
Abstract
Background:
Treatment of Graves' disease during pregnancy with antithyroid drugs (ATDs) poses a risk of inducing hypothyroidism and, thus, development of a goiter to the fetus.
Patient Findings:
We report two patients referred to our department after discovery of a fetal goiter by ultrasound examination in the second trimester of pregnancy. The women receiving 400 mg/day propylthiouracil and 10 mg/day thiamizole, respectively, had thyrotropin and total thyroxine values within the normal reference range but a lowered free thyroxine level. Fetal blood sampling by cordocentesis revealed severe fetal hypothyroidism as the cause of goiter development. Reduction of maternal ATD dose and injection of levothyroxine intra-amniotically quickly reduced the goiter size, and both babies were born euthyroid and without goiters.
Summary:
Two pregnant women with Graves' disease were overtreated with ATDs inducing iatrogenic goiter in the fetuses. Successful treatment with intra-amniotic levothyroxine injections rendered the babies euthyroid and nongoitrous at birth.
Conclusions:
Correct interpretation of thyroid function tests during pregnancy in general—and during ATD therapy of Graves' disease in particular—is difficult. Awareness of pregnancy-related changes in maternal thyroid status, and a close teamwork among endocrinologists, obstetricians, and experts in fetal medicine, is pivotal in ensuring normal growth and development of the unborn child of these patients.
Introduction
According to recent guidelines, pregnant women with Graves' disease should be treated with antithyroid drugs (ATDs), preferably propylthiouracil (PTU), risking surgery only in case of severe adverse effects of the drugs (8). PTU rather than imidazole derivatives is recommended during pregnancy due to the possible teratogenicity of the latter (i.e., aplasia cutis) (9 –12). However, reports of severe side effects of PTU, acute liver failure being one of them, have recently led to a warning on the use of PTU from the American Food and Drug Administration (13) and have spurred a debate on a revision of the current guidelines—some suggesting the use of PTU in the first trimester (when organogenisis occurs) and a switch to imidazole derivatives from the second trimester onward (14,15). Nevertheless, treatment of maternal hyperthyroidism during pregnancy is important. Untreated maternal hyperthyroidism has been associated with a higher risk of preeclampsia, congestive heart failure, fetal mortality, small-for-gestational-age infants, and thyroid storm—the risk increasing with maternal autoantibody levels (16 –18). The prevalence of hyperthyroidism in pregnancy is reported to be as high as 0.4% [not including gestational transient thyrotoxicosis, which is much more common (19)]. Approximately 90% of the cases are of autoimmune etiology, that is, Graves' disease (20).
ATDs given to the mother can pass to the fetus and exert their effect by blocking thyroid peroxidase activity and peripheral deiodination with risk of developing fetal hypothyroidism and goiter (Fig. 1). Before the onset of fetal thyroid function in mid-gestation, there is no need to assume any direct effect of PTU (iodide uptake and colloid formation begin as early as the 11th week postconception) (21). Fetal PTU clearance has been shown to be slower than the maternal PTU clearance, and the fetus is as such at risk of developing iatrogenic hypothyroidism (22). Therefore, it is of utmost importance to monitor both the thyroid status of the pregnant woman and the fetal development to prevent such incidences. Further, monitoring of maternal liver status is important when initiating treatment with PTU.
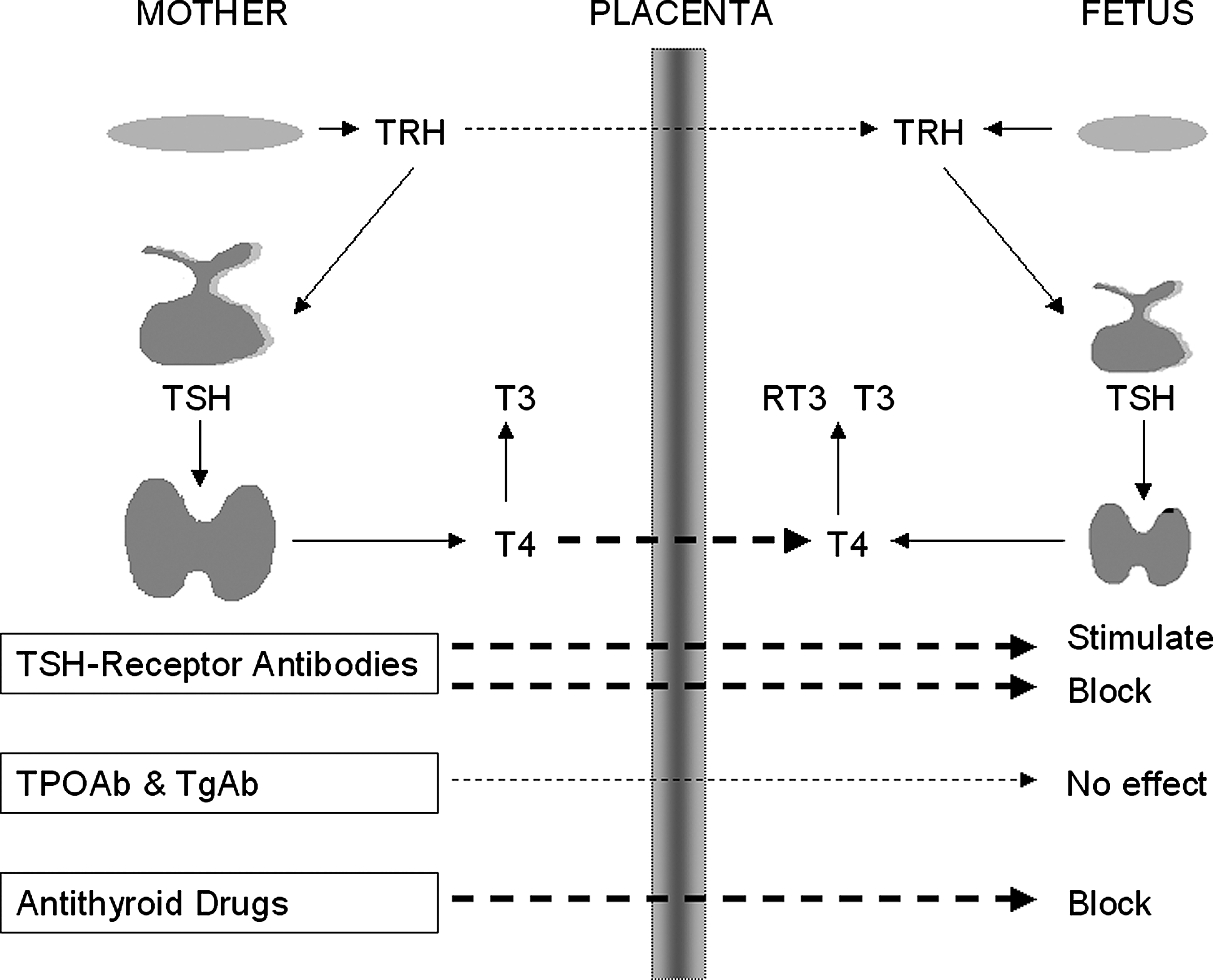
Maternal-fetal exchange. Several maternal circulating factors affect the fetus by transfer across the placenta. Deiodinases in the placenta prevent fetal thyrotoxicosis by allowing only a small, but physiologically significant, amount of thyroxine to pass. In pregnant women suffering from Graves' disease, TSH receptor antibodies pass freely to the fetus to exert their effect once the fetal thyroid becomes functional. Further, antithyroid drugs given to the mother will affect the fetus as well. RT3, reverse triiodothyronine; T3, triiodothyronine; T4, thyroxine; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TRH, thyroid-releasing hormone; TSH, thyroid-stimulating hormone.
To comprehend laboratory results, one must be aware of the changes occurring to maternal thyroid status during pregnancy, thereby leading to naturally suppressed thyrotropin (TSH) levels, elevated total thyroxine (T4) levels, and suppressed autoimmune activity—hence less need of ATDs as pregnancy progresses (23,24). This further increases the risk of overtreatment with ATDs.
We report two incidences of fetal goiter formation due to overtreatment of maternal Graves' disease with ATDs that were successfully treated with intra-amniotic levothyroxine injections.
Patients
Patient 1
A 29-year-old woman in her second pregnancy, week 23 + 6, had been treated for Graves' disease with ATDs regularly for 16 years. She had a son from the first pregnancy who was born with neonatal hypothyroidism and goiter (maternal treatment with PTU 400 mg/day had been started in the first trimester); the child quickly became euthyroid on levothyroxine and required no further treatment, suggesting that the goiter might have been induced by maternal PTU treatment.
The woman was referred to our antenatal unit after discovery of a possible goiter at an antenatal ultrasound examination (week 19 + 4) at another hospital. When referred to us, maternal actual dose of PTU was 4 × 100 mg daily. Maternal serum TSH was 2.3 mU/L (0.27–4.20), total T4 89 nmol/L (60–150), and free T4 (FT4) 8.5 pmol/L (12.0–22.0) (Table 1) (see Table 2 for conversion factors).
Patients 1 and 2 both suffering from Graves' disease were referred to our patient clinic after discovery of a fetal goiter at routine antenatal ultrasonography examination at a local hospital. Laboratory test results indicated maternal hypothyroidism (TSH within the normal reference range, but fT4 below). Fetal blood sampling showed severe fetal hypothyroidism. Reduction or discontinuation of maternal antithyroid drug dose and intra-amniotic levothyroxine injections quickly reduced the goiter size, and both newborns were euthyroid and goiter free.
Thyroid binding globulin -corrected T4.
Neonatal TSH screening was based on blood sampled 10 days PP due to lack of material from 5 days PP.
(a), amniotic fluid; (c), cord blood; fT4, free thyroxine; GA, gestational age; PP, post partum; PTU, propylthiouracil; TSH, thyroid-stimulating hormone (thyrotropin); tT4, total thyroxine; Week, gestational week.
Fetal ultrasound (week 23 + 6) demonstrated a female fetus with a bilaterally enlarged thyroid gland of 4.3 × 2.0 × 2.4 cm corresponding to a prominent fetal goiter. The thyroid gland had a homogenously echogenic texture and a high flow. There was no hyperextension of the fetal neck; however, there was an increased amount of amniotic fluid suggestive of tracheal compression. Fetal heart rate (140 beats per minute) and intrauterine growth were normal. The fetal thyroid function was evaluated by cordocentesis, which revealed severe fetal hypothyroidism with a TSH >200 mU/L (2–12) and FT4 3.4 pmol/L (5.1–27.0) (Table 1) [reference ranges for fetal thyroid status according to Thorpe-Beeston et al. (25)].
Based on these findings, maternal PTU dose was reduced to 100 mg ×3 daily and further reduced during the next couple of weeks to 50 mg/day at gestational week 29 (discontinued at week 39). Further, to hasten the process of goiter reduction, a series of intra-amniotic levothyroxine injections was initiated at gestational week 24 and continued for the next 5 weeks. A sample of amnion fluid was taken before each injection to follow the development in fetal thyroid status. The levothyroxine dose was calculated based on an estimated fetal need of 10 μg/kg/day (Table 1). A total of six intra-amniotic levothyroxine injections was given with doses ranging from 50 to 100 μg.
A reduction of the fetal goiter size was seen week by week, and fetal thyroid status quickly normalized (Table 1). As such, a female child of 4100 g, Apgar score 10 at 1 and 5 minutes, was born by spontaneous, uncomplicated, vaginal delivery at gestational week 40 + 5. No goiter was found at clinical examination, and cord blood analysis showed a euthyroid newborn with normal TSH and FT4 levels (Table 1) and slightly elevated total T4 levels of 158 nmol/L (60–140), TSH receptor antibodies <0.3 IU/L (<1), thyroidperoxidase-antibodies 244 kIU/L (<60), and thyreoglubolin antibodies <10 kIU/L (<60). At follow-up examinations at 6 and 16 months, the girl had met all her developmental milestones.
Patient 2
A 38-year-old woman in her third pregnancy, 24 weeks + 0, had been treated with ATDs for Graves' disease for 9 years including during her previous pregnancy 5 years earlier resulting in a child with Noonan's syndrome—a genetic disorder with autosomal dominant inheritance causing psychomotor developmental delay among other disorders. At gestational week 21, a routine ultrasound scan of the fetus demonstrated a fetal goiter, and maternal ATD treatment was reduced from 20 to 10 mg of methimazole (thiamazole) daily.
When referred to us, the mother had a TSH of 3.9 mU/L (0.4–4.0), total T4 77 nmol/L (60–140), and FT4 5.8 pmol/L (7–20) (Table 1). TSH receptor antibodies were 24 U/L (<1.5). Fetal ultrasound at gestational week 25 + 2 showed a male fetus with polyhydramnios and an enlarged thyroid gland of 1.4 × 3.5 × 3.5 cm, predominantly intrathoragic, with abundant flow (Figs. 2 and 3). Sonographic growth and flow parameters were within normal range as was fetal heart rate (157 beats per minute). Cord blood analysis was conclusive of fetal hypothyroidism (Table 1). Based on our experience with patient 1, we injected 55 μg of levothyroxine intra-amniotically the next day and discontinued maternal ATD treatment.

Fetal goiter viewed from an oblique sagittal plane. Fetal goitrous hypothyroidism can cause intrauterine hyperextension of the fetal neck, thus resulting in obstruction of the esophagus with risk of polyhydramnios and of the trachea with risk of asphyxia and death at delivery. The single white arrow indicates a sagittal scan of a diffusely enlarged fetal thyroid (patient 2, gestational week 28 + 1).

Fetal goiter viewed from the front in a transverse plane. The white dotted lines show the fetal goiter in transverse plane of ∼2.9 × 1.6 × 1.9 cm. A fetal arm is seen to the left. There is an excess volume of amniotic fluid (patient 2, gestational week 28).
One week later (week 26 + 3), the goiter was smaller and no signs of polyhydramnios were present. Another intra-amniotic injection of 150 μg of levothyroxine was given. The woman was followed by weekly thyroid function testing and ultrasound examination. The fetal goiter quickly regressed; at gestational week 30, it was within normal range; and at week 34, it could no longer be seen. Maternal thyroid function was kept at a slightly hyperthyroid level; at gestational week 28, the woman was restarted on methimazole (thiamazole) 5 mg/day; and at gestational week 30, it was increased to 7.5 mg/day. In total, two intra-amniotic injections were given with 55 and 150 μg of levothyroxine, respectively.
The woman went into spontaneous labor at gestational week 40 + 0. Due to breech presentation, an acute, uncomplicated cesarean section was performed and a healthy boy of 3630 g, Apgar 9/10, was delivered. He showed no clinical signs of hypothyroidism, and no goiter was seen. At 2 weeks, he showed no sign of delayed neurological or motor development.
Discussion
The patients reported here were 23 and 25 weeks pregnant when fetal goiter and polyhydramnios were demonstrated at ultrasound examination. They were at the time treated with a daily dose of PTU 400 mg and methimazole (thiamazole) 10 mg, respectively, resulting in maternal TSH levels in upper normal range, whereas FT4 concentrations were below the normal range (Table 1). Cord blood TSH levels were highly elevated with low T4. The fetal goitrous hypothyroidism caused polyhydramnios probably due to relative obstruction of the esophagus and trachea with risk of asphyxia and death at delivery. Although the intra-amniotic levothyroxine injections successfully rendered the fetus euthyroid and without goiters at birth, it is an invasive method that constitutes a risk to the fetus (26). Thus, it is crucial to prevent such incidences of iatrogenic fetal goitrous hypothyroidism from developing, and prenatal diagnosis and treatment are essential. Frequent measurement of thyroid hormones is essential in pregnant women treated with ATDs, and the dose of the drugs should be adjusted to keep the thyroid hormones in the upper normal range according to guidelines (8). Further, in pregnant women with elevated TSH receptor antibodies or treated with ATDs, fetal ultrasound should be performed to look for evidence of fetal thyroid dysfunction, which could include growth restriction, hydrops, or presence of goiter. Umbilical blood sampling should be considered only if the diagnosis of fetal thyroid disease is not reasonably certain considering its risk for bradycardia, infection, premature rupture of membranes, fetal hemorrhage, and death (8,27).
The risk of overtreatment of pregnant women with ATDs in Graves' disease is very high, as the disease itself, being autoimmune in nature, improves during pregnancy, thus requiring less ATDs throughout pregnancy (28 –30). At the same time, clinicians are caught by the fact that thyroid hormone measurements and their interpretation are more difficult during pregnancy. The pregnancy-related hyperestrogenism induces a rise in thyroid-binding globulin (TBG) and, thus, total T4 levels. This makes the interpretation of FT4 estimates difficult, as the estimates are usually derived by some correction for the TBG level either directly in the test tube (so-called nonprotein-bound T4 measurement) or by indirect measure of the protein binding in a triiodothyronine/T4 uptake test, with calculation of FT4 index or direct measurement of TBG (T4/TBG-ratio). Either way, the estimates are influenced by the rise in TBG during pregnancy, and the use of trimester-specific reference ranges based on the specific laboratory method is essential (24,31 –33).
The physiological increase of human chorionic gonadotropin stimulates the TSH receptor due to its TSH-like activity. This increases thyroid hormone production and suppresses TSH by negative feedback. Therefore, using nonpregnant reference intervals results in an underestimation of the amount of women who are in fact hypothyroid (34 –36). Both patients reported here had a serum TSH within the normal non-pregnant reference ranges. However, in a pregnant woman treated with ATDs, this is a strong indicator of maternal hypothyroidism and excessive ATD treatment. Further complicating the interpretation of maternal thyroid status, the intra-individual changes in thyroid hormone levels as the pregnancy progresses have been shown to be significantly smaller than the interindividual changes (37 –39). Finally, the latency of reaction of the pituitary hormone, TSH, worsens the situation of foreseeing maternal hypothyroidism (24,33,37,40).
It is very likely that this fetal condition is underreported, as Graves' disease is very frequent in young fertile women, and centralization of care is not obvious in most countries.
A third similar case has been previously reported by Lassen et al. (41), and patient 1 has been mentioned in a narrative review by Laurberg et al. (42), though the diagnosis and treatments were done in our specialized center after referral from the local hospital. Thus, we have treated three referred cases of iatrogenic fetal goiter within 3 years, which clearly underlines the need of raised awareness among clinicians when treating pregnant women with ATDs. In our own specialized endocrine-gynecology clinic, we treat many pregnant women with ATDs for Graves' disease every year, and due to close monitoring of the women and fetuses, we have not seen a single case of fetal goiter.
Graves' disease during pregnancy is to be considered a very specialized condition requiring close attention to avoid the few cases of malpractice and to optimize the growth and brain development of the child (43 –45).
We report two cases of iatrogenic fetal goiter induced by treatment of maternal Graves' disease with ATDs. The pregnant women were overtreated with ATDs, and hypothyroid, however, went undiagnosed by the local endocrinologist. In each case, obstetric ultrasound diagnosed the fetal goiter and polyhydramnios. The fetal goiters were gradually reduced in volume during the treatment with levothyroxine administered in utero. The babies were without visible goiters at delivery.
In pregnant women treated with ATDs, it is important to perform frequent measurement of peripheral thyroid hormones, especially FT4 estimates, and to keep these in the high, upper, normal nonpregnant reference range by appropriate adjustment of dose of the ATDs. The presence of normal serum TSH levels in pregnant women treated with ATDs indicate excessive treatment. Further, ultrasonography of the fetal thyroid gland by an experienced ultrasonographer is an excellent diagnostic tool. This tool in conjunction with a close teamwork among endocrinologists, obstetricians, and experts in fetal medicine can ensure a normal fetal thyroid function. The presented patients demonstrate the urgent need for centralized care of pregnant women with Graves' disease to very specialized multidisciplinary units, to maintain an optimal fetal brain development and health.
Footnotes
Acknowledgments
Ulla Feldt-Rasmussen has received a grant from Arvid Nilsson's Foundation. Sofie Bliddal is supported by a grant from the Danish Council for Independent Research: Medical Sciences and has received a grant from the H. Plesner Foundation.
Disclosure Statement
The authors declare that no competing financial interests exist.