
Abstract
Background:
Sorafenib is a multi-targeted tyrosine kinase inhibitor licensed for the treatment of hepatocellular carcinoma and renal cell carcinoma. Thyroid function test abnormalities have been reported for different tyrosine kinase inhibitors, but only limited data on thyroid function test abnormalities related to sorafenib are available, demonstrating the occurrence of hypothyroidism in patients treated with sorafenib.
Summary:
We describe two patients who developed temporary hyperthyroidism during the course of sorafenib treatment, which was followed by overt and subclinical hypothyroidism, respectively. Thyroid ultrasonography showed an atrophic thyroid gland in patient 1, and signs of thyroiditis in patient 2. Detailed reassessment of thyroid volumes on routinely performed computerized tomography scans showed a gradual decrease in thyroid volume during sorafenib treatment in one patient, suggesting progressive thyroid destruction.
Conclusion:
This case report describes in detail and for the first time two cases of sorafenib-induced thyroiditis. We assume that this sorafenib-induced destructive thyroiditis is an important cause of sorafenib-induced hypothyroidism.
Introduction
The most common side effects of sorafenib consist of fatigue, gastrointestinal side effects such as nausea and diarrhoea, anorexia, weight loss, and skin toxicity such as hand-foot syndrome (1).
Thyroid function test (TFT) abnormalities have been reported for different TKIs, most notably sunitinib (Sutent™, Pfizer), which has been reported to induce hypothyroidism in 36%–85% of patients (8). Various mechanisms for sunitinib-induced hypothyroidism have been proposed, such as destructive thyroiditis (9 –12), inhibition of iodide uptake (13), reduced synthesis of thyroid hormone (14), and impaired thyroidal blood flow and ischemia (15 –17). Only limited data on TFT abnormalities related to sorafenib have yet been reported, demonstrating that sorafenib is able to induce hypothyroidism as well (18,19). In this report we describe two patients who developed sorafenib-induced thyroiditis, leading to a typical pattern of TFT abnormalities and a variable clinical picture. Written informed consent was obtained from both patients.
Patient 1
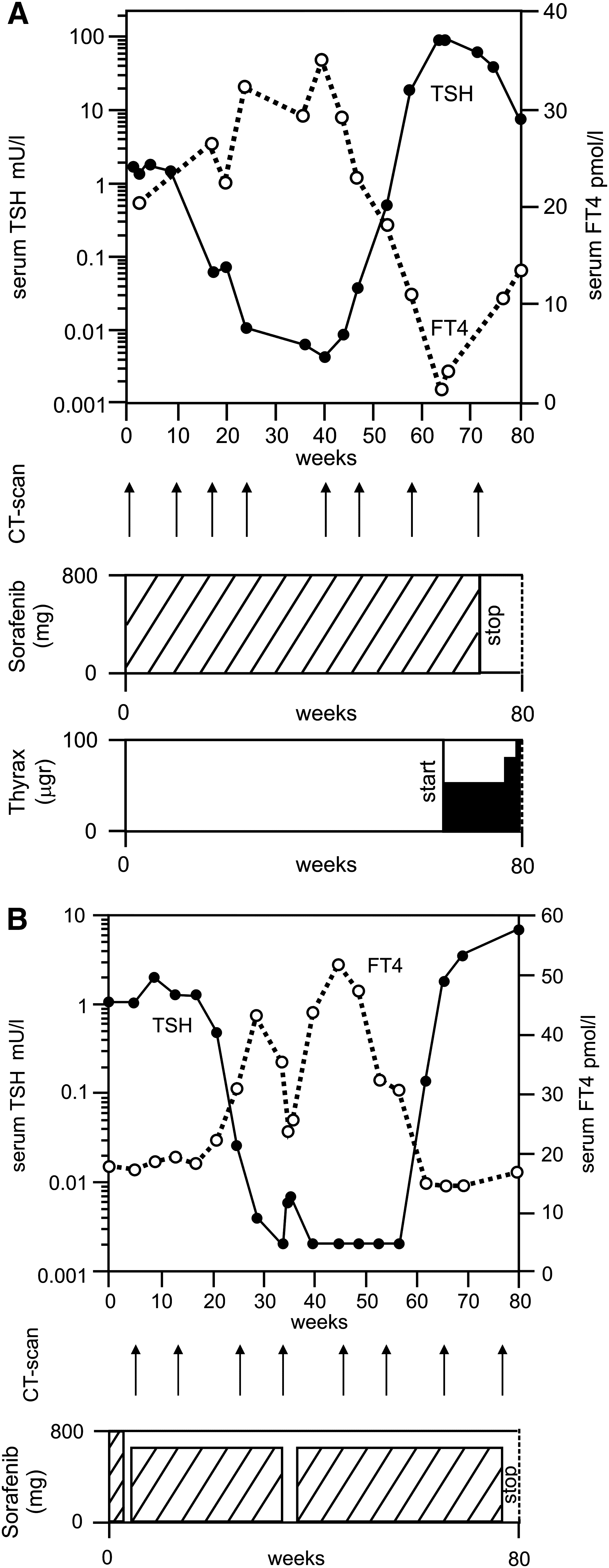
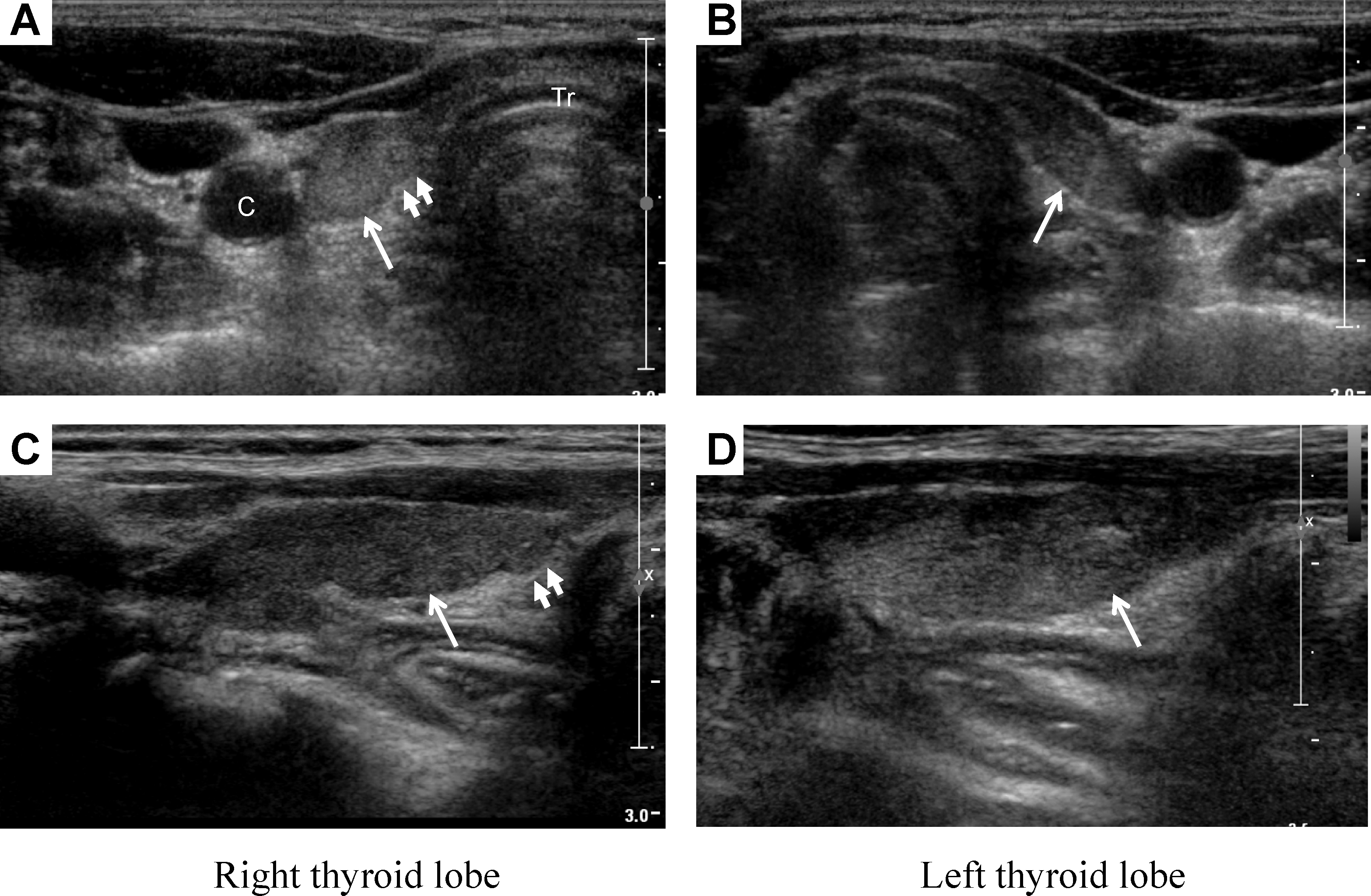
A 49-year-old woman with irresectable fibro-lamellar HCC received 400 mg sorafenib twice daily for 72 weeks. TFTs were performed at baseline and every 4 weeks thereafter, showing normal thyroid stimulating hormone (TSH) and free T4 (FT4) concentrations at baseline. Computerized tomography (CT) scans with intravenous contrast were performed every 2 months. After 17 weeks of treatment, TFTs showed mild biochemical hyperthyroidism (Fig. 1A). Since the patient was asymptomatic, no intervention took place. Sorafenib was continued, while FT4 levels reached a maximum of 35.2 pmol/L after 40 weeks of treatment. TSH levels concomitantly decreased to 0.004 mU/L. The patient remained completely asymptomatic throughout this period. Without any change in sorafenib treatment, FT4 levels subsequently decreased to 1.3 pmol/L after 64 weeks, accompanied by a steep increase in TSH levels to 86.5 mU/L. Thyroid peroxidase (TPO) antibodies were negative. Thyroid ultrasonography revealed profound thyroid gland atrophy. At that time, the patient developed complaints compatible with hypothyroidism (fatigue and weight gain), and levothyroxine treatment was initiated after 64 weeks (with an increasing dose to 100 μg daily), resulting in normalization of TSH and FT4 levels and improvement of symptoms. After 72 weeks of treatment, sorafenib was stopped due to disease progression. Over 30 weeks after stopping sorafenib, hypothyroidism had not recovered and the patient was still dependent on levothyroxine suppletion. A repeat ultrasonography demonstrated an unchanged atrophic thyroid gland with an heterogenous appearance and lobulated outline (Fig. 2), which are considered to be ultrasonographic features of end-stage thyroiditis (20).
Transverse
Patient 2
A 70-year-old man with irresectable HCC received sorafenib for 76 weeks. His TFTs at baseline were normal. Due to skin toxicity, sorafenib was temporarily discontinued and resumed at a 25% lower dose (400 mg morning dose and 200 mg evening dose), resulting in relieve of symptoms. CT scans with intravenous contrast showed stable disease at multiple time points. After 20 weeks of treatment, FT4 levels showed a gradual increase accompanied by a decrease in TSH, resulting in biochemical hyperthyroidism. The patient was completely asymptomatic until 33 weeks of treatment, when atrial fibrillation with high ventricular frequency was detected on a routinely performed electrocardiogram (ECG). At that time TSH and FT4 levels were 0.00 and 35.4 pmol/L, respectively. Thyroid ultrasonography showed signs of thyroiditis, such as an heterogeneous appareance and hypervascularity. Based on the experience with the previous patient, sorafenib-induced hyperthyroidism was suspected. Sorafenib was discontinued, and a β-blocker and coumarin derivative were started for the atrial fibrillation. Rate control was achieved and FT4 levels returned to normal within 7 days after sorafenib discontinuation (Fig. 1B). Sorafenib was resumed at the same dose. After one month, hyperthyroidism re-developed and FT4 levels remained elevated for 5 months. Subsequently, FT4 spontaneously returned to normal. At the last outpatient visit the patient had developed subclinical hypothyroidism, with an increased TSH level of 6.8 mU/L. TPO antibodies were positive, already after 36 weeks of treatment. After 76 weeks of treatment, CT scan analysis revealed disease progression, and sorafenib was stopped. The patient died a few weeks later due to disease progression.
Detailed reassessment of the routinely performed CT scans demonstrated a reduction in thyroid volume during sorafenib treatment in the first patient from 10.3 to 5.3 mL, while the thyroid volume in the second patient remained at a stable volume of 18–19 mL (Fig. 3). The thyroid volume decrease in patient 1 is larger than the inter-observer error (<5%) for thyroid volume measurements on CT and could be considered as a real change (21).
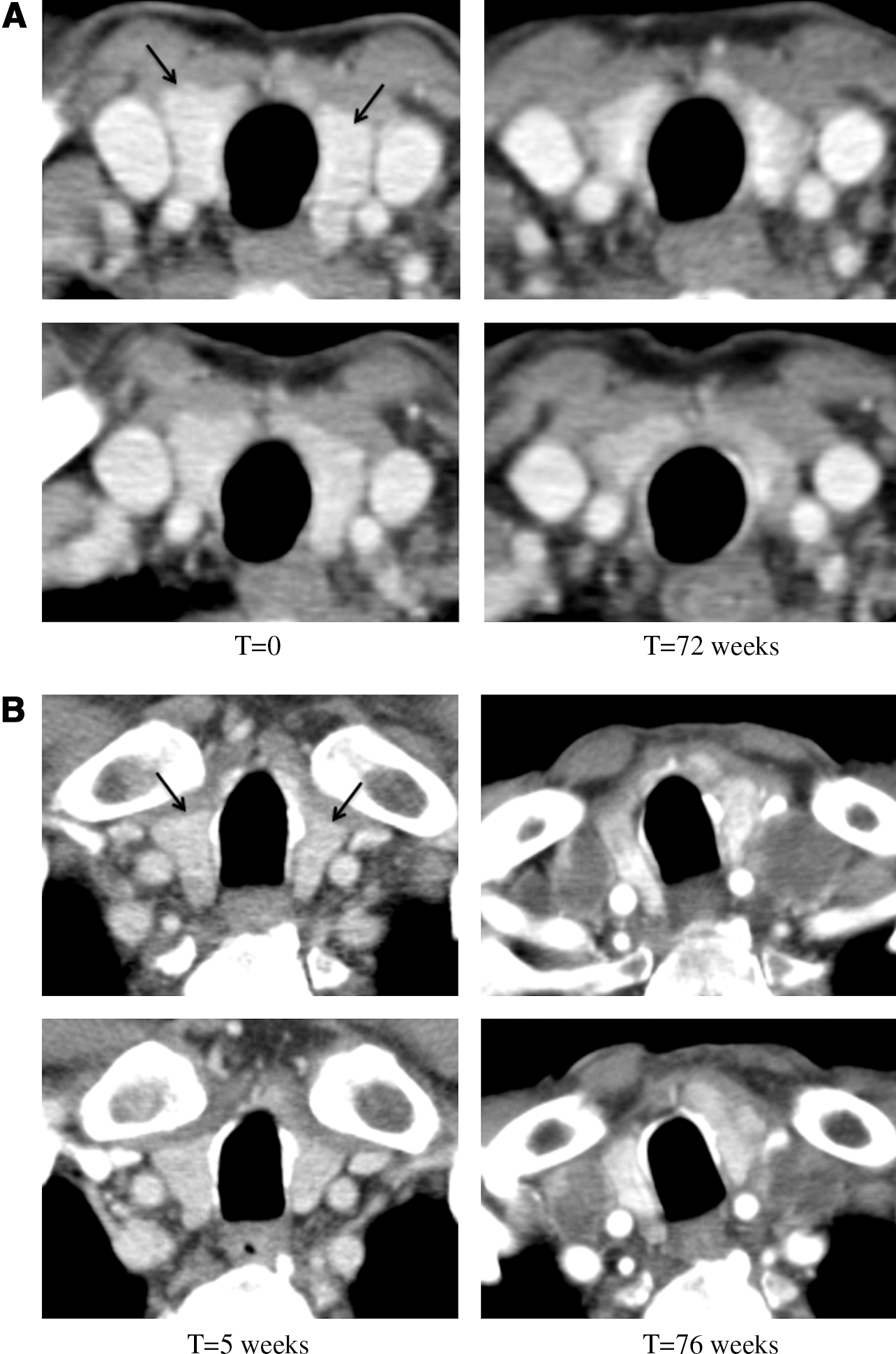
CT scan images (two consecutive 5-mm sections) of patient 1 before and at 72 weeks of sorafenib treatment
In addition to the two patients described, 10 additional patients receiving sorafenib for HCC were prospectively followed. None of these patients developed similar TFT abnormalities.
Discussion
In this report, we describe two patients who developed hyperthyroidism during the course of sorafenib treatment, which was followed by overt and subclinical hypothyroidism, respectively. Thyroid ultrasonography showed an atrophic thyroid gland in patient 1, and signs of thyroiditis in patient 2. Detailed reassessment of thyroid volumes on routinely performed CT scans showed a gradual decrease in thyroid volume during sorafenib treatment in one patient, suggesting progressive thyroid destruction.
The term “thyroiditis” is used for a variety of disorders characterized by an inflammatory response against the thyroid, but there is controversy about the different categories of thyroiditis. The classical pattern of nonautoimmune thyroiditis is characterized by hyperthyroidism, followed by progression (through a period of euthyroidism) to hypothyroidism, and then recovery (22). The hypothyroidism is usually transient, but it can be permanent as well. The pattern of TFTs as was observed in our two patients, with the induction and subsequent spontaneous resolution of hyperthyroidism, followed by the development of (subclinical) hypothyroidism is virtually diagnostic of a thyroiditis (22). A low uptake of radioiodine confirms the diagnosis, because of the loss of functional thyroid tissue, the suppressed TSH, and absence of other thyroid stimulators. Due to the iodinated contrast medium that was used for the regular CT scans in the two patients in this report, no reliable radioactive iodine uptake scan could be performed to confirm the diagnosis.
Theoretically, the altered TFTs in these patients may also have been caused by exposure to iodine from the CT scans. In iodine sufficient areas such as The Netherlands, iodine can cause hyperthyroidism in euthyroid patients with autonomous thyroid nodules. However, the risk of iodine-induced thyrotoxicosis is very rare (23). Since thyroid ultrasonography showed no signs of nodular goiter in both patients, but signs of atrophy and/or thyroiditis, iodine-induced hyperthyroidism is highly unlikely in these patients. Iodine can cause hypothyroidism as well. Excess iodine inhibits thyroid function, a phenomenon called the Wolff–Chaikoff effect. Patients can develop iodine-induced hypothyroidism because of failure to escape from this Wolff–Chaikoff effect (24). Patients with autoimmune thyroid disease are more susceptible to this failure to escape, but other patients can develop iodine-induced hypothyroidism as well. The preceding hyperthyroidism in both patients, and the negative TPO antibodies and persistant hypothyroidism more than 60 weeks after the last administration of contrast in patient 1 make iodine-induced hypothyroidism highly unlikely as well. Furthermore, discontinuation of sorafenib in case 2 resulted in a rapid normalization of TSH and FT4 levels, whereas the same TFT abnormalities reappeared after re-initiation of sorafenib, indicating a causative role for sorafenib.
Drug-induced thyroiditis has been reported for different types of drugs, including amiodarone, lithium, immunomodulators (e.g., interferon-α, interleukin-2, and etanercept) (25 –27), anti-angiogenic agents (e.g., thalidomide and lenalidomide) (28), and sunitinib (9 –17). The patients described in this report did not use any of these drugs. The mechanism via which sorafenib could induce this thyroiditis is unknown. As for sunitinib, thyroid dysfunction does not seem to be due to an autoimmune phenomenon (9,13,15 –17). If sorafenib were to trigger an autoimmune reaction against thyroid tissue, the rapid normalization of TFTs after discontinuation of sorafenib in patient 2 would not be expected. Furthermore, negative TPO antibodies in patient 1 also make an autoimmune process less likely. Although TPO antibodies were positive in patient 2, TPO antibodies at baseline were not known. The rapid normalization of TFTs after stopping sorafenib and the rapid reappearance of these abnormalities after re-starting suggest a more direct toxic effect of sorafenib. Sorafenib has been shown to induce endothelial apoptosis in orthotopic anaplastic thyroid carcinoma xenografts (29). Furthermore, sorafenib inhibits VEGFRs and it has been observed that inhibition of the VEGF signal transduction cascade by VEGFR inhibitors and by soluble fms-like tyrosine kinase 1 lead to a reversible reduction of thyroid vasculature and increased TSH levels in mice (30). One could therefore hypothesize that the decrease in thyroid volume and destruction of thyroid follicular cells is due to regression of the thyroid capillary bed (31). A recent study in patients with pre-eclampsia, which demonstrated that increased levels of soluble fms-like tyrosine kinase 1 are associated with increased levels of TSH, supports this hypothesis (32). Two recent case reports demonstrating a decreased thyroidal blood flow and a shrinkage in thyroid volume, respectively, in patients treated with sunitinib suggest a similar mechanism for this TKI (16,17).
Besides the induction of thyroiditis, sunitinib and other TKIs have also been reported to induce permanent hypothyroidism and altered TFTs (8). Sorafenib has been reported to induce hypothyroidism as well, in 7 out of 39 (∼18%) Western patients and in 46 out of 69 (∼68%) Japanese patients (18,19), which suggests a more severe impact of sorafenib in Japanese patients (19). The frequency of thyroiditis in our cohort (i.e., 17%) is similar to the frequency of sorafenib-induced hypothyroidism in Western patients, and similar to the frequency of Japanese patients who had a suppressed TSH preceding hypothyroidism (∼16%). However, no additional tests to confirm or reject the diagnosis of thyroiditis were specified in the latter study (19). These data together suggest that sorafenib-induced thyroiditis plays an important role in the development of sorafenib-induced hypothyroidism. To our knowledge, no other studies investigating the effect of sorafenib on TFTs have been published.
This study describes in detail and for the first time two cases of sorafenib-induced destructive thyroiditis, which is likely to play an important role in the development of sorafenib-induced hypothyroidism.
Footnotes
Acknowledgment
We thank H. Kneefel for his support with the figures.
Disclosure Statement
The authors declare that no competing financial interests exist.