
Abstract
Background:
Distant metastases from differentiated thyroid carcinoma occur in up to 20% of cases and represent the most frequent cause of thyroid cancer-related death. Metastatic disease to the spine has the potential to cause severe morbidity, including pain, neurological deficit, and paraplegia.
Summary:
We present a case series of eight consecutive patients with symptomatic spinal metastases due to thyroid carcinoma treated by our multidisciplinary team consisting of spinal surgeons, oncologists, and radiologists, with management of each case determined by our surgical algorithm. Four patients underwent surgical decompression and stabilization for spinal metastases causing instability, spinal cord compression, neurological deficit, or intractable pain. Three patients underwent vertebroplasty for focal mechanical pain due to osteolytic metastases in the absence of significant spinal cord compression or spinal instability; one of these patients required subsequent surgical decompression for spinal cord compression. One patient was nonoperatively treated. All patients underwent total thyroidectomy for the primary cancer and adjuvant radioiodine-131 treatment. The only patient with poorly differentiated thyroid cancer, which was refractory to radioiodine-131 died at 6 months after vertebroplasty procedures for symptomatic spinal metastases. One patient with medullary thyroid carcinoma died at 18 months after vertebroplasty. All remaining six patients who had well-differentiated papillary or follicular thyroid carcinoma were alive at an average of 50 months (range: 17–96 months) after diagnosis and treatment of symptomatic spinal metastases and were ambulant, independent, and able to perform activities of daily living and had no significant pain or neurologic symptoms.
Conclusion:
The potential for long-term survival of several years following development of spinal metastases should be considered during the counseling and decision-making process for patients with thyroid cancer.
Introduction
Studies specifically focusing on the outcome and survivorship of patients with vertebral metastases from thyroid carcinoma are currently lacking. As a subgroup of patients with metastatic bone disease, patients with spinal metastases may suffer symptoms due to pathological fracture, spinal cord compression, or structural instability of the spine, such as intractable axial and radicular pain, neurological dysfunction, and paraplegia. Treatment options in metastatic spinal disease include symptomatic medical management, radioidodine, chemotherapy, radiation therapy, vertebroplasty, and surgical decompression and stabilization (8 –10,18 –20). Goals of surgery are to provide symptomatic pain relief, restore spinal stability, and prevent or improve progressive neurological compromise. We present a consecutive case series of eight patients with symptomatic vertebral metastases due to thyroid carcinoma, who were treated in our multidisciplinary unit.
Materials and Methods
This retrospective review consisted of a consecutive series of eight patients who had assessment and treatment for symptomatic spinal metastases due to thyroid carcinoma by our multidisciplinary cancer unit at the Hospital Pellegrin-Tripode (Bordeaux, France) and Institute Bergonie (Bordeaux, France) from September 2001 to September 2009 (Table 1). The medical records, operative notes, and histopathological reports were available for analysis in all patients. Follow-up was calculated from the time of diagnosis of the spinal metastases until death or September 2009.
Treatment algorithm for spinal metastases
The case histories and radiological investigations of all patients were reviewed by our multidisciplinary team comprising spinal surgeons, oncologists, and radiologists concerned with the management of spinal metastases. Specific treatment of the spinal metastases and primary thyroid cancer was determined by our treatment algorithm, with the primary aim of providing palliative relief of symptoms. Surgical indications were for intractable pain resistant to nonoperative measures and pain and/or paralysis due to bony instability or spinal cord compression by tumor. Goals of surgery were to provide pain relief, restore stability, and reverse neurological compromise. Vertebroplasty was preferably performed if patients had focal mechanical pain due to osteolytic metastases in the absence of significant spinal cord compression or spinal instability. Medical treatment involving a combination of bracing, analgesia, radiotherapy, and chemotherapy was performed in patients without bony instability and with symptoms controlled by medication, or if patients refused surgery.
Treatment of primary thyroid cancer and ablative therapy
Definitive treatment of primary thyroid cancer was total thyroidectomy. Average tumor diameter was 3.6 cm (range: 0.9–7.0 cm). Thyroid capsule invasion was observed in three cases and lymph node involvement was observed in two cases. After primary thyroid surgery, all patients with follicular or papillary thyroid carcinoma were treated with 100 mCi radioiodine-131 after withdrawal of thyroid hormone treatment, every 3–9 months during the first 2 years and then once a year until the disappearance of any metastatic uptake. Thyroxine treatment was given at suppressive doses between radioiodine-131 treatment courses. Serial measurements of thyroglobulin and thyroid function tests were performed during follow-up to monitor for progression of disease.
Results
There were five female and three male patients (Table 1). Average age at time of diagnosis of the spine metastasis was 65 years (range: 45–76 years). In four patients, the spinal metastases were the first presentation of the thyroid cancer. All patients presented with local axial pain, with or without symptoms of metastatic epidural spinal cord compression. The primary thyroid carcinoma was asymptomatic in these patients and was subsequently diagnosed only after staging investigations or tissue biopsy of the vertebral lesion. In the remaining four patients, the spinal metastases became symptomatic at 1 month, 14 months, 9 years, and 16 years following diagnosis of the primary thyroid cancer. The histological diagnosis of the thyroid tumor was well-differentiated follicular in three patients, well-differentiated papillary in three patients, poorly differentiated papillary in one patient, and medullary in one patient.
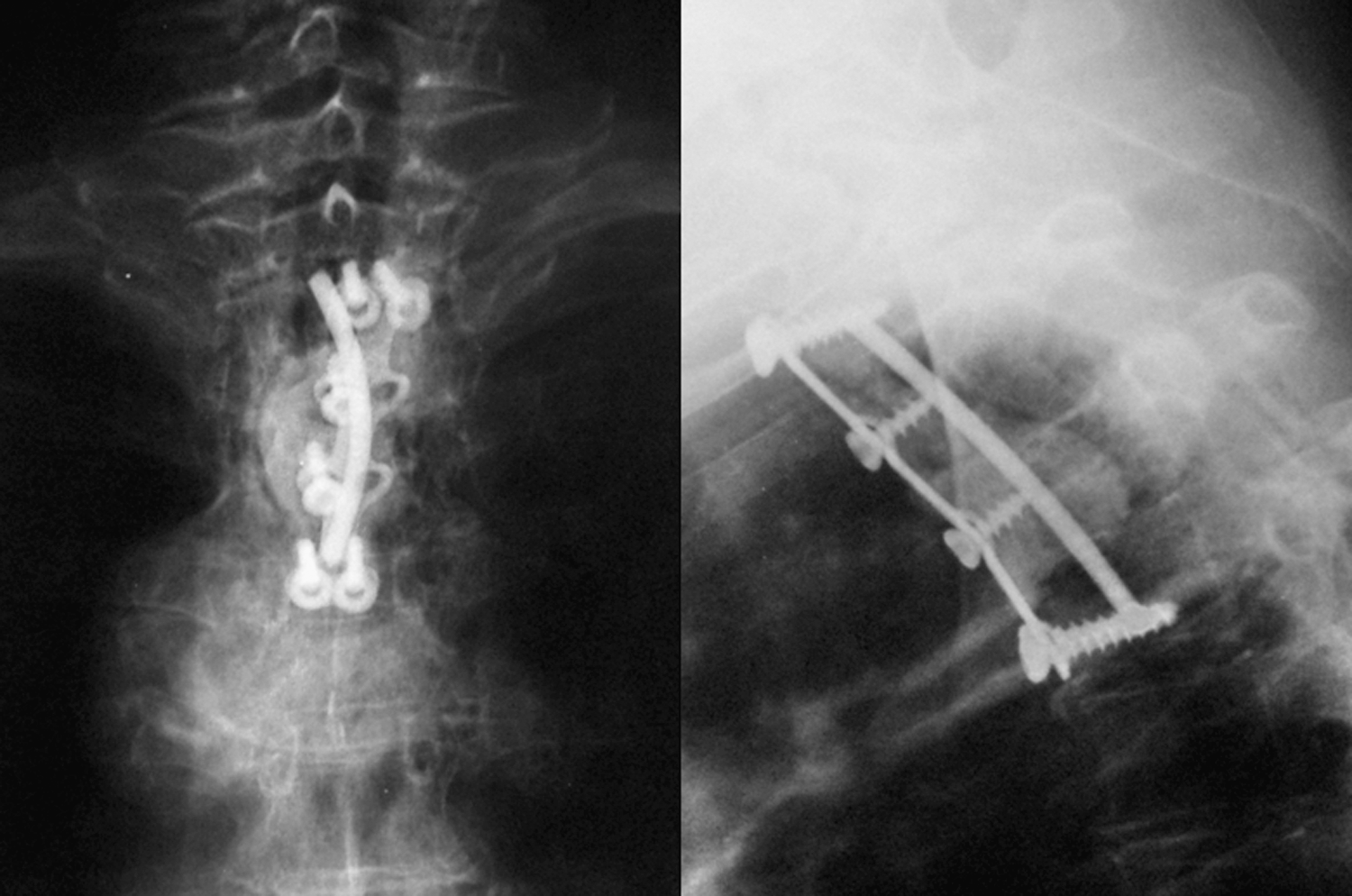
Four patients underwent surgical intervention for symptomatic spinal metastases. Three patients with lumbar metastases underwent posterior decompression and stabilization (Figs. 1 and 2) and one patient with a thoracic metastasis underwent anterior corpectomy and reconstruction with cement and an anterior plate (Fig. 3). One patient with a C3 metastasis was nonoperatively managed. Three patients had vertebroplasty initially performed to thoracic metastases (Fig. 4); one of these patients also required subsequent posterior decompressive surgery after he developed spinal cord compression.
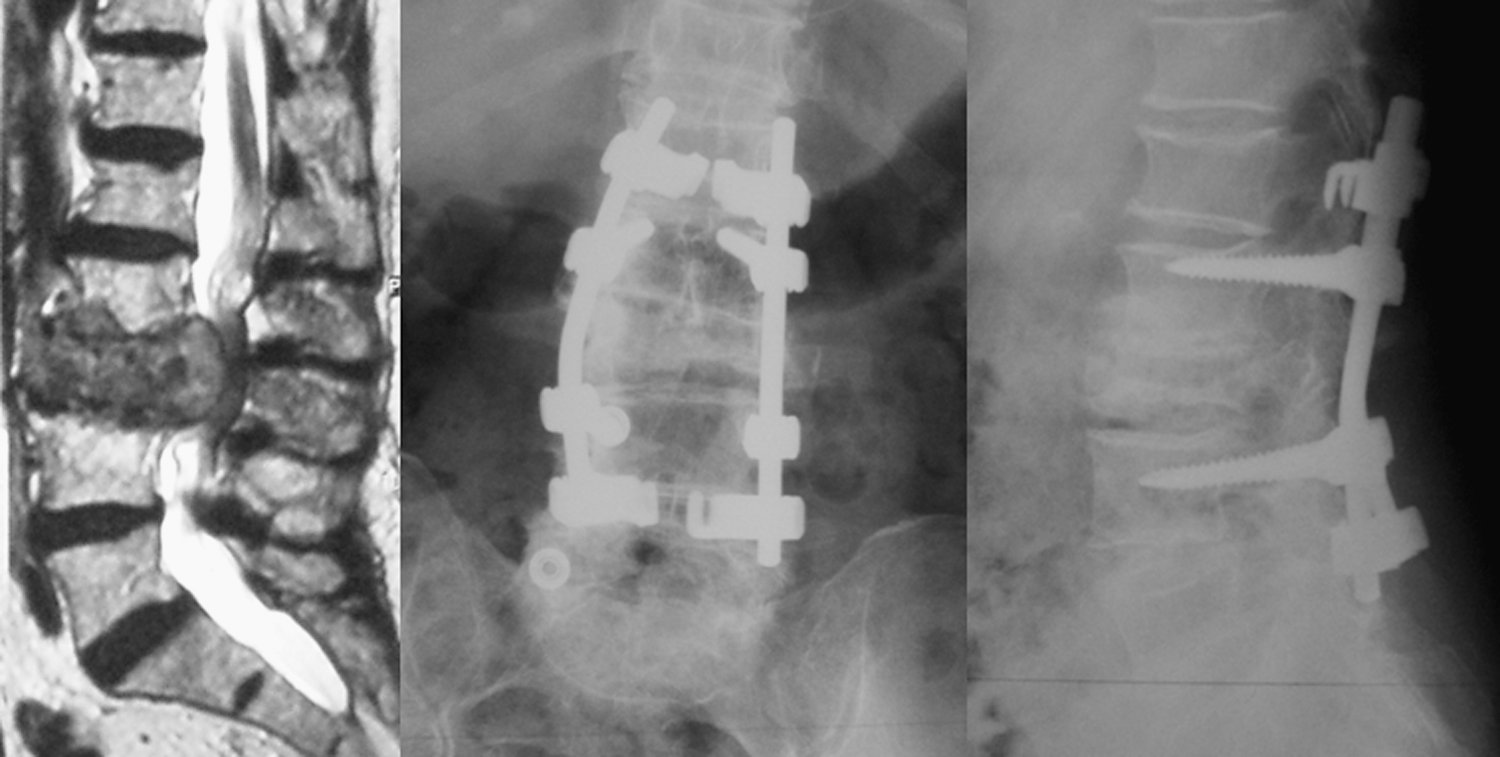
Preoperative sagittal T2-weighted magnetic resonance imaging slice and postoperative anteroposterior (AP) and lateral radiographs following posterior decompression and stabilization of L3 metastasis (Case 1).

Preoperative axial and sagittal computed tomography (CT) scan and postoperative AP and lateral radiographs following posterior decompression, resection, reconstruction with cement, and stabilization of L4 metastasis (Case 3).
Postoperative AP and lateral radiographs following anterior T3 corpectomy and reconstruction with cement and anterior plate (Case 4).

Postoperative coronal and sagittal CT scan AP following T8 vertebroplasty (Case 5).
Mean survival was 39 months (range: 6–96 months) after diagnosis and treatment of the spinal metastasis, with six patients alive at an average of 50 months. One patient had local recurrence of the primary thyroid cancer and was treated with external beam radiotherapy. He was the one with poorly differentiated carcinoma refractory to radioiodine-131 (Case 5). Only one patient achieved complete resolution of primary and metastatic disease (Case 4). All other patients had persistent uptake of radioiodine-131, although all of the six patients who were alive and available for review were ambulant, independent, and able to perform normal activities of daily living and had no significant local axial pain or spinal cord compression due to the spinal metastases.
Discussion
There is paucity in the current literature of histology-specific analyses of spinal metastases. Most studies include patients with metastatic thyroid cancer as a subset of patients in a larger heterogenous group of patients with a variety of different histological tumor types. In these studies, the numbers of patients with thyroid metastases are invariably low. Further, less than 10% of patients with bone metastases from thyroid carcinoma have symptomatic spinal cord compression requiring surgery (7,9). There are very few reports specifically focusing on the treatment and survival of patients with spinal metastases due to thyroid carcinoma. All our patients had total thyroidectomy surgery for the primary tumor, regardless of whether they presented with metastatic disease, because this facilitates scanning for metastases and, if present, more efficient treatment of these with radioiodine, which would have been preferentially taken up by thyroid tissue in the neck if total thyroidectomy had not been performed.
Previous retrospective studies have identified several potential prognostic factors affecting survival in patients with metastatic thyroid carcinoma (2,6 –8,11 –13,18,19,21,22). The strongest prognostic factors are younger patient age, histologic subtype of the tumor, and radioiodine avidity of the metastasis. Consistent with these observations, six of the eight patients in our series had well-differentiated papillary or follicular thyroid carcinoma that was responsive to radioactive iodine and had at least 12 months' survival following diagnosis and treatment of their symptomatic spinal metastases. Indeed, all six patients were alive at up to 8 years (average: 50 months) following successful treatment of the spinal metastasis. One patient died at 6 months following vertebroplasty to thoracic spine metastases and 20 months following primary thyroidectomy; however, this patient had poorly differentiated papillary carcinoma, which was refractory to radioactive iodine. The other patient who died had medullary thyroid carcinoma, which does not take up iodine.
Our observations are consistent with those of Abdel-Wanis et al. (23), who reported the outcome of 14 patients who underwent a total of 25 operations for thyroid cancer spinal metastases, with reoperations usually due to local recurrence. In their series, one patient died in the third postoperative day because of disseminated intravascular coagulopathy, five died because of the original illness after a mean of 67.8 months, and eight patients were living after a mean of 53.1 months. The authors concluded that because of an anticipated long survival, a radical therapeutic attitude should be considered in thyroid cancer spinal metastases. Indeed, Demura et al. (24) recently suggested that total en bloc spondylectomy may provide better local control of thyroid cancer spinal metastases compared with debulking surgery. Enkaoua et al. (4) retrospectively analyzed a series of 34 patients with metastatic thyroid cancer to the spine who underwent excisional or palliative spinal surgery. The subgroup of patients with thyroid carcinoma spinal metastases was evaluated alongside patients with renal cancer spinal metastases and metastases of unknown origin. The authors reported postoperative partial or complete relief of pain in 94% of patients and immediate restoration of stability in all cases except one. The neurologic condition of all patients except one either improved or stayed the same. The authors concluded that excisional or palliative surgery for thyroid spinal metastases provided good clinical results. More recently, minimally invasive techniques have been developed for select groups of patients. Percutaneous vertebroplasty and kyphoplasty represent viable alternatives to surgery in patients with severe focal mechanical pain due to osteolytic metastatic vertebral fractures in the absence of significant spinal cord compression or spinal instability (25). Similar to the two cases recently reported by Kushchaywev et al. (20), our patients who fit these criteria and were treated with vertebroplasty had immediate good symptomatic resolution.
Although distant metastases are the main cause of thyroid cancer-specific mortality, many patients may be long-term survivors (3). This long-term outcome depends on patient factors, tumor biology, and the adequacy of treatment. In our case series, patients presenting with symptoms from spinal metastases due to thyroid carcinoma who underwent prompt surgical decompression and stabilization of the spinal metastasis followed by total thyroidectomy and radioactive iodine to the primary and metastatic sites and then suppression of thyroid-stimulating hormone with exogenous thyroxine and regular follow-up had prolonged survival, provided their tumor was not poorly differentiated or did not take up radioiodine.
Conclusion
Our patients with vertebral metastases from well-differentiated thyroid carcinoma who had palliative surgical resection and stabilization, complete thyroidectomy for the primary cancer, and adjuvant radioiodine-131 treatment had prolonged survival. The potential for survival of several years following development of spinal metastases should be considered during the counseling and decision-making process for patients with thyroid cancer. As long survival may be anticipated, we recommend excising as much of the tumor as possible during surgery for symptomatic spinal metastases.
Footnotes
Acknowledgment
This work was supported by the National Health and Medical Research Council of Australia (Fellowship No. 558418 to G.M.Y.Q.).
Disclosure Statement
The authors declare that no competing financial interests exist.