
Abstract
Background:
Radiation-induced thyroid disorders have been reported in radiotherapy of head and neck cancers. This study evaluated the radiation-induced damages to thyroid gland in patients with nasopharyngeal carcinoma (NPC).
Methods:
Forty-five patients with NPC treated by radiotherapy underwent baseline thyroid hormones (free triiodothyronine, free thyroxine [fT4], and thyrotropin [TSH]) examination and CT scan before radiotherapy. The volume of the thyroid gland was calculated by delineating the structure in the corresponding CT slices using the radiotherapy treatment planning system. The thyroid doses were estimated using the treatment planning system. Subsequent CT scans were conducted at 6, 12, and 18 months after radiotherapy, whereas the hormone levels were assessed at 3, 6, 12, and 18 months after radiotherapy. Trend lines of the volume and hormone level changes against time were plotted. The relationship between the dose and the change of thyroid volume and hormone levels were evaluated using the Pearson correlation test.
Results:
An average of 20% thyroid volume reduction in the first 6 months and a further 8% shrinkage at 12 months after radiotherapy were observed. The volume reduction was dependent on the mean thyroid doses at 6, 12, and 18 months after radiotherapy (r = −0.399, −0.472, and −0.417, respectively). Serum free triiodothyronine and fT4 levels showed mild changes of <2.5% at 6 months, started to drop by 8.8% and 11.3%, respectively, at 12 months, and became stable at 18 months. The mean serum TSH level increased mildly at 6 months after radiotherapy and more steeply after 18 months. At 18 months after radiotherapy, 12 patients had primary hypothyroidism with an elevated serum TSH, in which 4 of them also presented with low serum fT4. There was a significant difference (p = 0.014) in the mean thyroid doses between patients with hypothyroidism and normal thyroid function.
Conclusions:
Radiotherapy for patients with NPC caused radiation-induced changes of the thyroid gland. The shrinkage of the gland was greatest in the first 6 months after radiotherapy, whereas the serum fT4 and TSH levels changed at 12 months. Radiation-induced changes were dependent on the mean dose to the gland. Therefore, measures to reduce the thyroid dose in radiotherapy should be considered.
Introduction
For external beam radiotherapy of nasopharyngeal carcinoma (NPC), neck lymphatics are routinely included in the target volume because over 75% of patients present with clinically positive or occult cervical lymphadenopathy (9). A variable portion of the thyroid gland is included in the irradiation field. The total dose delivered to the thyroid gland depends on the N-stages of the disease and the radiotherapy techniques. The prognosis of patients with NPC has been improving as a result of advancements in radiotherapy techniques. Therefore, it is likely that the risk of thyroid dysfunction after radiotherapy for NPC has also increased. The literature indicates that hypothyroidism after external radiation in the head and neck region usually occurs within 2 years (10 –14). High doses of over 40 Gy to the thyroid gland further shorten the latency period (15) and several authors observed early onset of hypothyroidism within 3 months after radiotherapy (7,16). Since it is estimated that the thyroid gland receives over 50 Gy during radiotherapy for NPC, the onset time of thyroid gland dysfunction could well be within the first 12 months after irradiation. There is little information regarding this, however. Therefore, we carried out a longitudinal study to evaluate radiation-associated changes in the thyroid gland in patients with NPC.
Materials and Methods
This was a prospective longitudinal study of 45 patients with NPC who were treated by external beam radiotherapy between February and August 2008. An additional 15 patients were considered for the study but not included for various reasons that made their participation unsuitable, including recurrent disease, death, development of metastasis, and loss in follow-up. The patients' age range was 24–73 (median 47). There were 33 men and 12 women. Their nodal (N) stage ranged from N0 to N3 (modal stage N2, AJCC 2005). There were no patients with history of thyroid abnormalities or recurrent or residual NPC, as they had been excluded from the study. The patients had received neck irradiation by techniques ranging from single anterior cervical beam to multiple intensity modulated radiotherapy (IMRT) beams to the cervical nodal regions. The single anterior cervical treatment covered the lower mandible down to the supra-sternal notch with a median block to spare the larynx and spinal cord, whereas the IMRT technique used 7–9 beams to irradiate the neck node in continuation with the primary nasopharyngeal tumor. For the IMRT planning, there was no specification of dose constraints to the thyroid gland during the plan optimization process of the inverse planning procedure. Because of the difference in beam arrangements, the volume of thyroid gland irradiated by high dose varied among the patients. This resulted in a spectrum of mean thyroid doses received by the subjects, which facilitated the evaluation of dose–complication relationship in this study. Six-megavolt photons were used for all techniques, and the prescribed dose to the neck ranged from 54 to 66 Gy depending on the N-stage of the patients. The study procedure was explained to all subjects who signed a written consent before the start of treatment. The study was approved by the Research Committees of Cancer Hospital, Shantou University Medical College, and Hong Kong Polytechnic University.
A baseline CT examination, a routine for radiotherapy planning, and thyroid function tests were performed for each subject before the commencement of radiotherapy. The CT image provided the volume information and the first set of CT scans was a prerequisite for the generation of a treatment plan. Thyroid function tests were obtained at 3, 6, 12, and 18 months after completion of treatment. Follow-up CT scans were performed at 6, 12, and 18 months post-treatment as part of routine postradiotherapy follow-up procedures for patients with NPC. During CT, the subjects were supine with the head and neck in a straight position. The contrast medium was administered before the scan to highlight the thyroid in the CT images. The scan included the vertex down to the level of first thorax spine (T1) with 3-mm-thick slices. Images generated from the scanner were transferred to the radiotherapy treatment planning system (TPS) for treatment planning. The volume of the thyroid gland was automatically calculated by the software of the TPS after delineating the thyroid gland in the corresponding CT slices.
Thyroid function tests included serum thyrotropin (TSH), the free triiodothyronine (fT3), and free thyroxine (fT4) and were performed by the electrochemiluminescence method using the Elecsys 2010 analyzer (Hitachi High Technology Corporation, Tokyo, Japan). The reproducibility of the three thyroid hormones tests were acceptable, and their coefficient variations ranged between 1.3% and 1.5%.
The estimation of dose received by the thyroid gland was conducted by the radiotherapy TPS using dose volume histogram, which gave the values of the maximum (hottest spot) and mean doses (average dose within the entire volume of the organ) of the thyroid gland. Pearson correlation test was used to evaluate the relationships between the radiation dose to the thyroid gland dose with the changes in thyroid volume and thyroid function tests.
Results
Thyroid gland volume
There was a trend for the thyroid volume to decrease in the 18 months after radiotherapy (Fig. 1). The mean volume was significantly reduced from 17.13 ± 8.04 cm3 before radiotherapy to 13.64 ± 5.59 cm3 6 months after radiotherapy (paired t-test: p = 0.020), a reduction of 20.0%. The decrease in mean volume was less after 6 months, becoming almost more stable between 12 and 18 months. The mean volumes at 12 and 18 months were 12.89 ± 5.29 cm3 and 12.49 ± 5.46 cm3. The relative percentage volume reduction, which was defined as the volume change at specific time after radiotherapy divided by the volume before radiotherapy × 100%, between 6 and 18 month after radiotherapy was within 8.0%, which was not significant (paired t-test: p = 0.652). The mean doses received by the thyroid gland among all the abnormal subjects ranged from 19.0 to 55.6 Gy. There were significant correlations between the estimated mean thyroid dose and the percentage decrease in thyroid volume at 6, 12, and 18 months after radiotherapy (correlation coefficients −0.399, −0.472, and −0.417, respectively).
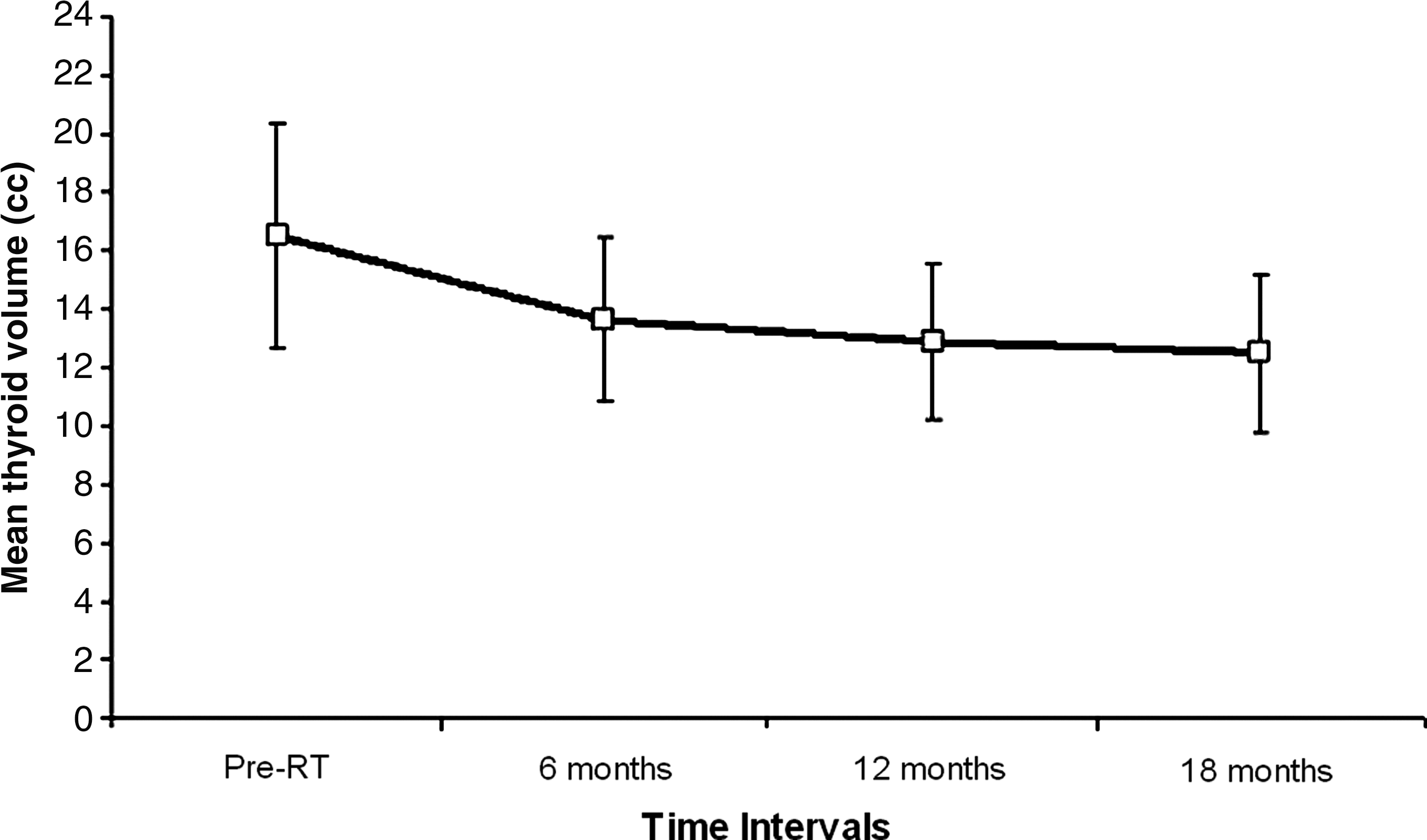
Change of thyroid gland volume before and after radiotherapy at various time intervals.
Thyroid hormones
The mean values of serum fT3 showed little change (2.1%) in the first 6 months after radiotherapy, ranging from 4.87 to 4.77 pmol/L (p > 0.05). During the 6–12-month period after radiotherapy, there was a greater decrease (8.8%) in the serum fT3 (p = 0.03). There was little change (0.2%) in the mean serum fT3 between 12 and 18 months after radiotherapy (p > 0.05) (Fig. 2).

Change of mean free triiodothyronine (fT3), free thyroxine (fT4), and thyrotropin (TSH) levels before and after radiotherapy at various time intervals.
Similarly, the mean values of serum fT4 also showed little change (2.5%) in the first 6 months after radiotherapy, ranging from 14.16 to 16.73 pmol/L (p > 0.05). During the 6–12-month period after radiotherapy, there was a greater decrease (11.3%) in the serum fT4 (p = 0.011). There was a mild change (2.4%) in the mean serum fT4 between 12 and 18 months after radiotherapy (p > 0.05).
The mean values of serum TSH showed little change (2.4%) in the first 3 months after radiotherapy, ranging from 1.66 to 1.62 mIU/L (p > 0.05). During the 3–6-month period after radiotherapy there was a greater increase (21.3%) in the serum TSH (p = 0.001). There were greater increases in the mean serum TSH between 6 and 12 months as well as 12 and 18 months after radiotherapy (83.4% and 32.8%, p < 0.001 and p = 0.001, respectively).
Before radiotherapy, all study patients had with normal serum fT3, fT4, and TSH concentrations. The normal ranges for the three hormones in the local Chinese population are 3.1–6.8 pmol/L, 12.0–22.0 pmol/L, and 0.27–4.20 mIU/L, respectively. Three to 6 months after radiotherapy a few patients presented with abnormal hormone levels (Table 1), but all except two patients returned to normal after 12 months. At 12 months after radiotherapy, 11 patients (including the previous two patients) showed an elevated serum TSH, which was a characteristic of primary hypothyroidism. Among them, four also presented with low serum fT4. One patient showed low serum TSH level and he returned to normal after 18 months. Eighteen months after radiotherapy one more patient showed elevated serum TSH. The rest of the patients had normal thyroid function. There was no patient with thyrotoxic condition (characterized by low serum TSH and normal or high fT3 and fT4) and central thyroid dysfunction (normal serum TSH with abnormal fT3 or fT4). There was a significant difference in the mean thyroid dose between patients with hypothyroidism (45.9 ± 7.5 Gy) and normal thyroid function (36.3 ± 11.1 Gy) (t-test: p = 0.014).
The number in parentheses is the actual number of subjects.
Cases also showed abnormally high TSH.
The subject with abnormal low TSH did not show abnormal low fT4 and fT3.
Normal ranges of fT3, fT4, and TSH are 3.1–6.8 pmol/L, 12.0–22.0 pmol/L, and 0.27–4.20 mIU/L, respectively.
fT3, free triiodothyronine; fT4, free thyroxine; RT, radiotherapy; TSH, thyrotropin.
Significant negative correlations were found between the mean thyroid dose and the change of serum fT4 level at 12 and 18 months after radiotherapy (r = −0.465 and −0.335, respectively). The change of hormone level was defined as the difference between the baseline level (before radiotherapy) and the level at the specified time interval. Significant positive correlations were present between the mean thyroid dose and the change of serum TSH level at 12 and 18 months after radiotherapy (r = 0.415 and 0.420, respectively). However, there was no dose correlation in the serum fT3 level in all time intervals.
There were significant correlations between the percentage volume shrinkage at 18 months after radiotherapy and the reduction of serum fT3 and fT4 levels (r = 0.391 and 0.392, respectively), but there was not a significant correlation between the percentage volume shrinkage at this time and the serum TSH level (r = −0.110).
Discussion
Thyroid gland volume
Several related studies suggest that the causes of radiation-induced thyroid gland damage were due to the damage of small thyroid vessels (17,18), direct thyroid cell injury, and immune-mediated damage (16,19), which subsequently leads to shrinkage of the organ. This likely explains the reduction of thyroid gland volume observed in this study. The shrinkage of the gland was more remarkable in the first 6 months after radiotherapy and then became more stable toward the 12-month interval. This demonstrated that the degree of volume reduction was correlated to the mean dose received by the thyroid gland but not the maximum dose. The explanation for the phenomenon that the volume reduction was independent of the maximum dose is probably that the maximum dose only affected a relative a small volume of the organ (<5%) and was not the determinant of the entire gland reaction.
Thyroid hormones
The changes of the serum fT3 and fT4 levels in the first 6 months after radiotherapy were relatively small and with no definite pattern. However, both of them demonstrated a greater decreasing trend at 12 months after radiotherapy, in which four subjects showed abnormally low serum fT4 levels, and no case of abnormally high serum fT4 level was reported. These results indicated that the effects started to appear at 12 months after radiotherapy. Contrary to the serum fT3 and fT4, the serum TSH level demonstrated an overall rising trend after completion of radiotherapy. The impact on serum TSH levels started at 6 months after radiotherapy and became more significant from 12 months onward. Further, the levels of thyroid hormones were dependent on the mean radiation dose received by the thyroid gland, which echoed the results of several related studies (9,20,21).
In this study, 12 cases of radiation-induced hypothyroidism were observed at 18 months after radiotherapy, all being primary hypothyroidism (high TSH with normal or low fT4). However, the patients did not have clinical symptoms during the study period. Between the end of radiotherapy and 6 months after, there was no case of hypothyroidism.
Our study has demonstrated that the shrinkage of thyroid gland, which was caused by radiation damage, occurred mainly at about 6 months after radiotherapy. Such damage gradually led to the reduced production of thyroid hormones (fT3 and fT4) at around 12 months after radiotherapy. This is the likely explanation of why the changes of fT3 and fT4 levels were dependent on the shrinkage of thyroid volume at 12 months after radiotherapy in this study. At about 12 months after radiotherapy, the reduction of thyroid hormones triggered the increased production of TSH from the pituitary gland that stimulated the thyroid to produce more thyroid hormones. Therefore, a steeper rise of TSH level was observed at 12 months and thereafter. It was expected that the increase of TSH would continue for some time and become more stable when the level of fT3 and fT4 returned to normal levels. Although the 24-month postradiotherapy results were not available in this study (which is a limitation), it was anticipated that the rise of TSH would slow down within 24 months after radiotherapy because our results showed that the levels of fT3 and fT4 were already fairly stable at 18 months after radiotherapy.
There were no cases of central hypothyroidism among the subjects as there was no subject who presented simultaneously with abnormally low TSH, fT3, and fT4 levels. This might be due to the relatively short follow-up period in this study, as the median clinical latent period for central hypothyroidism was reported to be 4.8 years in a study related to the radiotherapy of head and neck tumors (22). Further, central hypothyroidism is mainly caused by pituitary gland damage. Since the mean doses of the pituitary gland of most subjects in this study were below 50 Gy, which was below the tolerance dose of 60 Gy (23) for the pituitary gland, it was expected the clinical impact on the hypothalamic-pituitary axis would not be serious.
Conclusion
The present study has demonstrated that radical external beam radiotherapy to patients with NPC carries the risk of radiation-induced hypothyroidism at about 12 months after radiotherapy, which was manifested by the reduction of physical gland size and change of fT4 and TSH levels. There were correlations between the shrinkage of gland volume and the change of serum fT3 and fT4 levels, but not for the TSH level. The results also demonstrated that radiation-induced hypothyroidism was dependent on the mean dose received by the thyroid gland, and therefore any measures to reduce the thyroid dose in designing the treatment protocol should be considered.
Footnotes
Acknowledgments
This study was supported by research grants from the Hong Kong Polytechnic University, Hong Kong and the Science and Technology Grant of Guangdong Province, China (2008B030301236).
Disclosure Statement
None of the authors have any financial or personal relationships with other people or organization that could influence this study. A similar-topic article was accepted for oral presentation in the Radiological Society of North America (RSNA) conference (December 2010, Chicago).