A) who had a CLND as part of their primary surgical procedure, whereas 23 patients underwent CLND as a secondary procedure. The incidence of temporary hypocalcemia (12% vs. 9%), permanent hypoparathyroidism (1.8% vs. 0%), temporary recurrent laryngeal nerve (RLN) paresis (3% vs. 4%), permanent RLN paresis (0.6% vs. 0%), and wound infection (0.6% vs. 4.3%) was comparable between groups A and B, suggesting that there is no additional morbidity when CLND is performed as a secondary procedure for patients with PTC.
In the present study, we investigated the usefulness of intraoperative frozen section toward deciding whether to perform contralateral CLND, and showed a comparable rate of major complications in bilateral CLND group (transient hypocalcemia; p-value 0.084 and voice change; p-value 0.438, Table 1).
Also, predictive analysis for frozen biopsy of ipsilateral CLN showed relatively high sensitivity (78.3%) and 100% specificity. We believe that with its 100% positive predictive value and 91.1% accuracy, the method could be clinically applied. In univariate analysis for predicting contralateral CLN metastasis, the frozen biopsy for ipsilateral CLN was highly significant (p-value <0.001).
In considering the extent of prophylactic CLND in PTC, it should be kept in mind that the impact of the central compartment recurrence differs from that of a lateral compartment recurrence. Reoperation for recurrence in the lateral compartment can be performed more easily than that for recurrence in the central compartment, where more critical structures (i.e., trachea, great vessels, etc.) are located. Therefore, since metastases in the central compartment are very common and given that surgery for recurrence in the central compartment may be a complicated procedure, prophylactic central CLND during the initial thyroid surgery (usually through the same incision) seems to be a reasonable management option (22).
Despite the fact that (in experienced hands) CLND can be performed safely, it may be associated with a potentially significant morbidity. Therefore, decreasing the extent of CLND would reduce postoperative side effects. According to recently reported data, the risk of RLN injury was not greater with bilateral CLND compared to unilateral or no CLND (p = 0.18) (14).
In patients with unilateral PTC, routine ipsilateral CLND with intraoperative reading of the frozen section can be employed to assess the risk of contralateral CLN metastasis. This information should be of value in deciding whether to perform contralateral CLND or not. So, we suggest that elective routine ipsilateral CLND with its numerous therapeutic advantages and selective contralateral CLND based on results of intraoperative frozen section in order to decrease unnecessary morbidity is a reasonable strategy for unilateral PTC.
Footnotes
Acknowledgment
This article was supported by a grant from research fund donated by Gangneung Dong-In hospital.
Disclosure Statement
The authors declare that no competing financial interests exist.