
Abstract
Background:
Patients with progressive refractory thyroid cancer are potential candidates for clinical trials using tyrosine kinase inhibitors (TKIs), and a promising proportion of patients in these trials have achieved stable disease. Here we report an unusual adverse experience in a patient receiving a combination of TKIs.
Summary:
The patient was a 62-year-old man with chronic myloid leukemia (CML) and thyroid carcinoma that did not concentrate iodide and had metastases. He was started on imatinib for his CML. About 5 months later he was started on sorafenib for his thyroid cancer. At this time he had no risk factors for cardiac disease except moderate obesity. He had a complete cytogenetic response in his CML, and a partial response in his thyroid cancer. Twenty-one months after starting the combination of TKIs, he manifested signs of coronary artery disease. He received a combination of medications and his TKIs were continued. He died of a sudden myocardial infarction with cardiogenic shock 28 months after starting the combination of TKIs. A retrospective analysis of sequential 18-fludeoxyglucose positron emission tomography scans (18-FDG PET scans) were indicative of cardiac toxicity developing during the period of concomitant administration of TKIs.
Conclusion:
We report the first case of apparent lethal cardiotoxicity with imatinib-sorafenib combined therapy. Combination TKI treatment may enhance the risk of adverse effects. Our experience with this patient suggests that cardiac PET scan should be monitored closely in these type of patients.
Patient
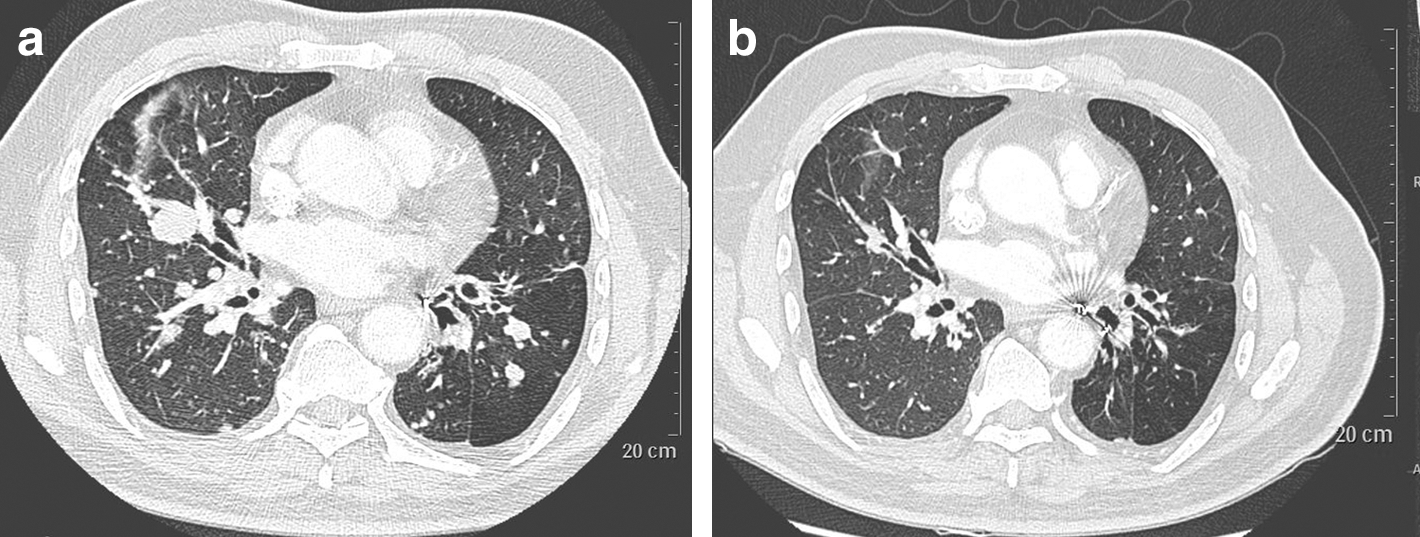
Computed tomography (CT) scan evaluation of lung metastasis of the thyroid cancer. The sequential CT scans performed at the beginning of the combination of imatinib and sorafenib
In July 2009, 21 months after he started this combination of imatinib and sorafenib, the patient developed a de novo acute coronary syndrome without ST elevation on electrocardiogram (EKG). EKG showed left anterior hemiblock, without repolarization abnormalities. Laboratory findings revealed elevated levels of troponin I (56 μg/L), and creatine-kinase MB (660 UI/L), and the coronary angiography disclosed a tritruncal stenotic coronary atheroma with subcoronary occlusion of the distal left circumflex. Echocardiography showed a moderate left ventricular hypertrophy, without segmental kinetic changes. It was decided not to do angioplasty or surgery because of the tritruncal stenosis with a poor vascular bed distal to the lesions and his poor prognosis related to thyroid cancer. His median progression-free survival was considered to range from 14 to 21 months based on phase II studies (4 –6). He was started on daily doses of clopidogrel 75 mg, atenolol 50 mg, perindopril 2 mg, atorvastatin 80 mg, and acetylsalicylate 75 mg for his cardiac disease. In the next 7 months coronary angiography was not repeated because of absence of new cardiac symptoms.
Seven months later, in February 2010, while the patient was undergoing a 18-fludeoxyglucose positron emission tomography scan (18-FDG PET scan) for evaluation of the thyroid cancer, he suffered acute thoracic pain. Despite an immediate transfer into the intensive care unit, he developed an extensive anterior acute myocardial infarction with cardiogenic shock and died 1 hour later.
His last 18-FDG PET scan indicated major left ventricular dilatation and lack of 18-FDG captation (Fig. 2c). Retrospectively, we found on the related 18-FDG PET images obtained in November 2008 (12 months after the beginning of the combined therapy and 8 months before the first clinical acute coronary syndrome) a de novo lack of 18-FDG captation in the apical and med-septal regions (arrows) corresponding to the territory of the left anterior descending artery (Fig. 2b), which was not seen on the normal imaging before tyrosine kinase inhibitor (TKI) therapy (Fig. 2a).

Short axis, vertical long axis, and horizontal long axis sequential images of cardiac 18-FDG positron emission tomography (18-FDG PET) scan. Normal myocardial metabolism before combined imatinib and sorafenib treatment
Discussion
Imatinib and sorafenib are orally administered inhibitors of receptor tyrosine-kinases, mainly platelet-derived growth factor receptor, and c-kit receptor for imatinib, BRAF, VEGF receptor 1,2, and c-kit receptor for sorafenib. In three recent phase II studies of patients with metastatic refractory thyroid cancers, sorafenib demonstrated promising clinical activity (4 –6). TKIs have been associated with cardiac toxicity, usually reversible and not severe, as the incidence of cardiotoxic mortality ranges between 1% and 3% (7). However, with expanded clinical experience, the incidence of cardiac events could be higher than previously reported (8). Imatinib may lead to severe left ventricular dysfunction with congestive heart failure, due to alterations in mitochondria function and cardiomyocytes apoptosis (9). In the TARGET study, acute coronary syndromes, including myocardial infarction, were observed in 3% of patients in the sorafenib arm compared to <1% in the placebo arm (10). A central role of RAF1 and BRAF inhibition has been proposed (7), but recent data suggest that mechanisms of sorafenib-induced cardiotoxicity might be due to inhibition of combinations of kinases different than RAF1 or BRAF (11). Interestingly, targeting c-kit with both imatinib and sorafenib might interfere with cardiac repair after myocardial infarction (12). There has been recent interest in using combinations of TKIs to minimize the possibility of resistance to their anti-neoplastic effects. However, the use of new combinations of TKIs is challenging because of the possibility of synergism as far as adverse events are concerned (13). Here we reported a first case of possible cumulative and lethal cardiac toxicity in a patient treated for a prolonged period with imatinib and sorafenib. To our knowledge, there is no other reported case of severe cardiac toxicity with a combination of TKIs.
18-FDG PET scan is a promising tool to evaluate tumor response to new drugs such as those that target the VEGF pathway (14). However, cardiac PET scan analysis is not usually performed in patients being treated with TKIs for advanced disease in oncology since cardiac uptake with FDG imaging is considered as physiological and therefore without clinical relevance.
In retrospect, cardiac PET scan analysis should have been performed at the same time as that the whole-body PET scan was interpreted in our patient. Indeed, in our patient, cardiac PET scan was probably predictive of cardiac toxicity since an 18-FDG defect in the territory of left anterior descending artery appeared 8 months before the first coronary symptoms.
There are new imaging strategies to assess cardiac status, including quantitative gated 18-FDG PET, when ischemic heart disease is suspected. These procedures can be used in patients with left ventricle dilatation to assess global impairment of myocardial metabolism, but require specific cardiac protocols (15). To date, there is no study assessing the predictive value of sequential cardiac PET scans in patients receiving cardiotoxic chemotherapeutic agents. Potentially useful information is likely to be that related to vascular uptake. In patients being treated for cancer it has been shown that increased 18-FDG uptake in major arteries as well as calcified plaques in the same vessels could be predictive of a subsequent vascular event (16). We did not observe any similar images in our patient.
Conclusion
Systematic cardiac follow-up should be considered for patients receiving long-term treatment with TKI monotherapy or combinations of TKIs. If a whole-body 18-FDG PET scan is performed, cardiac PET scan analysis could be taken into account to help in the prediction and management of TKI-related cardiotoxicity.
There is a need for developing a protocol that may be applied to those patients undergoing an oncology PET scan study; this would permit a systematic observation of the myocardial metabolic status. A prospective study is necessary for evaluating the role of cardiac reading when performing oncology FDG-PET/computed tomography, especially in patients at high risk of developing cardiac disease secondary to oncologic drug use. Strict follow-up is required in patients receiving TKIs for oncological diseases.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.