
Abstract
Cardiac metastasis from epithelial thyroid cancer is a very rare and potentially serious complication. We have identified only 54 reported cases over a 130-year period. Here we review this literature. Cardiac metastases are frequently asymptomatic, but when symptoms develop these tend to be severe and often fatal. The prognosis of cardiac metastases from thyroid cancer is unclear as survival data are often missing or absent in reported cases. However, as many patients died suddenly from cardiac complications, the prognosis seems poor. Of those patients who survived, all underwent surgical intervention. Trans-thoracic echocardiography is the diagnostic modality of choice as it allows dynamic evaluation of intracardiac masses. Metastatic involvement of the heart from thyroid cancer is uncommon. Left untreated this complication seems likely to be fatal. Therefore, in patients with established thyroid malignancy who develop cardiac arrhythmias, new murmurs, or signs of cardiac decompensation, we suggest that cardiac metastases be considered. Echocardiography should be performed in patients with advanced thyroid cancer and cardiac symptoms or signs. If a cardiac metastasis is present, we recommend surgical intervention if possible.
Introduction
Autopsy studies of patients with thyroid cancer have documented a frequency of cardiac metastasis of 0%–2% (5 –7). From an extensive literature search, we identified 54 cases of cardiac metastasis from thyroid cancer over a 130-year period (Table 1), with the most common histological type being anaplastic thyroid carcinoma, closely followed by FTC including Hurthle cell carcinoma, papillary thyroid carcinoma (PTC), and adenocarcinoma. The remaining cases of cardiac metastasis from thyroid cancer were from medullary carcinoma, clear cell carcinoma, well-differentiated carcinoma, and undifferentiated or poorly differentiated carcinoma. During our literature search we also discovered an additional 20 cases of thyroid cancer involving the heart through direct tumor invasion, mostly via the venous system (Table 2). In this instance, FTC represented the most common tumor type, followed by PTC.
U, unknown; HD, hematogenous dissemination; LD, lymphatic dissemination; RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle; TV, tricuspid valve; ATC, anaplastic thyroid cancer; FTC, follicular thyroid cancer; PTC, papillary thyroid cancer; VT, ventricular tachycardia; TTE, transthoracic echocardiogram; CT, computerized tomography; MRI, magnetic resonance imaging; PET, positron emission topography; HF, heart failure; TOE, transesophageal echocardiogram; SVC, superior vena cava; 90Y-Dotatoc, yttrium-90-DOTA-tyr3-octreotide; CCF, congestive cardiac failure; DIC, disseminated intravascular coagulation; MNG, multinodular goiter; WBS, whole body scan; XRT, external beam radiotherapy; VF, ventricular fibrillation; LVF, left ventricular failure.
LI, local intravascular invasion; LE, local extravascular invasion; SVCS, SVC syndrome (e.g., dyspnoea, dysphagia, suffocation, facial edema and cyanosis, superficial neck vein dilatation); IJV, internal jugular vein; SCV, subclavian vein; PA, pulmonary artery; IVC, inferior vena cava; MTC, medullary thyroid cancer; ATC, anaplastic thyroid cancer; HTC, Hurthle cell thyroid cancer.
Mathieu published the first reported case of thyroid carcinoma with cardiac metastasis in 1881 [cited in ref. (8)]. The most recent reports of cardiac metastasis from thyroid cancer include two cases of medullary thyroid carcinoma (MTC) by Bertagna et al. (9) and Morel et al. (10). Giuffrida and Gharib (5) reviewed the literature in 2001. We have performed an extensive and updated review of the literature.
Methodology
We identified a total of 74 cases of cardiac involvement from thyroid cancer in the international literature over the last 130 years. We used the databases Medline and PubMed to conduct our search using the following search terms: thyroid cancer or carcinoma, cardiac or heart, metastases or secondary or secondaries or neoplasms. We have also included case reports referenced in other publications. Of the 74 cases, 54 were considered as true metastases based on the description of cardiac and great vessel involvement, and are presented in Table 1 (5,8 –42). The remaining 20 cases presented in Table 2 (8,43 –53) involved the heart by direct extension and therefore were not considered metastatic in nature. Of the 54 case reports of cardiac metastases from thyroid cancer, nine articles including abstracts were in foreign languages, and four articles were in foreign languages with English abstracts. For the purpose of our review we chose to include all identified cases in the tables, but have limited our discussion to those articles written in English.
Epidemiology
Although more frequent than primary cardiac tumors, metastatic involvement of the heart from any cancer is uncommon (54,55). The most common primary cancer to metastasize to the heart is malignant melanoma, affecting the heart in more than 50% of cases in autopsy series (56,57). Various other tumors are typically associated with cardiac involvement and include breast and lung carcinoma, soft tissue sarcomas, renal carcinoma, esophageal carcinoma, hepatocellular carcinoma, and hematological malignancies such as lymphoma and leukemia (6,7).
Although the prevalence of cardiac metastases from thyroid cancer is difficult to ascertain, three case series provide relevant data. In a Swedish autopsy series of 10,160 cases by Berge and Sievers (11), 5% of metastatic carcinomas involving the myocardium originated in the thyroid. A retrospective study of 2107 consecutive adult autopsies by Kline (14) from 1950 to 1965 revealed 716 with malignant disease, with 36 metastatic tumors involving the myocardium, and one of these arising in the thyroid. Finally, in a case series by Pomorski and Bartos (37) from 1974 to 1998, one case of 975 thyroid malignancies involved the heart, representing a prevalence of 0.1% in this cohort.
Pathogenesis and Anatomy
Cardiac involvement from a thyroid neoplasm can arise from three mechanisms: (i) hematogenous dissemination, (ii) lymphatic dissemination, and (iii) local extension that may be intravascular or extravascular in nature. With intravascular local extension, right-sided cardiac chambers may be filled by tumor reaching them by direct extension through the thyroid veins via the superior vena cava (SVC), representing tumor thrombus. Extravascular local extension is cardiac involvement as a result of tumor directly invading extravascular tissues, such as adjacent organs or adipose tissue. Hematogenous dissemination and local intravascular extension is more commonly observed in FTC where there is a tendency toward angioinvasion and venous metastasization (30). Conversely, PTC tends to invade locally and disseminates by lymphatic vessels of the neck and upper mediastinum (30). Hematogenous and lymphatic dissemination reflect true metastatic involvement, whereas local extension describes extension of a primary tumor to a distant site and therefore is not strictly metastatic in character. This is an important distinction as while we identified 74 cases of thyroid cancer with cardiac involvement, only 54 cases may be considered truly metastatic. Eighteen cases described involvement of the heart by local intravascular extension of tumor thrombus from thyroid veins to the SVC, and two cases involved local extravascular extension of tumor from the left lower lobe of the lung into the left atrium.
Hirnle et al. (33) published the first case of malignancy in possible ectopic thyroid tissue in the heart (struma cordis). A 55-year-old woman is described who, 10 years after subtotal thyroidectomy for follicular adenoma, was found to have a follicular carcinoma in the right ventricle. While the authors acknowledge that distinguishing carcinoma arising in ectopic thyroid tissue from metastatic carcinoma is difficult, they suggest development of carcinoma in ectopic thyroid, rather than metastasis occurred in their patient. As the authors could not exclude the possibility of metastatic thyroid cancer to the heart, we have chosen to include it in our total number of cases.
The typical sites for cardiac metastases are the pericardium, epicardium, and the right side of the heart, with the endocardium, myocardium, and the left side of the heart far less commonly affected (54,58), as in our patient. Well over half of the cases reported cardiac metastases only involving the right side of the heart with a few of these also affecting the myocardium and pericardium. The next most common site of involvement was the pericardium with eight cases of sole pericardial involvement (8,18,19,22,30,32,35,41): five presenting with pericardial effusions. Other than pericardial effusion, pericardial thickening and nodular deposits may be associated with thyroid carcinoma (35). Only three cases reported both right- and left-sided heart involvement (8,36), and there was one case of thrombotic endocarditis of the tricuspid valve (TV) (36). Our literature search found only one case of isolated left-sided heart involvement (15). We identified two other cases of sole left-sided cardiac involvement, which are presented in Table 2, but these were due to local extravascular extension from tumor involving the left lower lobe of the lung, rather than true metastasis (50,51).
Clinical Features
Cardiac tumors may cause symptoms that tend to reflect the site of cardiac involvement rather than the histopathology. Examples include obstruction of circulation resulting in heart failure; interference with valvular function causing regurgitation; direct invasion of the myocardium producing impaired contractility, arrhythmias, heart block, or pericardial effusion; invasion of adjacent structures such as the lung causing pulmonary symptoms; embolization; and constitutional or systemic symptoms (55). Tumor invading intravascularly by extending along the veins and into the heart chambers interferes with venous return. Symptoms and signs in these cases are those of venous obstruction, and typically manifest as SVC syndrome. However, clinical diagnosis is difficult as there are usually no specific symptoms. In fact, metastatic cardiac involvement most often occurs during the terminal stage of disease and is usually diagnosed at autopsy (34).
Of the 54 case reports describing cardiac metastases from thyroid cancer, almost half of patients were asymptomatic and died suddenly, with metastases in the majority only identified at autopsy. Patients with symptoms tended to relate to local tumor recurrence or nonspecific constitutional symptoms of malignancy, such as fatigue. Only a few patients with cardiac metastases actually displayed cardiac symptoms, such as acute cardiac tamponade, cardiac ischemia, and congestive cardiac failure. In these patients, the onset was sudden and associated with serious underlying pathology; at least seven cases died within 1 month of presentation (19,21,27,30,36,39,42). Of the 18 cases of thyroid cancer with cardiac involvement due to local intravascular invasion, 13 of these cases were symptomatic with SVC syndrome.
Diagnosis
Echocardiography represents the first-line imaging modality for the detection and evaluation of cardiac tumors (59). Cardiac involvement in the majority of cases as well as ours (See Illustrative Case) was detected by transthoracic echocardiography, and later often confirmed by further investigations such as computerized tomography (CT), angiography, transesophageal echocardiography, and cytology. Although the echocardiographic characteristics of an intracardiac mass and its associated clinical findings may suggest an etiology, it is often difficult to differentiate thrombi from tumor, and benign from malignant tumors (42). Features on echocardiography to suggest a malignant lesion include right-sided involvement, extension to the heart through the vena cava or pulmonary veins, and intramural masses, commonly in association with intracavity or pericardial extension (42). The most common echocardiographic finding in patients with metastatic cardiac disease is pericardial effusion due to the frequent presence of pericardial seeding (60). While benign masses are unlikely to display these characteristics, no pathognomonic findings of benign or malignant tumors in two-dimensional echocardiography exist (61). Diagnostic evaluation therefore tends to rely upon initial echocardiography then adjunctive CT and magnetic resonance imaging (55). Of interest, in a case of right ventricular metastasis Moustafa et al. (42) demonstrated that contrast echocardiography perfusion imaging can be used to evaluate the vascularity of a mass, subsequently providing additional information to differentiate malignant lesions from benign tumors and thrombi. Therefore, if available, this imaging modality may also be considered in the assessment of intra-cardiac masses.
Whole body radioiodine scanning and serum thyroglobulin (Tg) are unreliable markers of metastatic disease due to high rates of non-iodine avid tissue and non-Tg-producing tumors, as in our patient (See Below) and many of the other documented cases. Of the few cases that recorded serum Tg levels, three had raised levels (27,29,33). Serum Tg levels were normal in the cases published by Fukuda et al. (39) and Kim et al. (38). The majority of published cases did not record results of radioiodine scanning, so it is unclear how many tumors were also non-iodine avid.
Prognosis
For all cardiac tumors, size and locality influence prognosis. For metastatic cardiac tumors, the prognosis is dependent on the histological tumor type (55). Given the rarity, the prognosis of metastatic cardiac disease arising from primary thyroid malignancy is unclear. The average length of survival of patients from the reviewed 54 cases, where stated, was 12.5 weeks. This is of very limited value, however, as survival data were incomplete or indeed absent in many of the reported cases. Nevertheless, it can be stated that at least 15 patients of the 54 cases with cardiac metastases secondary to thyroid cancer died within 3 months of presentation, with a substantial number dying suddenly from cardiac complications, including acute left ventricular failure, acute myocardial ischemia, and arrhythmias. Therefore, the prognosis of cardiac metastases from thyroid cancer is very likely to be poor.
Treatment
The mode of treatment for cardiac tumors in general varies according to the type, location, and extent of tumor, as well as symptoms. Observation may be sufficient when the mass is small, benign, and does not interfere with vascular hemodynamics (16). However, resection is necessary when there is hemodynamic compromise, large tumor burden, or significant symptoms (16,62). Medical management focuses on control of symptoms and possible complications, such as arrhythmia, thromboembolism, and congestive heart failure (16). All of the previously documented cases of cardiac metastases from primary thyroid cancers who survived, at least in the short term, underwent surgery (31,33,35,40,49). Therefore, based on these results, we recommend surgical resection of cardiac metastases from thyroid cancer in patients who are considered fit for surgery.
Illustrative Case
A 57-year-old woman with metastatic non-iodine avid poorly differentiated thyroid cancer was admitted for further assessment of an incidental large right atrial mass detected on a screening echocardiogram performed for entry into a clinical trial of a vascular endothelial growth factor/tyrosine kinase inhibitor.
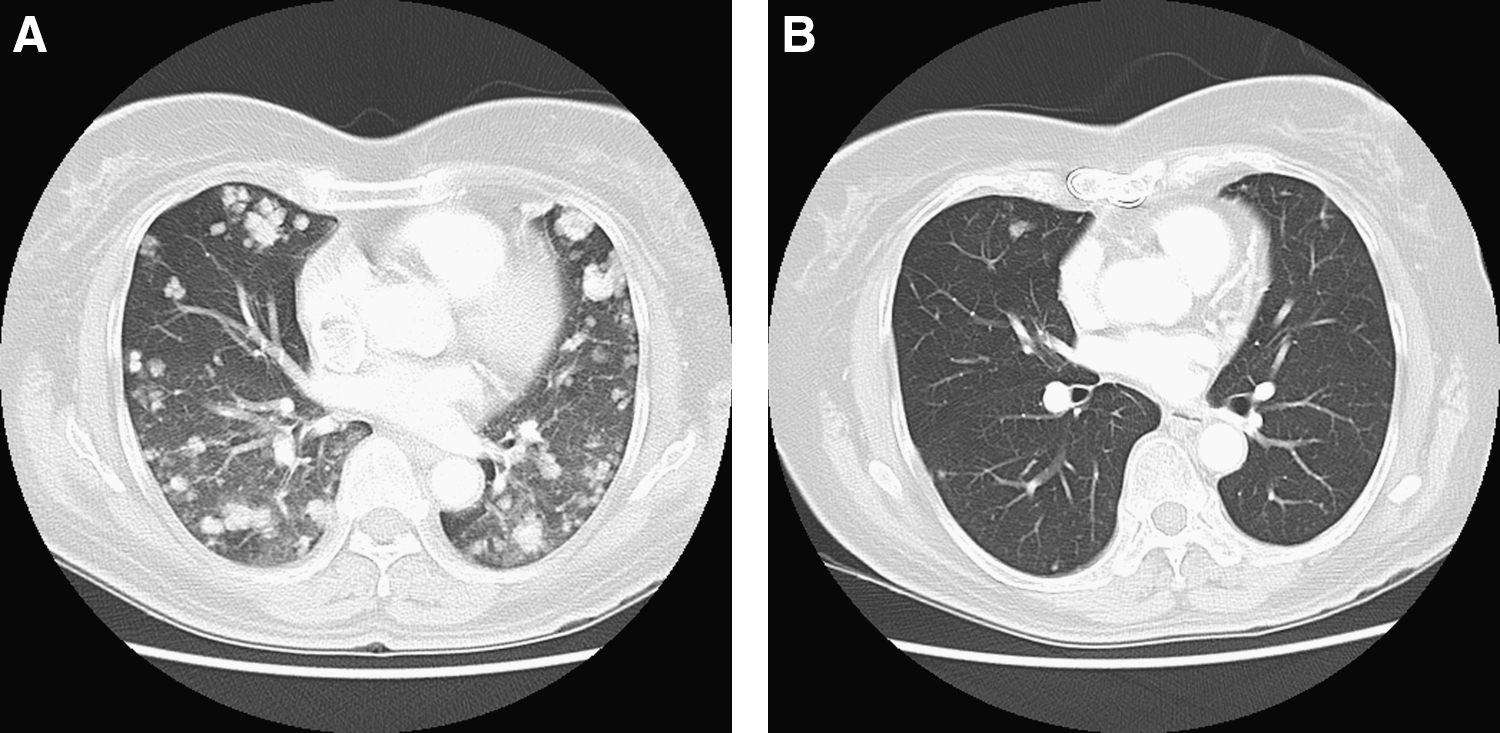
Poorly differentiated thyroid carcinoma (WHO histological classification 8020/3) with a follicular appearance was diagnosed 4 years before in late 2006. Treatment included total thyroidectomy and level VI lymph node dissection, followed by radioactive iodine ablation and external beam radiotherapy to the neck. One year later diagnostic whole body radioiodine scanning was clear of iodine avid tissue, but chest CT showed multiple pulmonary nodules consistent with metastases. Progressive enlargement of these pulmonary nodules shown on chest CT prompted evaluation for entry into a clinical trial for metastatic epithelial thyroid cancer in late 2009 (Fig. 1a).
Medical history included Graves' disease, originally diagnosed in 1996 and successfully treated with carbimazole and radioactive iodine; Sjogren's syndrome complicated by salivary gland calculi; and allergic rhinitis.
Our patient had no constitutional symptoms but reported some exertional dyspnea, and two minor episodes of hemoptysis. There was no arrhythmia, cardiac failure, SVC obstruction or tricuspid regurgitation, or evidence of pulmonary emboli although in retrospect, the episodes of hemoptysis may have been due to small tumor pulmonary emboli.
Transthoracic echocardiography demonstrated a 6.2 × 1.9 cm mobile multilobular mass seemingly attached to the TV and associated with mild to moderate tricuspid regurgitation (Fig. 2). Ventricular size and function were preserved. A Tc-99m methylene diphosphonate bone scan performed at the time of echocardiography did not reveal any scintigraphic evidence of osseous metastases. Serum Tg was modestly raised at 10.1 μg/L. An ECG was unremarkable. Cardiac magnetic resonance imaging demonstrated a large well-defined mass in the right atrium (RA) that extended into the SVC and right brachiocephalic vein, prolapsing through the TV into the right ventricle during atrial systole (Fig. 3). Valvular function, biventricular size and systolic function, as well as biatrial size were normal.
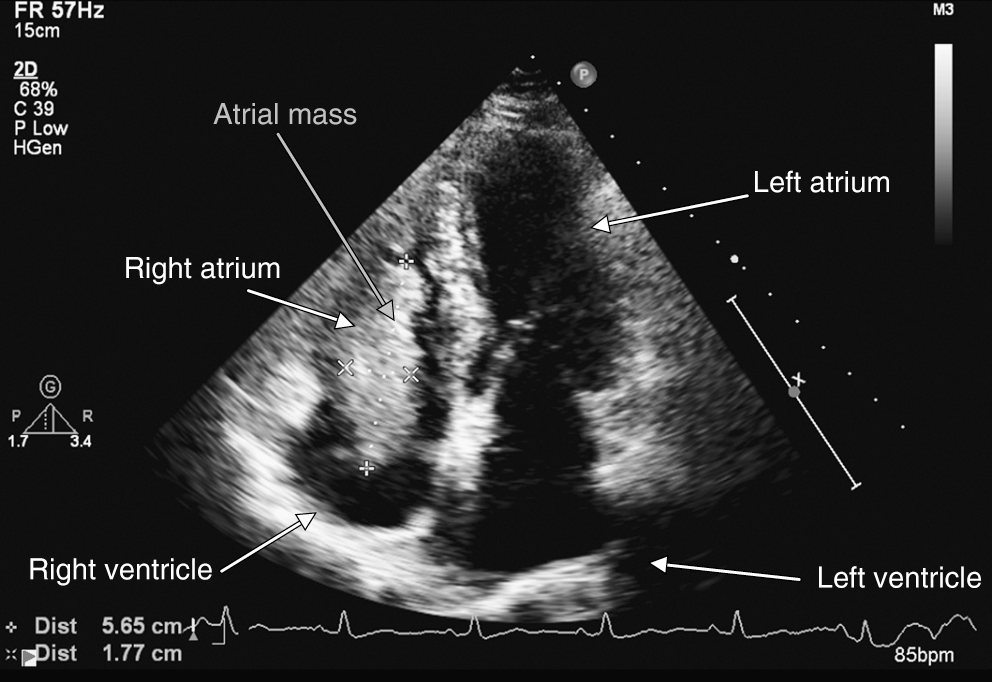
Transthoracic echocardiogram during screening process for entry into clinical trial (5/11/09). Four-chamber view demonstrating a large (6.2 × 1.9 cm) mobile multilobular mass in the right atrium prolapsing through the tricuspid valve into the right ventricle. Normal biventricular size and function.
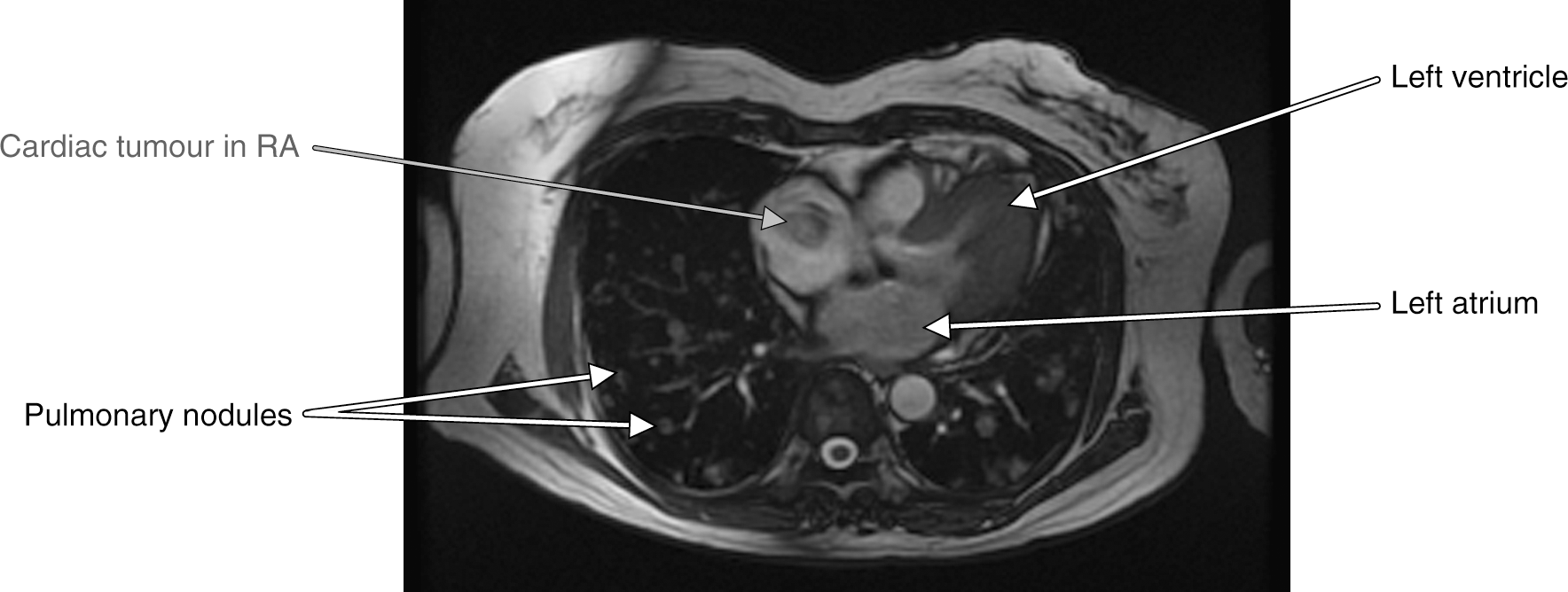
Cardiac magnetic resonance imaging of incidental atrial tumor (10/11/09). Reveals a large, well-defined mass in the RA. Extensive pulmonary nodules also apparent. RA, right atrium.
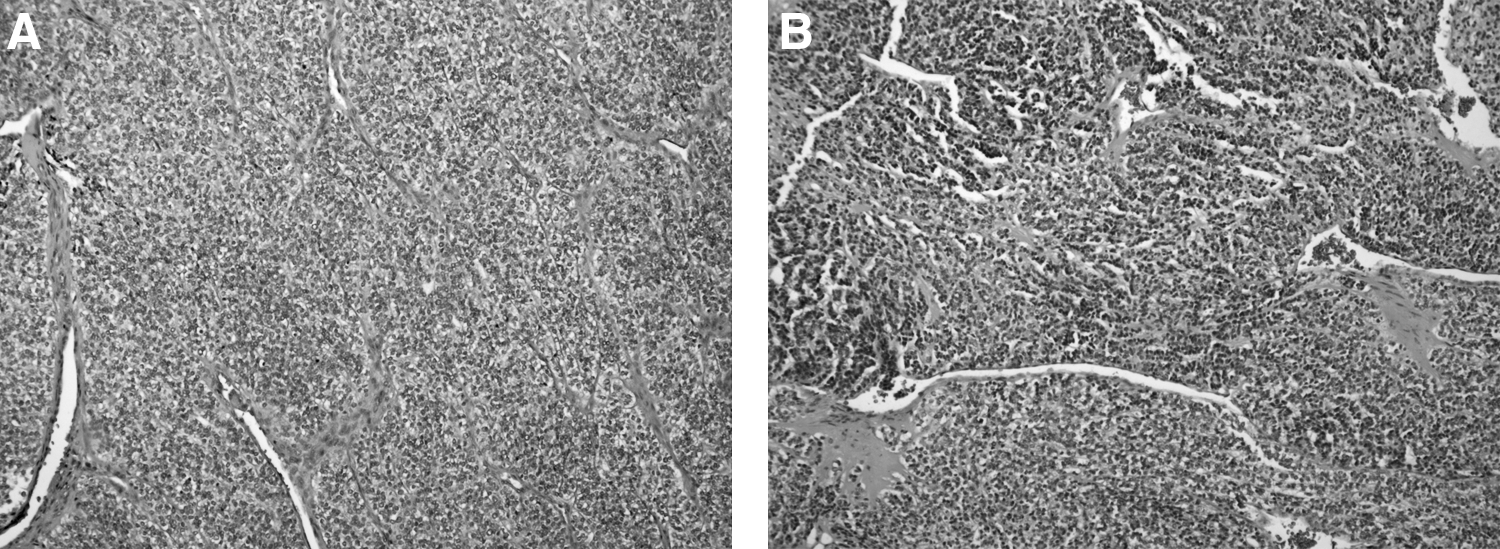
Upon excision via sternotomy, the mass measured 6.2 × 1.7 cm and arose from the junction of the RA and SVC. It extended 2 cm proximally into the SVC, traversed the RA, and prolapsed through the TV. Most of the mass was excised with a residual section remaining at the junction of the SVC and RA. The histopathology revealed a poorly differentiated carcinoma of thyroid origin (Fig. 4b). Both the primary (Fig. 4a) and metastatic tumors displayed identical cell architecture on hematoxylin and eosin staining, and also stained for thyroid transcription factor 1 and Tg. Given the absence of either thyroid bed recurrence or regional lymphadenopathy, the cardiac tumor was considered a distant site of metastasis, rather than local invasion.
Our patient recovered well postoperatively, and after 6 months on trial therapy made a dramatic improvement with chest CT demonstrating a marked reduction in the size and number of pulmonary nodules (Fig. 1b), maintained so far at 12 months on trial therapy.
Conclusion
In patients with established thyroid malignancy, particularly FTC, who develop cardiac arrhythmias, new murmurs, or signs of cardiac decompensation, it is essential that cardiac metastases be considered. As cardiac involvement is extremely rare, routine echocardiographic screening in metastatic thyroid cancer is unwarranted, but in our case, fortuitous early detection by echocardiography facilitated surgical resection and allowed entry into an experimental vascular endothelial growth factor/tyrosine kinase inhibitor drug trial program. The good result so far suggests that this therapy may be worthwhile, but more extensive study is required.
Afterword
Since submission of this manuscript, we have found two further reports which are noteworthy. Mizukami et al. (63) described four cases of pericardial metastases in patients of unspecified age or type of differentiated thyroid carcinoma. Eichfeld et al. (64) described one case of cardiac metastasis from FTC in a patient of unknown age. Neither of these reports included descriptions of serum Tg, treatment, or outcome.
Footnotes
Acknowledgment
We thank the Departments of Diagnostic Radiology and Cardiology, Alfred Health, for cardiac imaging.
Disclosure Statement
The authors declare that no competing financial or other interests exist.