
Abstract
Background:
Riedel's thyroiditis (RT) is a rare disease characterized by a chronic inflammatory lesion of the thyroid gland with invasion by a dense fibrosis. Publications of the imaging features of RT are scarce. To our knowledge, ultrasound elastography (USE) findings have not been previously reported. Therefore, we describe two patients with RT who were imaged with ultrasonography (US), USE, and fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT).
Summary:
Two women were referred for a large, hard goiter with compressive symptoms (dyspnea and dysphagia); in one patient, the goiter was associated with retroperitoneal fibrosis. In both cases, RT was confirmed by surgical biopsy with pathological examination. Thyroid US imaging was performed with a US scan and a 10–13 MHz linear transducer. The hardness of the tissues was analyzed using transient USE (ShearWave, Aixplorer-SuperSonic Imagine). PET/CT scanning was performed with a Philips Gemini GXL camera (GE Medical Systems). In the first patient, US examination revealed a compressive multinodular goiter with large solid hypoechoic and poorly vascularized areas adjacent to the nodules. The predominant right nodule was hypoechoic with irregular margins. The second patient had a hypoechoic goiter with large bilateral hypoechoic areas. In both cases, an unusual feature was observed: the presence of tissue surrounding the primitive carotid artery, associated with thrombi of the internal jugular vein. Further, USE showed heterogeneity in the stiffness values of the thyroid parenchyma varying between 21 kPa and 281 kPa. FDG-PET/CT imaging showed uptake foci in the thyroid gland. In both cases, US showed a decrease in the thyroid gland volume and the disappearance of encasement of the neck vasculature in response to corticosteroid treatment. In contrast, the FDG-PET/CT features remained unchanged.
Conclusions:
US features, such as vascular encasement and improvement under corticosteroid treatment, seem to be specific to this rare disease. For the first time, USE documents the hardness of RT tissues. Apart from the FDG-PET/CT findings that merit further investigation, US and USE prove useful tools in the assessment of such a rare disease.
Introduction
Imaging Procedure
Ultrasound imaging of the thyroid gland was performed by ultrasound scan (Siemens, Antares 5 and Toshiba Aplio) using a 10–13 MHz linear transducer. 2B and Color Doppler examinations were done, and the volume of the thyroid glands were estimated using the equation, V = (length × width × depth)/2 for each lobe. The echo structure and echogenecity of the parenchyma and the presence of nodules were assessed as well as the lymph node areas and vascular axes.
USE was performed during the US examination, using the same US system and the same probe, which was placed on the neck with light constant pressure. Deformation of nodules and surrounding tissue was recorded by specific encoding according to stiffness.
The hardness of the tissues was analyzed using transient USE. The compression wave (bulk wave) given by the probe generates a tangential sliding wave (ShearWave) whose speed is directly related to stiffness of the tissue. The visualization of this very fast wave is possible with an ultra-speed beam former (Aixplorer-SuperSonic Imagine). The measure was given in kilopascal (kPa). Both patients gave written informed consent.
The cervical, thoracic, and abdominal computerized tomography and the 99mTc thyroid scanning were done for both patients. Abdominal magnetic resonance imaging (MRI) was done for the first patient.
PET/CT scanning was performed by a Philips Gemini GXL camera, GE Medical Systems. The patients had fasted for a minimum of 6 hours before intravenous injection of 5 MBq/kg of 18F-FDG, followed by a tracer uptake phase of approximately 60 minutes. Mean capillary glucose was checked before injection in both patients. For scanning, the patients were positioned supine and head first on the in-line PET-CT system. Images from the upper part of the thorax to mid-thigh level were obtained with arms raised above the head followed by images from the top of the skull to the upper part of the thorax with arms along the thorax. CT scan was performed with parameters set to 80 milliamperage-seconds (mAs) and 150 kilovolt peak (kVp). Slice thickness was 3.75 to 5 mm. For the FDG-PET scan, 4-minute emission acquisitions per field of view were obtained in three-dimensional mode. PET scans were reconstructed in a 128 × 128 matrix with an ordered subset maximum expectation iterative reconstruction algorithm and attenuation correction based on CT data.
Patient 1
A 44-year-old woman had been followed for a multinodular goiter for 13 years. Her goiter suddenly increased in size along with compressive symptoms (dyspnea). Palpation revealed a stonehard, fixed goiter. The thyroid-stimulating hormone (TSH) level was 4.57 mUI/l. The patient was positive for antithyroglobulin antibodies, and her creatinine clearance was 36 ml/min. US revealed a multinodular goiter compressing the trachea with a predominant large, solid, hypoechoic nodule with peri- and intranodular vascularization. This predominant nodule was located in the lower part of the right lobe. Its margins were poorly defined. Large, solid, poorly vascularized hypoechoic areas were observed adjacent to this nodule, but also in the left lobe. The thyroid volume was 72.5 cm2. A feature that could be considered characteristic of RT was the presence of thick tissue surrounding the right common carotid artery, associated with thrombi in the right internal jugular vein (Fig. 1A). There were no pathological neck lymph nodes. The 99mTc thyroid scan showed cold bilateral zones with a hot nodule in the lower part of the right lobe corresponding to the predominant right nodule seen with US. Two large open biopsies taken from the thyroid tissue (one from each lobe) led to the diagnosis of RT. The histopathology showed fibrous tissue with infiltration of the lymphocytes and extension to the muscle fibers.
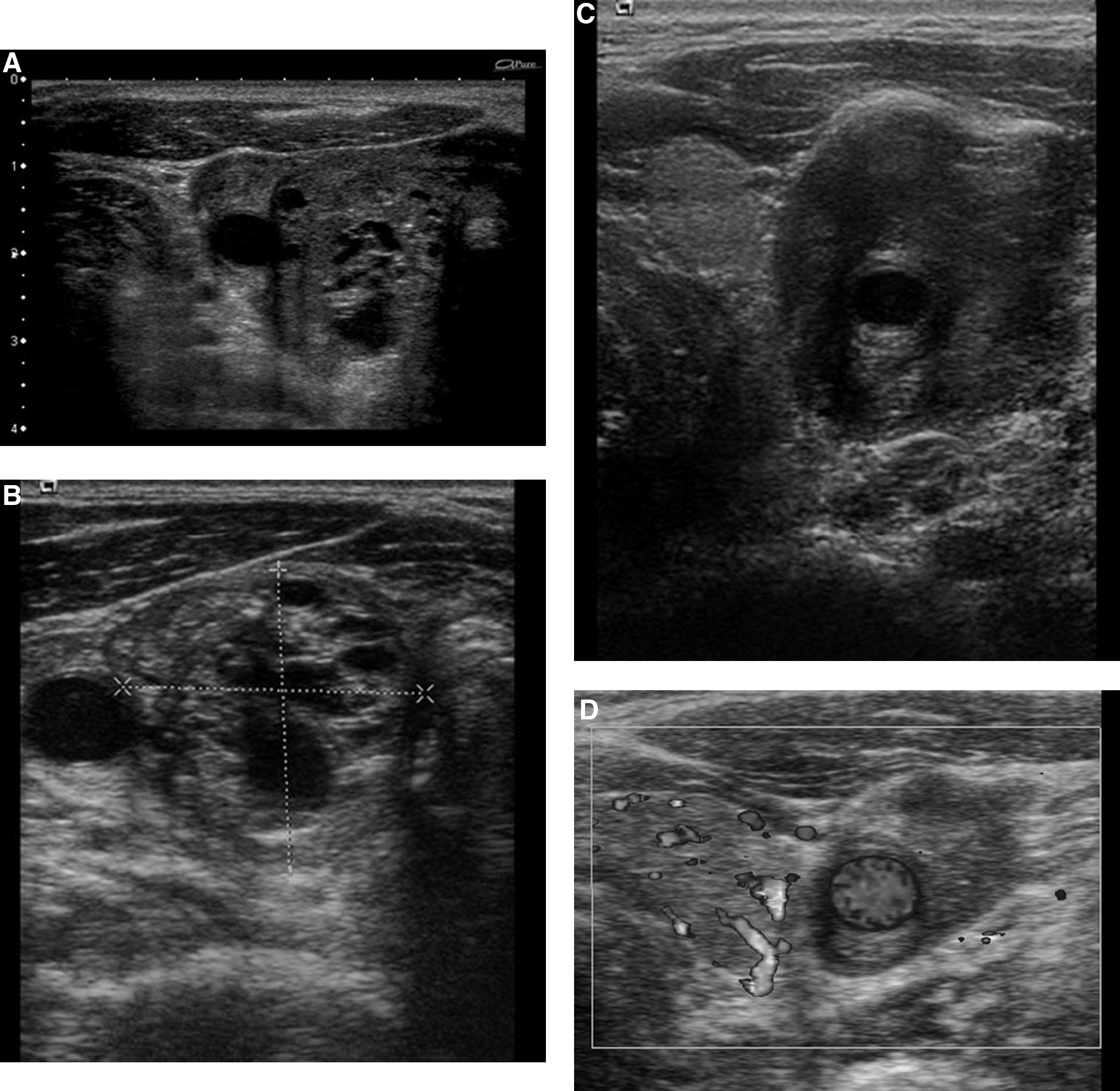
Cervical, thoracic, and abdominal CT showed the large, multinodular goiter with compression of the trachea, and retroperitoneal fibrosis compressing the left ureter with dilatation of the left renal pelvis associated with atrophy of the left renal cortex, without mediastinal fibrosis. Abdominal MRI revealed the presence of a retroperitoneal fibrosis that was significantly enhanced after the gadolinium injection. The patient was treated with a high dose of corticosteroid (1 g/day methylprednisolone) for 3 days followed by 1 mg/kg/day prednisone, which was gradually decreased; levothyroxine; and anticoagulant (antivitamin K). Six months later, the patient's clinical symptoms had improved. Her TSH value was 2.56 mUI/l, and the creatinine clearance rate had risen to 60 ml/min. Thyroid US showed a reduction in the entire thyroid volume to 33.7 cm2, including the hypoechoic region. The size of the predominant right nodule remained stable, but there was a significant decrease in the volume of the thick tissue surrounding the common carotid artery (Fig. 1B). The CT scan showed a decrease in the size of the thyroid gland and of the retroperitoneal fibrosis, with regression of the dilatation of the left renal pelvis.
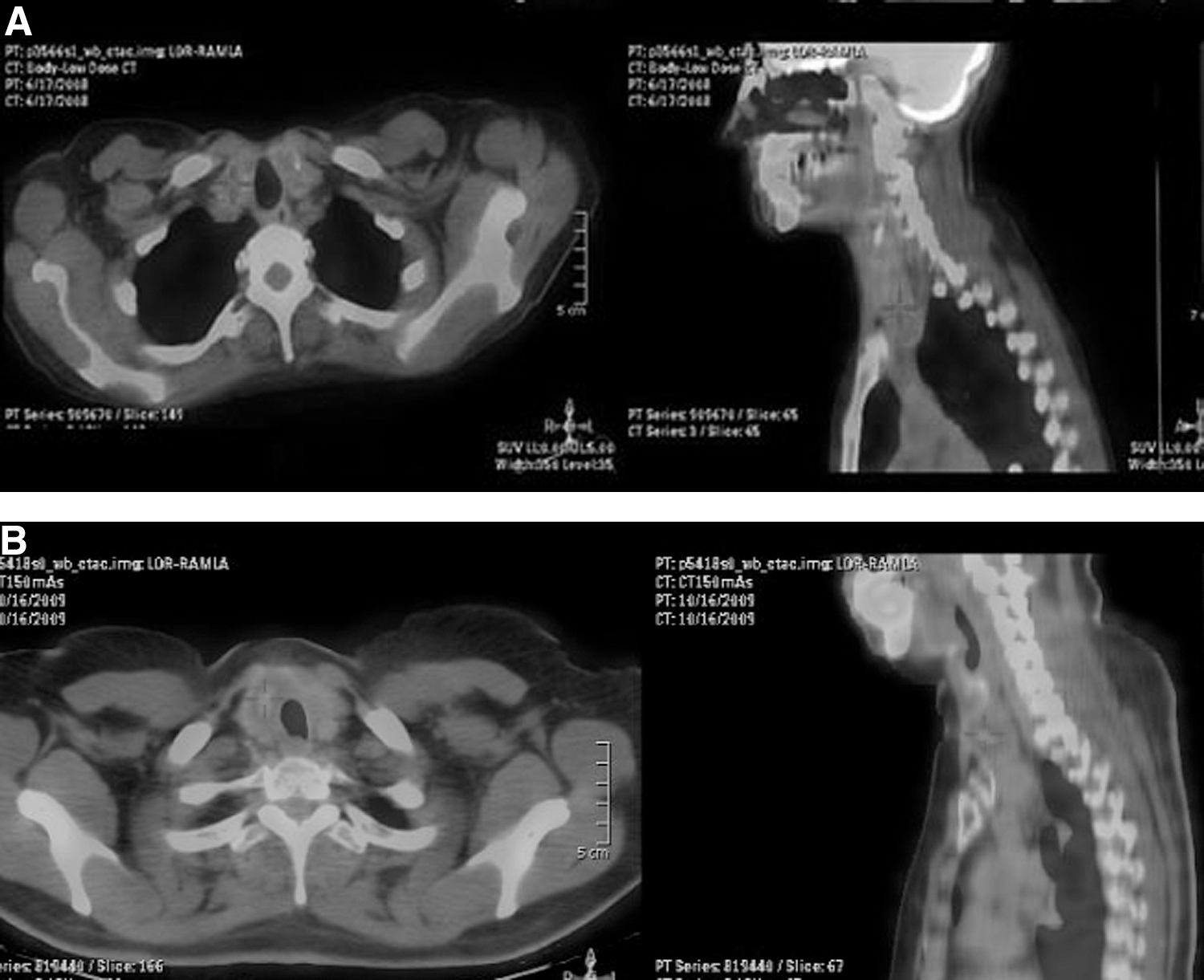
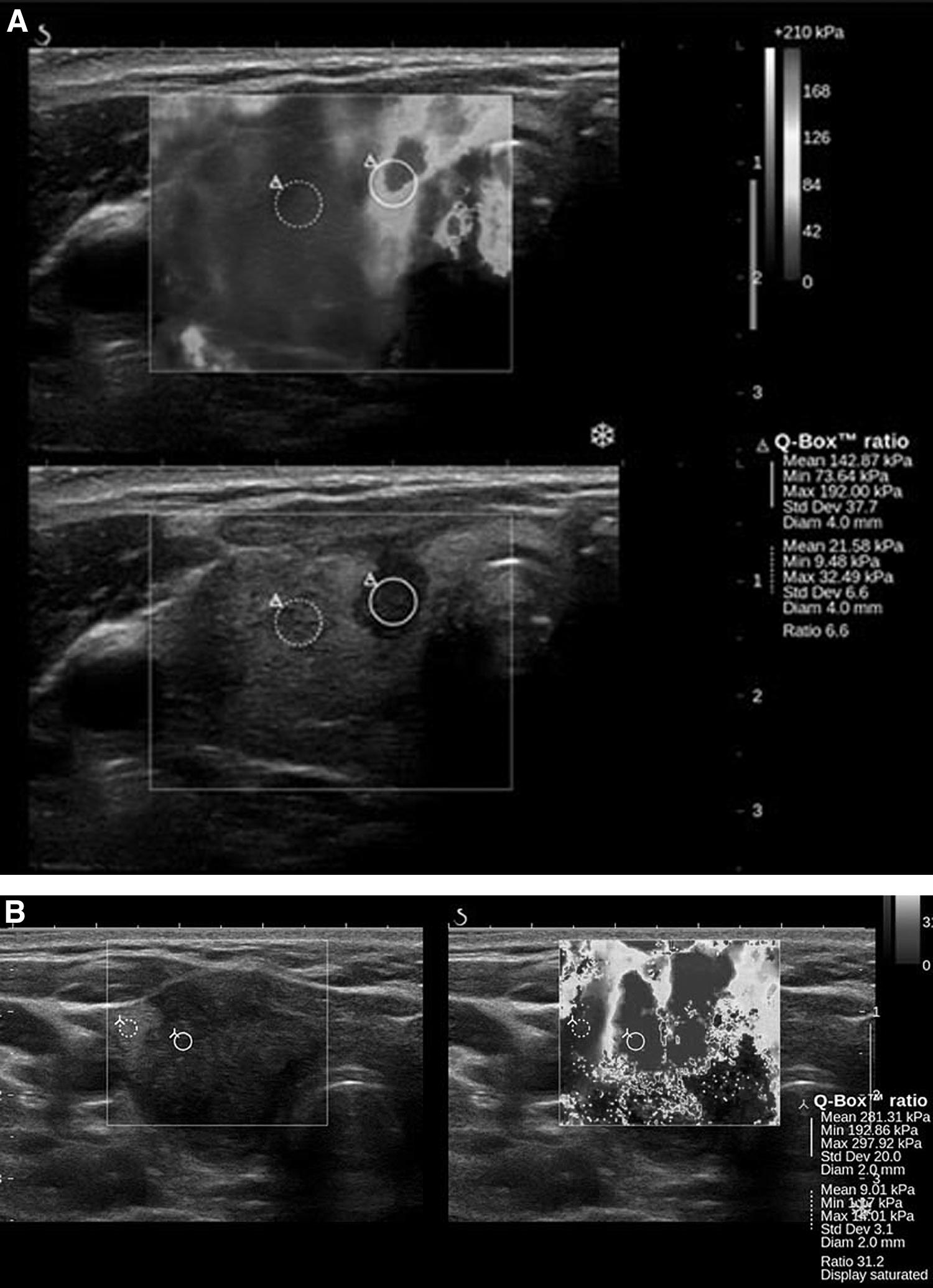
FDG-PET/CT performed 1 year after treatment was initiated and showed a mild increase in uptake in the lower part of the right thyroid lobe (maximum standardized uptake value [SUVmax] at 2.2) without retroperitoneal uptake (Fig. 2A). The abdominal MRI showed loss of the enhancement that had previously occurred after the injection with gadolinium. One year after treatment began, the prednisone dosage was decreased to 5 mg daily. Two years after the beginning of treatment, the FDG-PET/CT uptake foci remained unchanged (SUVmax at 2.8). Corticosteroid treatment was stopped after 2.5 years. At 3 years, clinical compressive symptoms had disappeared. USE, which was not available at the initial diagnosis, was performed and showed heterogeneity in the stiffness values of the nodules: 21 kPa in the right nodule compared with 142 kPa in the very hard initial hypoechoic area discovered adjacent to the right nodule (Fig. 3A).
Patient 2
A 52-year-old woman who had been treated with an insulin pump for type 1 diabetes since 1982 presented with dysphagia, a stone-hard goiter, and an inflammatory syndrome (weight loss, fatigue, and increased levels of c-reactive protein). Her TSH level was 2.72 mUI/l, and her thyroid peroxidase and antithyroglobuline antibodies were positive. The thyroid US showed a homogeneous hypoechoic goiter without nodules. The hypoechoic areas corresponding to RT were large and bilateral. Almost all of the right lobe and 75% of the left one were affected. However, the lower part of the left lobe appeared healthier. The color Doppler examination showed a poorly vascularized gland. The thyroid volume was 36 cm3. The goiter had invaded the adjacent tissues and, as in patient 1, surrounded the two common carotid arteries, especially the left one, with thrombi in the left internal jugular vein (Fig. 1C). There were also bilateral carotid jugular lymph nodes. Cervical, thoracic, and abdominal CTs showed a large heterogeneous goiter without retroperitoneal fibrosis. FDG-PET/CT revealed a mild increase in uptake of the right thyroid lobe (SUVmax at 3.4) (Fig. 2B). The scans revealed no evidence of retroperitoneal fibrosis. The 99mTc thyroid scan showed large, cold bilateral areas. An open biopsy led to the diagnosis of RT. Thus, corticosteroid treatment (1 mg/kg/day prednisone for 1 week and then 0.5 mg/kg/day) was initiated.
Six months after the beginning of the treatment, thyroid US showed a decrease in the volume of the thyroid from 36 to 12 cm3. The right totolobar hypoechoic area significantly decreased in size as did the left hypoechoic area. The tissue that initially surrounded the carotid arteries had decreased (Fig. 1D). A second FDG-PET/CT scan (SUVmax at 3) did not reveal any changes from the scan performed 6 months earlier. After 8 months of treatment, clinical compressive symptoms had disappeared. A US scan revealed that the thyroid volume had not increased from 2 months earlier (12 cm3). USE showed that the right lobe affected by RT was mostly hypoechoic and extremely hard (281 kPa), in contrast to the base of the left lobe, which had a much healthier appearance (only slightly hypoechoic) with normal stiffness (Fig. 3B).
Discussion
RT or invasive fibrous thyroiditis is a chronic inflammatory thyroid disease of unknown etiology that can occur as an isolated disorder or as part of multifocal fibrosclerosis (2). Clinically, it resembles anaplastic thyroid carcinoma or lymphoma, with a stone-hard goiter attached to adjacent structures. The patients complain of a nonpainful, rapidly growing thyroid mass, causing compressive symptoms, such as hoarseness, inspiratory dyspnea, and dysphagia. Most patients are euthyroid, but 30% are hypothyroid. Extracervical fibrosclerosis is found in one-third of cases, and the sites affected include the retroperitoneum, mediastinum, biliary track, and orbit (2).
Fine-needle biopsy in patients with RT is inadequate for making the diagnosis, and an open surgical biopsy is essential to establish the correct diagnosis and to exclude malignancy. Pathological examination shows a stone-hard fibrous mass that destroys the normal glandular architecture. Three criteria are required to make a diagnosis of RT: these include the presence of fibrosis in all or in part of the thyroid gland, near-complete destruction of the affected portion of the gland, and extension beyond the capsule. Surgical treatment depends on the stage of the disease. In our two cases, total thyroidectomy was not possible, and corticosteroid treatment was successfully used.
There are few publications about the appearance of RT with different imaging techniques; even fewer have been performed that measured the progress of the disease during treatment. Previously published sonographic features of RT include a large, homogeneous hypoechoic goiter with a decrease in vascular flow and loss of clear demarcation of the gland where fibrotic invasion of adjacent anatomic structures are present (3,4). A patient with RT associated with massive neck fibrosis was recently reported; this patient had a symmetrically enlarged, diffusely hypoechoic thyroid gland with a massive, heterogeneous soft-tissue mass enveloping the thyroid gland and encasing the neck vasculature. Color Doppler sonography showed only slight vascularization of the mass (5). Our article differs from these previous descriptions of RT in that we have focused on the US, USE, and FDG-PET/CT features of RT.
In both our patients, the ultrasound appearance was typical with voluminous hypoechoic and poorly vascularized goiters (with nodules for Patient 1, although this nodule is not part of RT, as it remained stable after the corticosteroid treatment) and resembled an anaplastic carcinoma or a lymphoma. However, the encasing of the neck vasculature and its improvement under corticosteroid treatment has never been observed in cases of anaplastic carcinoma or lymphoma. These US findings, therefore, appear to be specific to RT. Moreover, in both patients, the decrease in thyroid volume under treatment is further evidence of RT. USE is a recently developed dynamic technique that can be used to identify suspicious thyroid nodules (6). To our knowledge, this is the first article describing USE features in RT. In the two patients with RT, USE revealed heterogeneity in the stiffness values of the thyroid parenchyma. It should be noted that the hypoechoic areas corresponded to the highest stiffness values. These areas could correspond to a high degree of fibrosis. Longer follow-up times are necessary to evaluate the extent to which corticosteroid treatment can alter such stiffness values.
Two previous publications described the FDG-PET/CT features of patients with RT (7,8). The first publication reported a case of RT associated with retroperitoneal fibrosis. The FDG-PET/CT showed an increased uptake of FDG in the thyroid and in an abdominal mass surrounding the aorta. A second FDG-PET/CT done 4 months after initiation of corticosteroid therapy revealed that the uptake foci had disappeared (7). The second study reported described a patient with RT associated with multiple sclerosis. In this case, there was a dramatic decrease in the FDG metabolic activity after 2 weeks of treatment (8).
In our two patients, the FDG-PET/CT showed a mild increase in the SUVmax in the affected thyroid and no visible improvement several months after the initiation of treatment. This could be accounted for by the fact that in the first patient, the first FDG-PET/CT was performed too late after the start of corticosteroid treatment. It is, thus, possible that a high increase in uptake may have been missed in the early stage. For the second patient, the second FDG-PET/CT was done too early after beginning the treatment. Thus, the FDG-PET/CT did not enable us to interpret the effect of therapy with total accuracy. The results could depend on both the stage of the disease and the response to treatment. Although these FDG-PET/CT findings appear limited in our case report, this examination could be useful as a baseline in the assessment of such a rare disease.
Conclusion
In these two cases, apart from the FDG-PET/CT findings that merit further investigation, US and USE features appear promising in the evaluation of RT. The US vascular encasement and improvement with corticosteroid treatment clearly show these features as specific to RT. Moreover, USE documents for the first time the hardness and the heterogeneity of RT tissues. Thus, US and USE prove useful tools in the assessment of such a rare disease.