
Abstract
Background:
Medullary thyroid carcinoma (MTC) is a rare thyroid malignancy with the potential for aggressive behavior. Measurement of serum calcitonin (Ct) in the thyroid nodule population is the most sensitive way to detect occult MTC. An important and controversial question is whether all patients with thyroid nodules should undergo Ct measurements to detect occult MTC.
Summary:
The prevalence of MTC detected by performing surgery on unselected individuals with thyroid nodules with elevated serum Ct is 0.4%. The central role of pentagastrin (PG) stimulation for triaging patients with minimally elevated serum Ct to prevent unnecessary surgery is reviewed. Data concerning a large reservoir of medullary thyroid microcarcinomas are discussed.
Conclusion:
Given the unavailability of PG in the United States and Canada, the available data argue against routine Ct measurements in all individuals with thyroid nodules in these countries because of the potential for unnecessary surgery and the uncertain benefit in diagnosing medullary microcarcinoma.
Introduction
A number of prospective studies (5 –19) and a review (20) support the thesis that measurement of serum Ct is the most sensitive screening test for detecting occult MTC in individuals with thyroid nodules. Yet, controversy swirls around the question of screening for MTC with routine serum Ct measurements in the thyroid nodule population (Ct screening). This review analyzes this controversy by reviewing all the studies that support the use of Ct measurement to screen for MTC and evaluates the nature of the potential benefits and risk of Ct screening, if this were adopted in the United States and Canada.
Review
Ct screening for occult MTC in thyroid nodule populations
A number of primarily prospective studies (Table 1) have found serum Ct measurements to be a highly sensitive screening test for diagnosing occult MTC in patients with thyroid nodules (5 –19). Overall, after measurement of serum Ct, MTC was discovered in 0.4% of 72,000 unselected individuals with thyroid nodules. MTC is virtually never diagnosed in individuals with isolated thyroid nodules in the isthmus, obviating the need for Ct screening in this population (21).
This study also included patients referred to their institution with elevated basal or stimulated Ct.
MTC, medullary thyroid carcinoma.
Ct measurements
A serum Ct >10 pg/mL is considered abnormal in most studies that screen for MTC in the thyroid nodule population. However, the upper limits of normal for serum Ct range from study to study and from assay to assay. One study of several thousand diabetic patients found that the upper limit of normal was <5 pg/mL in women and <8.4 pg/mL in men (22). In many assays, the upper limit of normal is higher in men than in women, and in smokers than in nonsmokers. When d'Herbomez et al. (23) evaluated 375 clinically euthyroid individuals with five different Ct assays, they found that 2.5% to 9.8% had serum Ct >10 pg/mL depending upon the assay. These figures represent an almost fourfold range of elevated basal Ct, despite the fact that all of these individuals had no apparent C-cell disease. The majority of the elevated Ct values were in male smokers.
A number of conditions unrelated to C-cell pathology can cause modest serum Ct elevations. Elevated serum gastrin, due to a variety of conditions, can elevate the serum Ct. These conditions include pernicious anemia, drugs inhibiting gastric acid secretion, or gastrinomas. In one study, individuals taking proton pump inhibitors or H2 blockers had a mean serum Ct of 11.9 pg/mL, whereas those not taking these agents had a mean serum Ct concentration of 6 pg/mL (24).
Additional causes of elevated serum Ct concentration include Ct production from non-MTC malignancies (rare), kidney failure, auto-immune thyroid disease, alcohol consumption, smoking, sepsis, and heterophilic antibodies (23). One recent study reported the presence of heterophilic antibodies causing falsely elevated Ct in 1.3% of individuals with thyroid nodules (25). In short, it is important to be aware that there are many patients with serum Ct >10 pg/mL, without C-cell pathology.
What is the specificity for MTC of an elevated serum Ct in the thyroid nodule population? The study of Costante et al. (7) provides some helpful data (Table 2). Of 5817 patients with thyroid nodules, 216 patients (3.7%) had Ct between >10 and <20 pg/mL. This group of patients was followed clinically. One patient eventually had surgery because of a rising Ct and was found to have CCH. Patients with Ct concentration between >20 and 100 pg/mL underwent pentagastrin (PG) stimulation in this study. A stimulated Ct >100 pg/mL was considered abnormal. For patients with basal or stimulated Ct >100 pg/mL, surgery was recommended. There were 49 patients with Ct between 20 and <50 pg/mL who had PG stimulation testing and 12 were abnormal. Ten patients agreed to surgery. Four patients had MTC and four patients had CCH. There were eight patients (0.14%) with a basal serum Ct between 50 and 100 pg/mL. Four of these had an abnormal PG stimulation test and all four had thyroid surgery. Two of these had CCH and two had MTC. There were nine patients with basal serum Ct of >100 pg/mL, all of whom had thyroid surgery, and all were found to have MTC. Thus, in this study, a basal Ct >100 pg/mL had 100% specificity for MTC. In the whole group, 19 of the 292 patients with abnormal basal serum Ct concentrations (6.5%) had MTC. For individuals with elevated basal serum Ct between 10 and 100 pg/mL, only 5% required surgery.
Source: Costante et al. (7).
CCH, C-cell hyperplasia.
A number of studies (Table 1) analyzed the results of measuring serum Ct in large populations of individuals with known thyroid nodules to help diagnose MTC. Most of these studies incorporated PG-stimulated serum Ct when the basal serum Ct was only modestly elevated. Figure 1 shows a typical algorithm for most studies using screening serum Ct measurements in individuals with known thyroid nodules. Although the general study design was to perform a PG stimulation test for patients with basal serum Ct concentrations between 10 and 100 pg/mL, other studies performed this test when serum Ct concentrations were between 20 and 100 pg/mL. In many studies the design was to perform thyroid surgery if the PG-stimulated Ct concentration was >100 pg/mL; in other studies the design was to perform thyroid surgery if the PG-stimulated serum Ct was >200 pg/mL. Still other studies used a design calling for thyroid surgery if the PG-stimulated serum Ct concentration was greater than three times baseline. In some studies the design called for patients having a PG-stimulated serum Ct between 60 and 100 to have follow-up with PG stimulation in the future (20). Regardless of what Ct cut-off is used in a study, it is clear that PG stimulation occupies a central role in the evaluation of thyroid nodules with modest Ct elevations in most of the published literature. Despite a variety of protocols, the results were consistent across the studies with the largest patient populations. The study of Ozgen et al. (14) is a notable exception in that surgery was performed on four patients with serum Ct >150 pg/mL and no PG-stimulation tests were performed on the others.
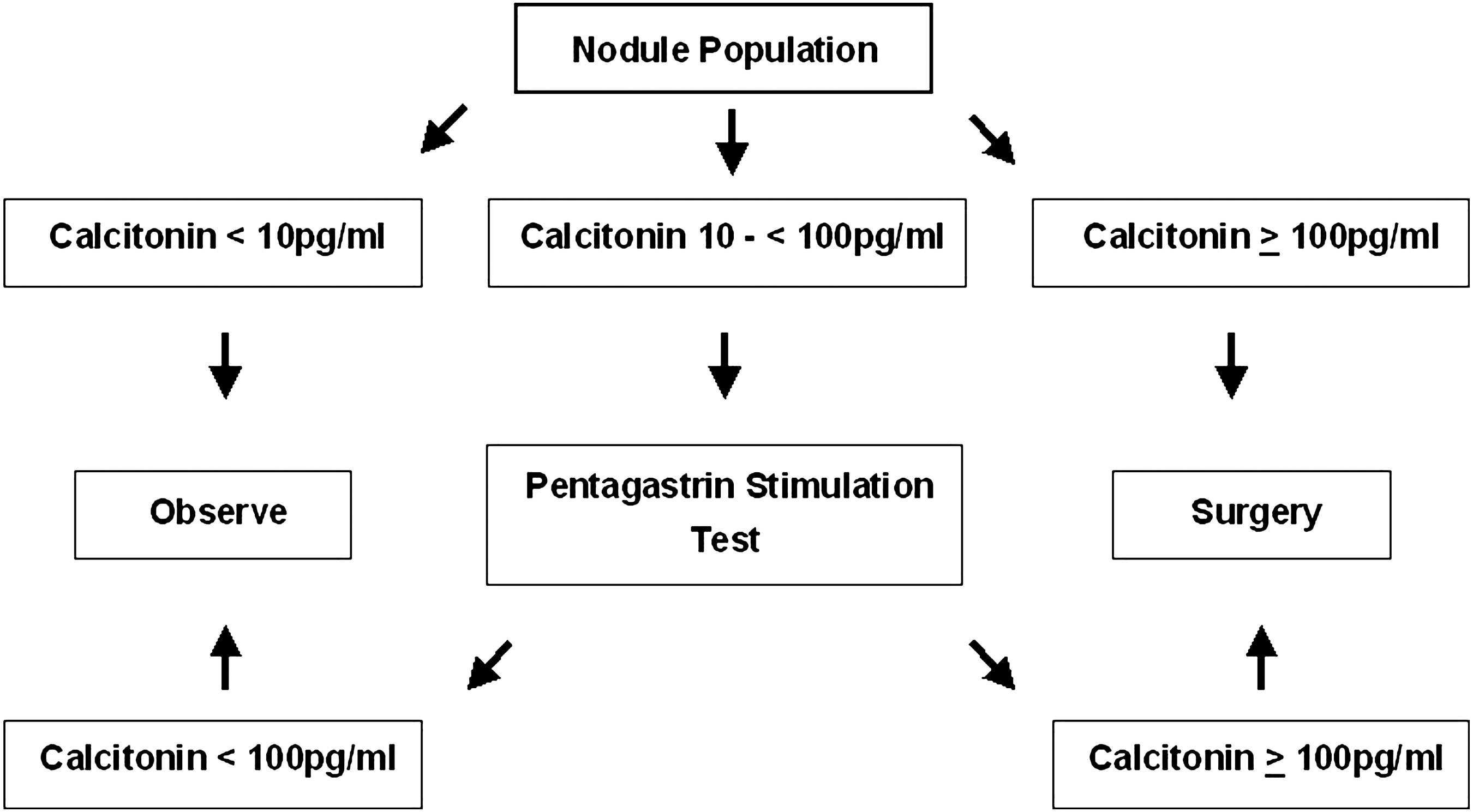
Algorithm for medullary thyroid carcinoma screening in the thyroid nodule population, using serum calcitonin measurements and pentagastrin stimulation testing for elevated serum.
Table 2 shows the data on 5817 patients with thyroid nodules who had serum Ct measurements (7). All patients with Ct >100 had surgery, whereas patients with lower Ct had surgery if the PG-stimulated serum Ct was exaggerated. The higher the basal serum Ct concentration, the greater the prevalence of MTC at surgery. It is likely that surgery on all thyroid nodule patients with modest Ct elevation has a very low yield of MTC, but this remains an unproven assumption, since most of these patients did not have surgery. None of the 216 patients (3.7%) with basal Ct between >10 and <20 pg/mL had MTC, although only 1 such patient had surgery. Of the 49 individuals (3.7%) with basal serum Ct between >20 and <50 pg/mL, 10 (with exaggerated PG-stimulated serum Ct concentrations) had surgery and 4 had MTC. Although it is generally thought that the yield of MTC will be higher if surgery is performed only on individuals with modest serum Ct elevations who have exaggerated PG-stimulated Ct, it is impossible to prove this hypothesis unless all patients in the study group undergo surgery.
Questions such as what baseline Ct or PG-stimulated Ct achieves 100% specificity for diagnosing MTC are less important in the context of screening, since the basic purpose of screening is to achieve a high degree of sensitivity for diagnosing MTC. In general, the sensitivity of Ct measurement is higher than that of fine-needle aspiration (FNA) for the diagnosis of MTC (16,19,26). With FNA alone, the majority of the medullary microcarcinomas reported in many studies (15,16,19,26) would not have been diagnosed. For example, with FNA alone, Henry et al. (15) were able to diagnose 12 of 13 medullary macrocarcinomas but none of 11 microcarcinomas. A variable percentage of the MTCs discovered by screening Ct measurements are low-stage medullary microcarcinomas (Table 1). Scheuba et al. (27) found that 97 of 159 MTCs diagnosed during the years of Ct screening at his institution were medullary microcarcinomas. His data are not included in Table 1 because the number of individuals screened is not recorded.
Some studies suggest that the prognosis for MTC diagnosed by Ct screening is better than MTC diagnosed in historical controls without the benefit of serum Ct screening (10,28). Using a basal Ct of >50 pg/mL as the criteria for performing thyroid surgery, Elisei et al. (10) found an improved outcome in MTC diagnosed by serum Ct screening as compared with MTC patients diagnosed before the serum Ct screening era. These authors found a 10-year survival rate of 86.8% in MTC patients diagnosed by serum Ct screening as compared with a 43.7% 10-year survival rate in those diagnosed before serum Ct screening. Karga et al. (28) compared MTC diagnosed before serum Ct screening in the years between 1969 and 1989 (group 1) with MTC diagnosed in the era of serum Ct screening between 1990 and 2009 (group 2). The MTC tumors were smaller and the 15-year disease-specific survival rate was higher in group 2 (85%) compared with group 1 (35%).
Hence there is clear evidence favoring screening Ct measurements to diagnose early MTC. Yet despite this evidence, recommendations for and against Ct measurements in the thyroid nodule population are considered controversial.
Natural history of MTCs as a determinate of the benefits of screening
When recommending screening for an uncommon disease, the cost and the risks of screening must be weighed against the benefits. Let us address the major potential benefit first, namely, the well-established increased ability to diagnose early MTC with serum Ct measurements. Measurement of serum Ct is a more sensitive test for diagnosing occult MTC than FNA. The data clearly support a high prevalence of MTC (approximately 0.39%) in patients with thyroid nodular disease (Table 1). It is axiomatic that all large MTCs begin as small MTCs. Is it valid to assume that all small MTCs grow and eventually become larger, potentially morbid or fatal MTCs? If there is a large reservoir of medullary microcarcinomas that rarely grow into aggressive medullary carcinomas the potential benefit of discovering these microcarcinomas would be small.
Based on the number of individuals with thyroid nodules in the United States by decade of age (29) and the U.S. population based on the 2008 census, one may estimate that 76 million individuals (25% of the U.S. population) have thyroid nodules 1 cm or greater in size. Based on data from European epidemiologic studies, this number may be an underestimation pending additional epidemiologic studies from the United States. Hegedüs reports a 50% prevalence of thyroid nodules in an iodine-deficient population (30). Gharib and Papini suggest that 20% to 76% of individuals will have nodules detected by ultrasound (31). If nodules smaller than 1 cm are considered, even more individuals will have thyroid nodules. In a recent evaluation of 635 consecutive German individuals (33% female, 67% male, mean age 56.7 years), 68% had thyroid nodules (32). The data in Table 1 suggest that the prevalence of MTC in small thyroid nodules is likely to be as high or perhaps even higher than in larger nodules.
Based on the studies reviewed in Table 1, if the prevalence of MTC in the thyroid nodule population in the United States is the same as in the European studies, then the prevalence of MTC in the United States must be at least 296,000 cases (0.39% of 76 million individuals with nodules). Based on the SEER database we know that approximately 2% of the 37,000 newly diagnosed thyroid cancers each year are MTC (1) for a total of approximately 750 new cases of MTC each year in the United States. Based on an arbitrary estimate of a 30-year period to allow MTC to grow large enough for clinical diagnosis, the prevalence of MTC must be approximately 23,000 cases, that is, annual incidence of 750 cases per year ×30 years.
Taken together, these figures suggest that there is at least a 10-fold disparity between the screening data (296,000 cases) and the clinical data (23,000 cases) for MTC. Indeed, this disparity might be even greater if the prevalence of thyroid nodules is higher than 25%.
Is it possible that the screening data are incorrect? The studies included in Table 1 include over 70,000 individuals, a sample size that is likely to yield highly reliable data. The most logical explanation is that there is an undiagnosed reservoir of patients with medullary microcarcinoma that are either never discovered or else remain clinically insignificant. Although quantitatively smaller, this situation is similar to the undiagnosed reservoir of papillary thyroid microcarcinomas in the population (33). Are there other data to support this high prevalence of medullary microcarcinomas?
Table 3 reviews a number of autopsy studies that commented on thyroid pathology (34 –41). One study (35) was from Belarus, one from the United States (36), and the others were all from Europe. Similar findings in these studies suggest but do not prove that medullary microcarcinomas may be common in all populations. These reports do not include those in which there was not clear distinction between papillary and medullary microcarcinomas. The prevalence of MTC in these autopsy studies in nonselected populations was 0.75%, a higher figure than the one reported for individuals with thyroid nodules in Table 1, but if one excludes the apparent outlier study of Autelitano et al. (38), which reported a 3.4% prevalence of MTC, then the prevalence of MTC in the remaining unselected autopsies is 0.3%, a number roughly comparable to the Ct screening studies in the thyroid nodule population. If the autopsy data are correct then the prevalence of medullary microcarcinomas in the general U.S. population could be as high as 900,000 (0.3%) to 2,250,000 (0.75%).
Other data also support the presence of medullary microcarcinomas in individuals without apparent thyroid nodules, or with normal baseline Ct concentrations. Karanikas et al. (11) evaluated 219 individuals with non-neoplastic thyroid disease. Fifteen patients had an elevated Ct and one (0.4%) had a medullary microcarcinoma. Niccoli et al. (18) evaluated 1133 patients with nodules destined for surgery with normal serum Ct concentrations (<10 pg/mL). Two of these patients (0.2% of the group) had MTC. Kaserer et al. (16) found that 3 of 19 MTCs had a serum Ct concentration of <10 pg/mL. Scheuba et al. (27) reported that 6 of 97 medullary microcarcinomas had a basal serum Ct of <10 pg/mL. Vierhapper et al. (8) also measured serum Ct in 3843 patients without thyroid nodules. All patients with baseline serum Ct >10 pg/mL underwent PG-stimulated serum Ct measurements. Of the 198 who had PG-stimulated serum Ct, 24 of these had PG stimulated serum Ct concentrations of >100 pg/mL. Surgery was performed in only six patients: two had MTC and four had CCH. Therefore, only 0.05% of these patients had MTC but 75% of patients with PG stimulated Ct >100 pg/mL did not undergo surgery. In contrast, 75% of patients with nodular thyroid disease, with basal serum Ct concentrations of >10 pg/mL and with PG stimulated serum Ct concentrations of >100 pg/mL underwent thyroid surgery (8). One can conclude that there are populations with MTC without apparent thyroid nodules as well as populations with MTC with apparent thyroid nodules and a low baseline serum Ct (<10 pg/mL) who have MTC.
Risks of thyroid surgery for patients with indolent MTCs or screening-based suspicion of MTC
Thyroid surgery on all patients with modest Ct elevation has a very low yield of MTC (Table 2). Using a vigorous response to PG-stimulation as an indication for surgery markedly increases that yield. In countries, such as the United States, where PG is not available, it is difficult to know the correct course of action when the serum Ct falls between 10 and 100 pg/mL. For Ct concentrations between 50 and 100 pg/mL the risk of MTC is approximately 25%. This high risk may justify surgery for all patients with Ct between 50 and 100 pg/mL, but surgery would be unnecessary in 75% of these cases. Based on the available data (Table 2) 4.5% of individuals with thyroid nodules would likely have a serum Ct between 10 and 50 pg/mL if Ct measurements were performed on all individuals with thyroid nodules. Using gender-specific Ct thresholds may improve the specificity of modest Ct elevations for diagnosing MTC (42). The potential risks of Ct screening for individuals with Ct between 10 and 50 pg/mL are unnecessary surgery (only 2% of these patients have MTC) or unnecessary anxiety for the patient and the physician. The potential morbidity and expense of unnecessary thyroid surgery is of great concern. The morbidity related to persistent anxiety and uncertainty related to an elevated serum Ct cannot be estimated. It is difficult to know whether concern for patient outcome or fear of litigation will drive clinicians to recommend surgery for all patients with elevated basal Ct.
Calcium is also a secretagogue for Ct in both normal individuals and in those with MTC and CCH. Doyle et al. (43) evaluated 50 healthy nonsmoking individuals without thyroid nodules. After PG stimulation, the 95th percentile peak Ct was 37.8 pg/mL in men and 26.2 pg/mL in women. After calcium infusion, the 95th percentile peak in men was 131.1 pg/mL and 90.2 pg/mL in women. The peak Ct in one man was 230 pg/mL. The authors concluded that calcium is a better tolerated and a more potent stimulus for Ct release than PG. Unfortunately, these data provide no guidance for the use of calcium-stimulated Ct in patients with thyroid nodules. Specifically, they provide no guidance about what stimulated-Ct concentration should trigger a recommendation for surgery because there are no data available concerning the sensitivity and specificity of various Ct cut-offs after calcium stimulation for diagnosing MTC or CCH in the thyroid nodule population. Until such data are available, the role of calcium stimulation to improve the specificity of basal Ct measurements in the thyroid nodule population is purely speculative.
Are there data to support the safety of observation in individuals with thyroid nodules and serum Ct between 10 and 50 pg/mL? Although no studies directly address this question, some studies indirectly address the consequences of observation. The study of Hasselgren et al. (44) is not included in Table 1 because it was a retrospective study, and not all nodule patients in the study had Ct measurements. These authors measured Ct in 702 nodule patients but did not measure Ct in 300 additional patients. Six of the Ct-screened nodule patients had MTC (0.9% of those with Ct measurements, 0.6% of all nodule patients). The Ct assay was insensitive with the detection limit being 100 pg/mL. After a median follow-up of 7 years, none of the 300 patients without Ct measurements and none of the screened patients with (presumed) Ct concentrations between 10 pg/mL and 100 pg/mL subsequently appeared in the Danish Thyroid Cancer registry as having MTC. The Danish Thyroid Cancer registry records all cancer diagnoses in Denmark. Sixteen patients with Ct >100 pg/mL, did not have thyroid surgery, and none of them were subsequently diagnosed with MTC. In this study, the positive predictive value of a Ct >100 was only 15.4%. Four of the six MTC patients had a malignant FNA.
Costante et al. (7) observed 216 patients who did not have initial surgery with serum basal Ct concentrations between >10 and <20 pg/mL. Among patients, 45 refused follow-up. One patient, whose basal Ct increased to 33 and was 317 pg/mL after PG-stimulation, was diagnosed with CCH after a thyroidectomy. In contrast, the study of Rink et al. (6) showed that 3 of 28 MTCs diagnosed by screening Ct had basal serum Ct concentrations between 15 and 20 pg/mL. Iacobone et al. (12) found that 9 of 26 medullary microcarcinomas had basal serum Ct concentrations of <30 pg/mL, 4 of whom had PG-stimulated serum Ct <100 pg/mL. Cherenko et al. (45) reported on 125 patients over a 15-year period with nodular thyroid disease and basal Ct <30 pg/mL and stimulated Ct <200 pg/mL. Seventy-three patients underwent thyroid surgery. Medullary thyroid microcarcinoma was found in 6 patients (8%), CCH was found in 54 patients (74%), and 13 patients (18%) had no C-cell pathology. Fifty-two additional patients with Ct values in this range did not have surgery (mean basal Ct 18.1 pg/mL; S.D. 4.8 pg/mL and stimulated Ct 75.5 pg/mL; SD 49.1 pg/mL). In one-third of these patients, Ct concentrations subsequently normalized on their own. Cherenko et al. (45) concluded that surgery may not be necessary for individuals with Ct concentrations in this range. Patients were followed-up over a mean of 36 months (SD 38 months) and no mention was made of subsequent MTC.
An interesting question is whether the discovery of CCH should be considered an added beneficial outcome of routine Ct measurements in the thyroid nodule population. Although CCH is generally considered a precursor for MTC in individuals with MEN 2 and MEN 2 RET mutations (46) [although not all MEN 2 MTCs are accompanied by CCH (47)], there is no compelling evidence that CCH is a precursor to MTC in the general (non-MEN 2) population. In fact, CCH is very common in the absence of MTC. In one study of forensic autopsies, 33% of individuals with apparently normal thyroid glands had CCH (48). Santeusanio et al. (49) carefully examined 150 autopsy thyroid glands for CCH. Of the 48 patients with normal thyroid histopathology, 66% had CCH; higher percentages were found in individuals with various thyroid pathologies,
There are little data about serum Ct concentrations in individuals with CCH at pathological examination in the non-MEN population. Scheuba et al. (50) evaluated C-cell changes in 57 individuals with normal PG-stimulated Ct testing before thyroid surgery. On pathological examination of the 18 patients with Graves' disease, 66% had CCH. Of the 39 patients with nodular disease, 41% had CCH. Two patients were found to have neoplastic CCH but not frank MTC. The serum Ct concentrations were 1 and 14.8 pg/mL, respectively, in these two patients, but both of them had normal PG stimulated Ct. Based on these limited data, Ct hypersecretion is not characteristic of most patients with sporadic CCH.
There are rare reports of sporadic MTC with apparent transition from CCH (17,19). It is not known how often (non-MEN 2) CCH with modest Ct elevation is a precursor for MTC, but we do know that CCH cannot be an obligatory precursor to MTC given the high prevalence of CCH noted above. Individuals diagnosed with MTC based on Ct screening studies do occasionally turn out to be index cases of MEN 2 kindreds (8), but this is a rare event.
Reviews and guidelines concerning Ct screening
A number of authors and professional societies have opined on whether Ct measurements should be performed in all individuals with thyroid nodules. Some of the regional differences in their conclusions may be explained by the availability of PG (e.g., in Europe) and its nonavailability in the United States.
Based on a literature review through 2004, Hodak and Burman (51) concluded, “It does not seem to us that the use of basal Ct levels in the routine screening of patients with nodular or non-nodular thyroid disease is warranted at present, without the ability to use PG stimulation as a confirmatory test.” Since that time, a number of different opinions have been expressed.
The German Evidence Based Consensus recommendation was, “Analysis of basal Ct is advisable in all patients with documented thyroid nodules with and without thyroid enlargement” (52). The European Thyroid Cancer task force concluded, “Thus, serum Ct measurement is recommended in the initial diagnostic evaluation of thyroid nodules” (53). However, several leading European authorities, one of whom contributed to prior guidelines, subsequently argued that “convincing arguments for or against the routine use of Ct screening in patients with thyroid nodules are currently lacking” (54). The American Thyroid Association Guidelines were agnostic concluding that “the panel cannot recommend either for or against the routine measurement of serum Ct” (55). The American Association of Clinical Endocrinologists (AACE), Associazione Medici Endocrinologi (AME), and European Thyroid Association (ETA) guidelines noted: “Measurement of nonstimulated serum Ct level may be considered before thyroid surgery for nodular goiter” (56). These authors speculated that calcium-stimulated Ct testing—currently available in the United States —can serve as a substitute for PG- stimulation. As noted, this is a plausible hypothetical suggestion which requires clinical data to support this position.
A recent analysis from Canada concluded that Ct screening for nodular disease would be cost effective in the United States (57). Cheung et al. (57) concluded that the addition of Ct screening would cost $11,793 (range $10,941–$12,646) per life years saved. This figure was based on a Ct cost of $37 (range $ 25–75), whereas life years saved were calculated based on disease stage at diagnosis. At our institution, the current charge for Ct measurement is $172, although different insurers will pay different amounts for this same test. The calculations of Cheung et al. (57) were based on surgical recommendations for individuals with Ct measurements >50. This study did not address the dilemma of elevated Ct between 10 and 50 pg/mL and the potential unnecessary surgeries in this group of patients.
Like Cheung et al. (57), Borget et al. (58) concluded that Ct screening is cost effective in the nodule population, but they also noted that more work was needed before a final assessment of the benefit of Ct screening could be made: “[A]t the same time, further studies are obviously needed to confirm the benefits of routine Ct screening on life expectancy and, conversely on unnecessary treatment. These studies should be prospective, randomized, and based on a large number of patients who are followed for a protracted period of time.”
Analysis and Conclusions
It is difficult to accurately assess the cost–benefit analysis of serum Ct measurements in the United States, where PG stimulation is no longer available. The data suggest that there is a large, previously unrecognized reservoir of medullary microcarcinoma that might be uncovered by Ct screening in the nodule (or general) population. It is impossible to assess the benefit of surgery for most medullary microcarcinomas, since we do not know what percentage of these microcarcinomas grow into to medullary macrocarcinomas. We also cannot accurately assess the risk of observation for medullary microcarcinomas diagnosed on the basis of Ct screening. If, as suggested by the data, the natural history of medullary microcarcinoma is considerably more favorable than heretofore assumed, and most non-FNA diagnosable MTCs are microcarcinomas, then the benefits of screening may be overestimated and the risks of observation may be acceptable.
If a Ct screening strategy were adopted in the United States, the correct approach to individuals with Ct between 10 and 50 would introduce a new dilemma: how do we assess the risks of unnecessary surgery versus the potential physician and patient anxiety related to observation in patients with Ct concentrations in this range? Physician concern about litigation for not recommending surgery must also be considered. If one were to accept a valuable and central role for Ct measurements in individuals with known thyroid nodules, an additional dilemma arises. Are we now obligated to use ultraonography to screen the remaining U.S. population for the 80%–90% of individuals with thyroid nodules who remain undiagnosed during their life-time (29)? Last, based on the autopsy data, would Ct screening be required in the general population?
What is the alternative to Ct measurements in all individuals with thyroid nodules? The current alternative utilizes a combination of ultrasound guided FNA when indicated and careful ultrasound surveillance. It is likely that current ultrasound and ultrasound-guided biopsy techniques will lead to surgery for most medullary macrocarcinomas (≥10 mm). Henry et al. diagnosed 12 of 13 medullary macrocarcinomas by FNA (15). Bugalho et al. (26) reviewed the preoperative FNA diagnoses on 67 confirmed MTC. Of 67 FNAs, 9% were considered benign, 63% were diagnosed as MTC, 21% were suspicious for malignancy (not MTC), and 7% were indeterminate (and referred for surgery). Hence, 91% of the MTCs would have been referred for surgery based on the FNAs.
When an FNA is cytologically atypical or suggestive of MTC, either immunohistochemistry for Ct can be performed on FNA cytology specimens or Ct can be measured on needle washings from repeat FNA specimens (59). These techniques should enhance the preoperative diagnosis of MTC. For smaller (micro) MTCs, it is apparent that many may be missed on the initial ultrasound. Given the resolution of current ultrasound examinations, nodules as small as 1–2 mm are often evident and these can easily be monitored for growth.
The critical question remains unanswered: what is the risk of developing a clinically important, potentially lethal MTC which will be diagnosed too late when a patient undergoes careful annual serial ultrasound examinations? Both clinical experience and the observational data presented here suggest that this risk is unknown, but likely to be minimal. Even if most medullary microcarcinomas do not become aggressive cancers, is there harm in testing for them and operating on those in whom the basal Ct is in the range found in medullary microcarcinoma? In my opinion routine Ct measurement in patients without PG availability would expose an inordinately large percentage of these patients with modestly elevated Ct to the costs and risks of an unnecessary total thyroidectomy as they would not have MTC.
In summary, it can be concluded from the available data that routine Ct measurements in the U.S. thyroid nodule population to diagnose cryptic MTC is not indicated at this time. The reasons include the large reservoir of medullary microcarcinomas of uncertain malignant potential; the unavailability of PG stimulation in the United States, which may lead to unnecessary surgery for patients with minimally elevated serum Ct; and increased patient and physician anxiety related to observing patients with minimally elevated serum Ct.
If calcium-stimulated Ct screening proves reliable in predicting MTC or if PG becomes available again in the United States, the question of Ct screening should be re-assessed with the benefit of randomized, controlled trials. In the meantime, it might be interesting to explore whether an elevated procalcitonin:Ct ratio predicts aggressive behavior of small MTCs. In a preliminary study of 69 overt MTC patients, Walter et al. found that higher procalcitonin:Ct ratios predicted disease progression (60).
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.