
Abstract
Background:
Pretibial myxedema (PM) is an uncommon and characteristic manifestation of Graves' disease (GD), with local autoimmune reaction in cutaneous tissue. The treatment of PM is a clinical challenge. We herein report a patient with PM who achieved complete remission by multipoint subcutaneous injection of long-acting glucocorticid.
Summary:
A 38-year-old man presented with an 18-month history of GD and a 1-year history of PM. Physical examination revealed mildly prominent eyes, diffuse enlargement of the thyroid gland, and PM of both lower extremities. The patient was treated with triamcinolone acetonide by multipoint subcutaneous injections in a combined dose of 20 mg in each lower extremity administered every 25–28 days. The injection was started from the borderline of the lesions and normal skin by selecting 4 to 5 points per leg for each course and then moving to other parts in subsequent courses of treatment. The depth of needle insertion was 0.5–1.0 cm. The patient's PM achieved complete remission in both lower extremities after an approximately 6-month period that included seven courses of treatment with a total dosage of 280 mg triamcinolone acetonide.
Conclusions:
Our experience with this patient suggests that multipoint subcutaneous injection of long-acting glucocorticid is a safe, effective, and convenient treatment of PM in patients with GD.
Introduction
Case Report
A 38-year-old man was admitted to our hospital because of heat intolerance, heart palpitation, and weight loss for 18 months and PM for 1 year. Eighteen months previously, he developed heat intolerance, excessive sweating, palpitations, an increased appetite, weakness, and weight loss. He visited the local hospital about 6 months later, where he was diagnosed as having GD. After being treated with 300 mg of propylthiouracil daily for a month he felt some relief of these symptoms but began to develop PM. He visited several hospitals and was given oral prednisone, 40 mg/day for 2 weeks. The PM continued to expand, however, and he had the onset of thyrotoxic periodic paralysis. Prednisone was stopped and he was treated with oral potassium chloride.
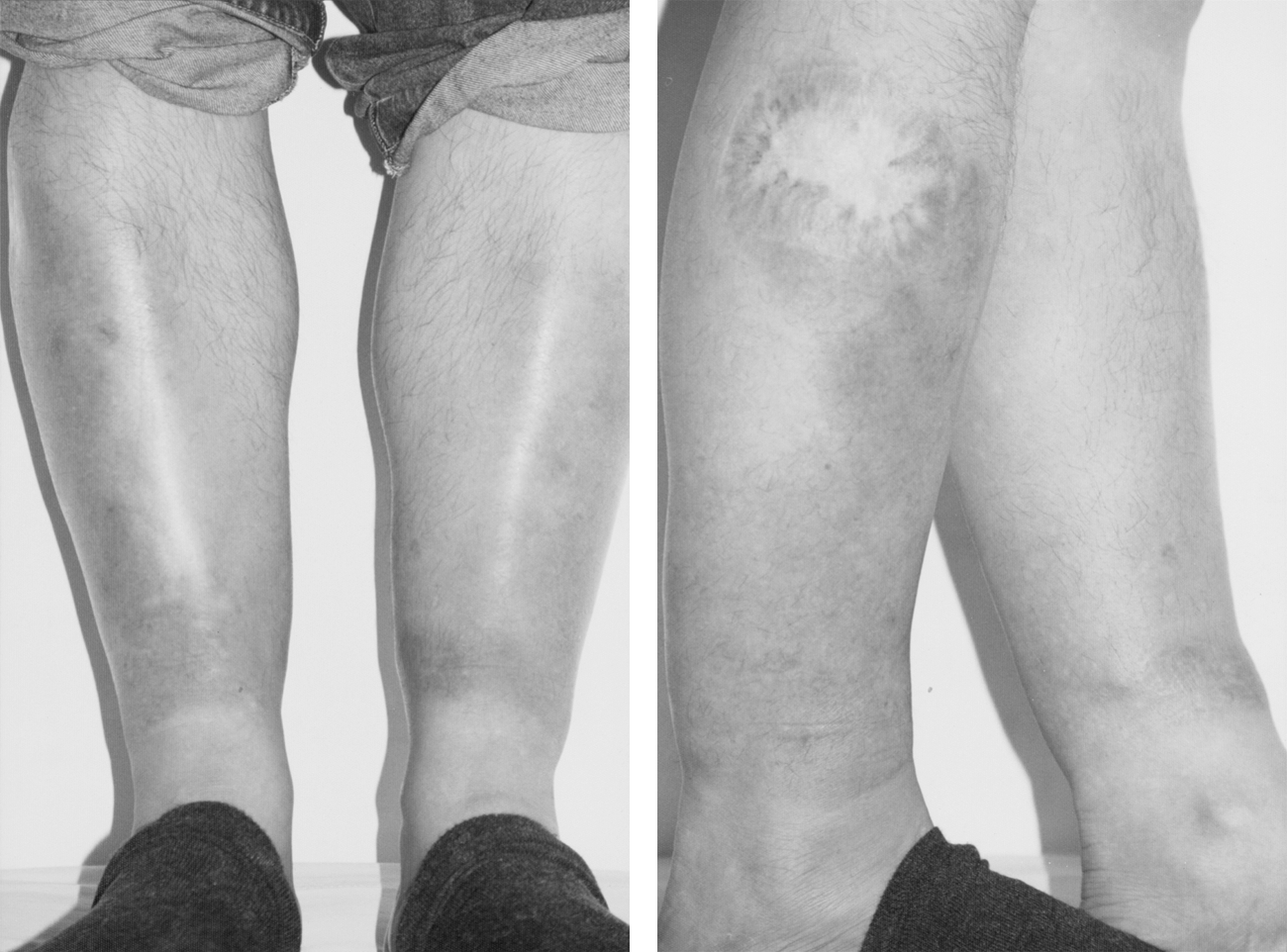
Physical examination revealed mildly prominent eyes, diffusely enlarged thyroid glands, grade 2 without bruits, and PM of both lower extremities (Fig. 1). Laboratory evaluation showed a low serum concentration of thyroid-stimulating hormone (0.005 mIU/L vs. normal value 0.27–4.2 mIU/L), a high level of serum free triiodothyronine (16.71 pmol/L vs. normal value 2.8–7.1), and a high level of free thyroxine (39.58 pmol/L vs. normal value 12–22). Biopsy specimens from the pretibial skin showed large amounts of mucin-like substances in the reticular dermis, confirming the diagnosis of PM.

The patient's lower extremities with pretibial myxedema before therapy. Color images available online at
The patient was treated with multipoint subcutaneous injections of triamcinolone acetonide once every 25–28 days. For each treatment session, a total volume of 1 mL was administered in 10 multipoint injections at a concentration of 40 mg/mL triamcinolone. The injections were started from the borderline of the lesions in both legs and then moved to the other parts of the skin lesions in subsequent courses of treatment. The depth of needle insertion was 0.5–1.0 cm, depending on the thickness of the lesion for the sake of obtaining an optimal position of the skin. The skin surrounding the injection points became soft, thin, and almost normal in color at 10–14 days after the first injection. As the treatment courses were continued, the area of the lesions gradually became smaller. After a 6-month period of treatment of seven courses with a total dosage of 280 mg triamcinolone acetonide for both legs, there was complete remission of PM in both lower extremities. There were no adverse effects from the use of the corticosteroid (Fig. 2). During this triamcinolone treatment, the patient was also treated with 30 mg methimazole (thiamazole) daily for thyrotoxicosis. As his Graves' ophthalmopathy was mild, we administered glucosidorum tripterygll totorum, a traditional Chinese medication for regulation of immune system. The patient's Graves' ophthalmopathy remained stable.
Pretibial myxedema was completely cured after therapy for 6 months.
Discussion
PM, together with ophthalmopathy and acropachy, is an extrathyroidal manifestation of GD. It occurs most commonly in the lower third of the pretibial region, although it can also involve the feet, toes, knees, upper extremities, or even the face. Ninety percent of patients with PM have hyperthyroidism, and the other 10% may either have hypothyroidism or be euthyroid (1). The pathogenesis of PM is unclear but there appear to be interactions of immunologic, cellular, and mechanical processes (2). The thyroid-stimulating hormone receptors existing in the connective tissue are attacked by thyroid-stimulating autoantibodies, inducing immune activation mediated by T lymphocytes (3). Pathologic evaluation of biopsies from the lesion show large amounts of glycosaminoglycans in the reticular dermis (4), but collagen fibers are frayed and reduced (5).
Most lesions of PM are asymptomatic or simply cause cosmetic problems and may resolve in several years without special treatment. But severe cases may be complicated by functional impairment and affect daily activities, in which case an effective treatment is needed. The treatments employed have included management of risk factors and thyroid dysfunction, local corticosteroid therapy, management of ophthalmopathy, systemic immunomodulation, octreotide therapy, compressive therapy, and surgery (6).
Most previous studies advocated the external use of glucocorticoids, with the lesion covered with a plastic film to achieve more efficacy (1,7 –9). There is a recent study reporting a 32-year-old man of PM being treated by subcutaneous injection of triamcinolone acetonide at a large dose (10 mL, 5 mg/mL) monthly (10). Clobetasol ropionate occlusions during the day and elastic bandages at night were regularly applied during the therapy period. As the lesion of PM is usually thick and hard, it is very difficult to apply subcutaneous injection. Our practice of using multipoint injections to obtain a high concentration of corticosteroids may offer a method to overcome this problem. In addition, the once-a-month treatment course can be administered on an outpatient basis, which is more convenient and more acceptable for patients. The therapeutic outcome in our patient demonstrated that this method may be curative with minimum adverse effects.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.