
Abstract
Background:
Papillary thyroid cancer (PTC) is the most common differentiated thyroid carcinoma. Metastases usually occur in regional lymph nodes or to lungs. Distant metastases to skeletal muscle are rare. Here, we report a patient with a solitary metastasis to skeletal muscle.
Patient Findings:
A 31-year-old woman was found on routine physical examination to have a 1-cm nodule in the right thyroid lobe. The patient underwent endoscopic total thyroidectomy with central cervical lymph node dissection in April 2008. Pathological analysis showed a 1.5 × 0.9 cm PTC in the right thyroid lobe with extension into perithyroidal soft tissue and lymph node involvement (all six central lymph nodes examined were positive). After surgery, she received 100 mCi of radioactive iodine. Subsequently, the patient was found to have a lateral neck recurrence and, therefore, underwent right unilateral modified radical neck dissection followed by additional radioactive iodine ablation. In February 2010, her serum thyroglobulin was 19.4 ng/mL, but the neck ultrasound was negative. However, a fluorodeoxyglucose (FDG) positron emission tomography scan showed focal FDG uptake in the vastus medialis muscle of the right distal femur. A 0.9 × 0.5 cm, well-defined, whitish mass in the vastus medialis muscle was confirmed on histopathology to be metastatic PTC.
Summary:
Here, we report an adult woman who presented with a thyroid nodule that was noted to be PTC on histopathology after total thyroidectomy. Almost 2 years later, she was noted to have had focal FDG uptake consistent in the region of the right femur. A solitary metastasis of PTC in the right vastus medialis muscle was resected. A MEDLINE (Medical Literature Analysis and Retrieval System Online) search showed that this is only the third report of PTC with a distant, solitary skeletal muscle metastasis.
Conclusions:
Distant skeletal metastasis in PTC is very rare. Until the availability of FDG to detect skeletal metastasis of PTC, they may have been more difficult to discern.
Introduction
Although extrathyroidal extension into the soft tissues of the neck may occur in PTC, distant metastases, except to lungs, are rare. Skeletal muscle metastases from a differentiated thyroid carcinoma are quite rare, particularly a solitary metastasis. To our knowledge, there have been only two reports; one of these was to the biceps muscle (12) and the other to the trapezius muscle (13). Here, we report a patient with PTC and a metastasis to the right vastus medialis muscle.
Patient
A 31-year-old woman was found on routine physical examination to have a nodule in the right thyroid lobe. A neck ultrasound (US) showed an approximately 1-cm hypoechoic nodule in the right thyroid lobe. It was diagnosed as PTC by fine needle aspiration (FNA). A neck computed tomography (CT) with contrast showed an ill-defined, ovoid, moderately enhancing 1-cm nodule with ipsilateral central neck lymphadenopathy. Thyroid function tests demonstrated a euthyroid state.
The patient underwent endoscopic total thyroidectomy with central cervical lymph node dissection in April 2008. The pathological analysis showed a unifocal and unilateral PTC, 1.5 × 0.9 cm, in the right thyroid lobe with extension into the perithyroidal soft tissue and lymph node involvement (all six central lymph nodes examined were positive for PTC). After a total thyroidectomy, the patient received 100 mCi of radioiodine in July 2008. At that time, serum thyroglobulin (Tg) level was 25 ng/mL, but whole body radioiodine scanning (WBS) and neck US were negative. Six months after total thyroidectomy, her Tg level was 4.4 ng/mL, and neck US did not reveal tumor recurrence or lymphadenopathy. To evaluate the patient further, we performed a neck CT and an F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) scan. The neck CT showed a small area of lymphadenopathy in the right mediastinum and right lateral neck (level IV). This FDG-PET scan showed focally increased FDG uptake in the right level IIb and level IV cervical lymph node chains.
In November 2008, she underwent unilateral modified radical neck dissection (MRND) (Table 1). Histological examination of 10 lymph nodes showed four metastases in the dissection of the material from the right lateral neck. After MRND, the patient received a second 100 mCi dose of radioactive iodine in April 2009. At that time, her Tg level was 21.0 ng/mL, and her 131I WBS showed no uptake. After 6 months, her Tg level was 0.1 ng/mL, and there was no evidence of recurrence on follow-up US. Six months later, her Tg level was 1.7 ng/mL, and there was no evidence of recurrence on follow-up US. However, PET-CT showed uptake at in the right neck level III lymph nodes and in the high right mediastinum. After 4 months, her Tg level was 3.5 ng/mL, and her Tg antibody levels were 19 U/mL. One week later, the patient's Tg level increased to 19.4 ng/mL, but there was no significant interval change in the small area of greatest mediastinal lymphadenopathy on the right as noted on neck CT. However, a repeat FDG-PET scan showed focal FDG uptake in the vastus medialis muscle of the right distal femur and mild FDG uptake (Fig. 1) in a high right mediastinal lymph node and a right level III cervical lymph node. The cytology from a core biopsy of the nodule in the right vastus medialis muscle demonstrated PTC. The high mediastinal lymph node could not be biopsied with FNA due to its location. The patient underwent selective lymph node dissection to biopsy the mediastinal lymph nodes and wide excision of the mass in the right vastus medialis muscle after tattooing.
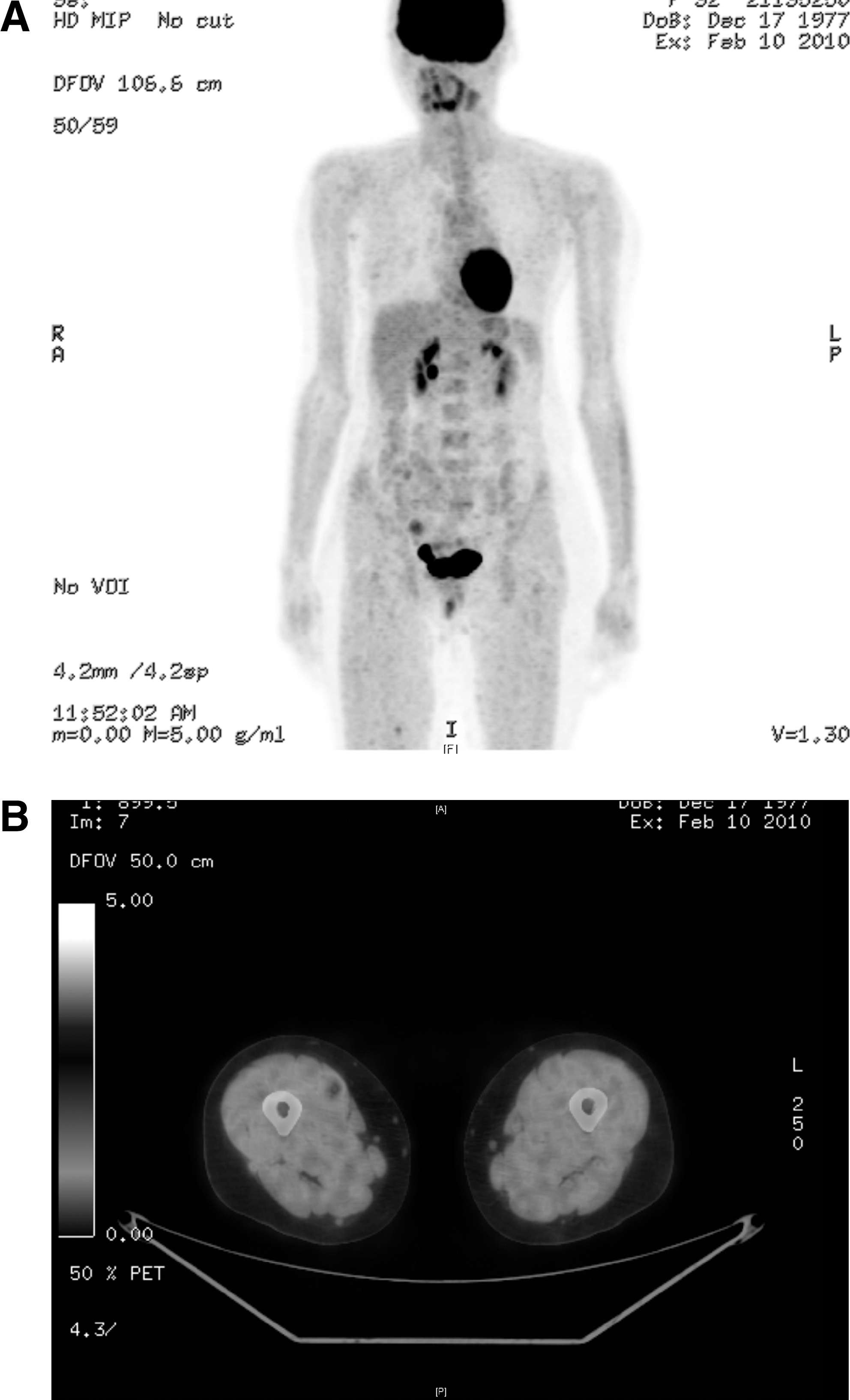
Fluorodeoxyglucose–positron emission tomography showing focal fluorodeoxyglucose uptake in the vastus medialis muscle in the right distal femur. Coronal view
Tg, thyroglobulin; POD, postoperative day; TT, total thyroidectomy; CLND, central lymph nodes dissection; SLND, selective lymph nodes dissection; Ex, excision; RAI, radioactive iodine ablation; FDG, fluorodeoxyglucose; PET, positron emission tomography; CT, computed tomography.
Three of four mediastinal lymph nodes showed metastatic PTC; the other samples were identified as thymus. The 0.9 × 0.5 cm, well-defined, whitish mass in the vastus medialis muscle was resected and confirmed on histopathology to be as metastatic PTC (Fig. 2).

Primary papillary thyroid carcinoma showing extension to the perithyroidal soft tissue
Discussion
PTC is commonly associated with lymphatic spread to cervical lymph nodes (14,15). Therefore, metastases commonly occur in regional lymph nodes, whereas distant metastases are a rare occurrence. The most common sites for distant metastases of PTC are the lungs, followed by the bone; rare metastases occur in the liver and brain (2,8,16). There are also rare reports of metastases to the following sites: the adrenal, kidney, ovary, orbit, and sphenoid sinus (1,7,10,11,17,18). Skeletal muscle metastases from a differentiated thyroid carcinoma are reported to be extremely rare, even for follicular thyroid carcinoma, which is well known for its hematogenous spread to various sites (i.e., to lung, bone or brain) (13,19).
This is the third reported case of PTC manifesting as a solitary skeletal muscle metastasis, with previous reports finding metastases in the upper extremity muscle and trapezius muscle (12,13).
A case of PTC presenting as solitary metastasis in the right bicipites muscle was described in an elderly male patient (12). This was thought after ultrasound scan and magnetic resonance imaging to be a soft tissue tumor. The patient subsequently found to have a toxic goiter with a primary 3.5 cm PTC in the left lobe of the thyroid. The second case was a 69-year-old female patient who had a PTC metastasis to the trapezoid muscle metastasis (13). She had a painless lump that did not have uptake on 131I-whole body scan. She did not have other imaging studies. In both of these patients, the PTC was well differentiated and of a follicular variant.
The follow up of PTC is based on clinical evaluation, neck US, Tg levels, and 131I-WBS. Postoperative serum Tg levels and radioiodine scans are sensitive methods to detect metastatic disease (20). A radioiodine scan can localize a lesion with high sensitivity and specificity, but the accuracy for anatomical localization of abnormal findings is often problematic, particularly in soft tissues. Due to the fact that the iodine scan is a functional diagnostic tool that only visualizes iodine, there are no anatomic landmarks on the scan (21 –23). Importantly, 131I-WBS-negative thyroid cancer occurs in up to 20% of patients with DTC (24). When the 131I-WBS is negative, but Tg is detected in serum, it is difficult to locate metastases in an evaluation limited to the cervical area.
There are some reports of multiple distant skeletal muscle metastases from PTC (25 –28). In two of these patients, there was iodine uptake on 131I-WBS (26,27). In the present patient, an 18F FDG-PET scan associated with fine-needle cytology demonstrated the presence of a solitary distant metastasis. Recently, there have been several reports that emphasize the usefulness of FDG-PET as a tool for localizing such recurrences in the presence of elevated Tg and negative 131I-WBS (21,23,24,29 –32).
Radiolabeled FDG is a glucose analog that accumulates in tissues that are metabolically active. FDG is labeled with 18F at the 2′ hydroxyl position, which prevents the normal degradation during glycolysis and allows the radiolabeled FDG to accumulate within the tissue. Malignant tissues tend to have increased metabolism compared with normal surrounding tissues, which provides an opportunity for differential accumulation of radiolabeled FDG in malignant tissues compared with benign tissues. When 18F-FDG-PET and CT are performed, functional information can be coregistered with anatomic imaging (33).
In the patient reported here, FDG-PET was valuable in localizing the hypermetabolic abnormalities to specific anatomical regions. FDG-PET makes it possible to perform a whole body examination with tomographic imaging, greater spatial resolution, and, therefore, high sensitivity. Further, FDG-PET is able to focus on a specific area of the body, thus facilitating radiologic interpretation (21 –23).
In summary, this is only the third reported case of a distant solitary skeletal metastasis from PTC. It is important to recognize that a solitary metastasis with a negative radioiodine scan may occur in a small minority of patients with PTC.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.