
Abstract
Background:
Thyroid hormones have profound effect on the heart and peripheral vasculature. Hypothyroidism is associated with an increase in a number of coronary heart disease (CHD) risk factors including dyslipidemia, hypertension, and elevated levels of homocysteine. Our objective was to assess the effects of hypothyroidism (thyroid-stimulating hormone [TSH]: >10 μU/mL), moderate subclinical hypothyroidism (SCH; TSH: 6.1–10 μU/mL), and mild SCH (TSH: 3.1–6.0 μU/mL) on cardiovascular risk factors, CHD prevalence, and all-cause mortality in patients at high risk for CHD seen in a preventive cardiology clinic.
Methods:
All patients seen in the Cleveland Clinic Preventive Cardiology clinic have demographic and laboratory tests including TSH and multiple CHD risk factors obtained at the baseline visit. All data are entered into a database (called PreCIS). The social security death index is queried monthly to determine all-cause mortality.
Results:
Several CHD risk factors including age, male gender, systolic blood pressure, triglycerides, and fibrinogen were more common in hypothyroid patients. Prevalence of CHD was more common in hypothyroid and moderate SCH patients. All-cause mortality was higher in hypothyroid and moderate SCH patients, but not in mild SCH patients. Higher mortality in these groups was observed in both genders, patients under 65 years of age, and patients not on thyroid replacement therapy, but was not observed in patients over 65 years of age.
Conclusions:
Hypothyroidism and moderate, but not mild, SCH are associated with increased CHD prevalence and all-cause mortality. These observations suggest patients with moderate, but not mild, SCH and patients at high risk for CHD should be treated with thyroid replacement therapy.
Introduction
Thyroid hormones cause a decrease in the peripheral vascular resistance through genomic and nongenomic action on vascular smooth muscle cells. These include increase in endothelial nitric oxide synthase activity and increased expression of adrenomedulin. Decrease in peripheral vascular resistance activates the renin–angiotensin system and leads to increase in intravascular volume.
Hypothyroidism is associated with an increase in a number of coronary heart disease (CHD) risk factors including dyslipidemia, hypertension, and elevated levels of homocysteine. Hypothyroidism is also associated with increased CHD events and mortality. Subclinical hypothyroidism (SCH) defined as an elevated thyroid-stimulating hormone (TSH) with normal thyroxine and T3 has been associated with CHD risk factors, but the association with CHD events and mortality is not clear (2,3). Further, there is evolving controversy about whether SCH is characterized only by TSH above the upper limits of normal for most TSH assays (typically in the range of 5–6 μU/mL) or whether a lower threshold (e.g., >3 μU/mL) should be used (4
–6). These observations have implications for when replacement with thyroid hormone, most commonly
The Preventive Cardiology Clinic at the Cleveland Clinic has obtained TSH values as part of the baseline screening examination for >10 years. Several traditional and nontraditional markers for CHD are evaluated and all-cause mortality is available for patients who have been seen in this clinic. Therefore, we analyzed whether hypothyroidism and SCH using two different TSH ranges (>3–6 and >6–10 μU/mL) would be associated with increased all-cause mortality. We also determine whether these ranges predicted CHD risk and/or were associated with CHD risk factors reported in other studies. Finally, if our hypothyroid group(s) showed any increase in mortality, we could determine whether such an increase was a result of increased CHD risk factors or might be the result of other metabolic abnormalities.
Methods
Study design
We performed a retrospective cohort analysis of 6408 consecutive patients from the PreCIS database (Preventive Cardiology Information System, Cleveland Clinic) who were seen between January 1995 and June 2008. Patients seen in this clinic have been previously described (7 –10) and may be self-referred or referred by a physician for assessment and management of CHD risk factors for one (or more) of the following criteria: known CHD, a strong family history of CHD, and difficulty with management of one or more CHD risk factors. From among this group, we excluded 168 patients who had a TSH <0.4 μU/mL as we did not include any patients with overt or subclinical hyperthyroidism. By prespecified analyses, we defined the reference group as those with TSH values between 0.4 and 3.0 μU/mL. The other TSH ranges were prespecified prior to the analyses and were defined as mild SCH (TSH: 3.1–6.0 μU/mL), moderate SCH (TSH: 6.1–10 μU/mL), and hypothyroidism (TSH: >10 μU/mL). Patients on replacement therapy for hypothyroidism were included in the initial analyses. Mortality data were subsequently analyzed for patients not on thyroid replacement therapy. The PreCIS database was updated monthly for death status using the Social Security Death Index. The mortality in our study was calculated based on the number of deaths that occurred in the study cohort between the intervals defined above.
Baseline measurements
At the time of the visit, demographic information, medical history, physical examination, and laboratory data were entered into an electronic medical record and corresponding database. All assays were performed using standard laboratory methods. Fasting low-density lipoprotein–cholesterol values were calculated using the Friedwald equation unless triglycerides were >250 mg/dL when direct determination was employed. TSH was measured by a two-site chemiluminometric assay performed on an automated platform (Modular analytics E-170; Roche Diagnostics). The assay has an analytical sensitivity of 0.005 μU/mL at three levels.
Statistical analyses
Data are presented as mean ± standard deviation or median and interquartile range for continuous variables and percentages for categorical variables. Demographic and risk factors for cardiovascular disease were compared across TSH groups using analysis of variance for normally distributed or Kruskal–Wallis test for nonnormally distributed, continuous variables and chi square test for discrete variables. Some variables were not available for the full duration of the baseline visits, because they have not been consistently obtained. Uric acid values were obtained early and then discontinued as a routine measure. Urinary albumin/creatinine ratio and ultrasensitive C-reactive protein were not included in the baseline visits for several years, but were added later. These values were included in the summary analyses, and reduced numbers of patients were reported in the results.
Kaplan–Meier survival curves by TSH groups were used to summarize time to death up to 8 years of follow-up. Time to death was defined as the difference between the patient's prevention clinic entry visit until the date of death. Patients who did not die were censored at their last prevention clinic visit.
Multivariable Cox proportional hazards models were employed to determine whether TSH categories remain associated with death after adjustment for clinical risk factors. Variables considered for adjustment resulted from a bootstrapping analysis in which 300 models were generated. Variables that entered the models at least 50% of the time were considered for the final model. TSH categories were included in the bootstrapping analysis. Variables that remained statistically significant (p-value < 0.05) in the multivariable model were used. These variables, including TSH categories, are age (per 10 years), current smokers, primary versus secondary prevention categorization, history of cerebrovascular disease, history of hypertension, waist circumference (cm), body mass index, diastolic blood pressure, glucose, and the log transformation of homocysteine and triglycerides. As there were several variables that had missing values (<10%), an imputation of the mean values was used to eliminate the loss of patients in the model. Hazard ratios (HRs) and 95% confidence intervals (CIs) were used to demonstrate the risk of all-cause mortality through 8 years. The TSH category of 0.4–3.0 μU/mL (euthyroid) was used as the reference group.
All analyses were performed using SAS 9.1 (SAS, Inc.). No adjustment was made for multiple comparisons. p-Values <0.05 were considered statistically significant.
The PreCIS database analyses were approved by the Cleveland Clinic Institutional Review Board.
Results
Demographic characteristics
Subject groups were divided by prespecified TSH ranges (μU/mL) <0.4, 0.4–3.0, 3.1–6.0 (defined as mild SCH), 6.1–10 (defined as moderate SCH), and >10 (hypothyroidism) (Table 1). We excluded the <0.4 μU/mL group (n = 168), to have a true euthyroid comparator. Most patients (n = 4675, 76.4%) were in the euthyroid range based on TSH, whereas 1218 (19.5%) had mild SCH, 178 (2.9%) had SCH, and 79 (1.3%) had hypothyroidism.
Values are reported at mean ± standard deviation or median (interquartile range).
n/n/n/n for each group when the reported variable had not been obtained for the duration of the baseline visits.
TSH, thyroid-stimulating hormone; SCH, subclinical hypothyroidism; BMI, body mass index; SBP, systolic blood pressure; DPB, diastolic blood pressure; CHD, coronary heart disease; TG, triglyceride; HDL-C, high-density lipoprotein–cholesterol; LDL-C, low-density lipoprotein–cholesterol; usCRP, ultrasensitive C-reactive protein; Lp(a), Lipoprotein (a); NS, not significant; ATP, adult treatment panel.
There were more men in the euthyroid group (p < 0.001). Mean systolic blood pressure was highest in the hypothyroid group. Both total cholesterol (p = 0.024) and triglycerides (p = 0.006) showed progressively higher values from euthyroid to hypothyroid groups. Although high-density lipoprotein–cholesterol values were lowest in the euthyroid group, there was no consistent trend across groups; however, differences were statistically significant (p = 0.006). Among other risk factors, only fibrinogen showed higher values in the hypothyroid groups (p = 0.002). Median serum creatinine values were statistically higher in the hypothyroid group compared with the other groups (p = 0.02). In general, patients in the SCH and hypothyroid groups had greater risk for vascular disease as shown by a higher prevalence of baseline CHD (p < 0.001), more patients classified as secondary prevention (p = 0.003), and higher Framingham risk scores (p < 0.001). The percentage of patients on any lipid-lowering agent was not different across groups.
All-cause mortality
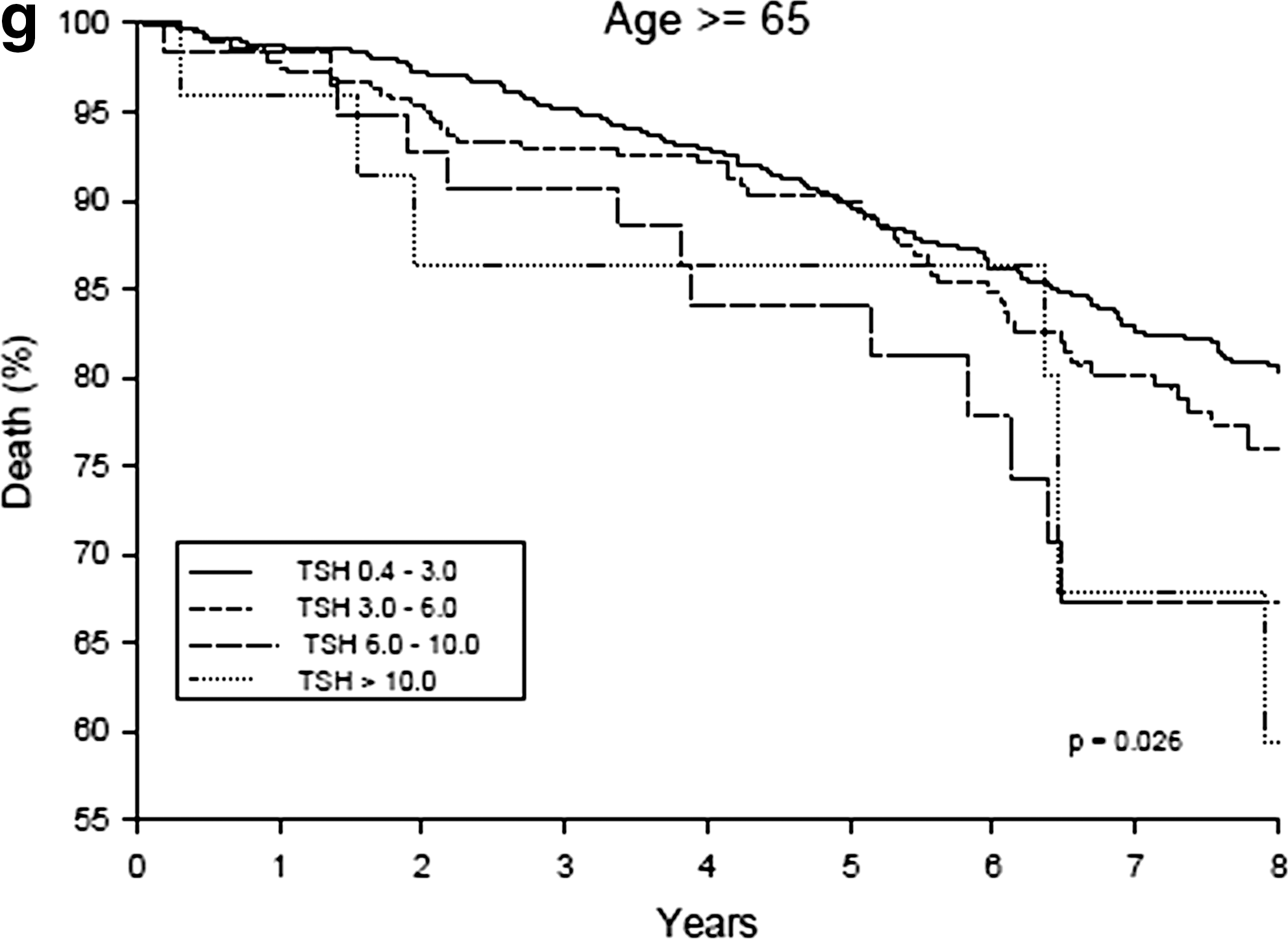
All-cause mortality was increased across the four patient groups when all subjects were included in the analyses (Fig. 1a, p < 0.001). Specifically all-cause mortality was increased in the hypothyroid (25.7%) and the SCH-moderate (18.0%) patient groups. All-cause mortality was not increased in the SCH-mild group compared with the euthyroid group until 8 years after prevention entry visit. The increased mortality with hypothyroidism was seen in both genders (Fig. 1b, c: women, p = 0.003; men, p < 0.001). For both patients aged <65 years and patients aged >65, mortality was increased in the hypothyroid and SCH-moderate groups. For patients not on thyroid replacement therapy (Fig. 1d), all-cause mortality was increased in hypothyroid and SCH-moderate groups compared with the euthyroid group (p < 0.001). There were no differences in mortality in patients on thyroid replacement therapy; however, the number of subjects (n = 515) was much smaller than in the other groups.

Multivariable analysis
The unadjusted HRs for SCH-mild, SCH-moderate, and hypothyroid groups (compared with the euthyroid group) were statistically significant (HR = 1.31, 95% CI: [1.03, 1.68]; HR = 2.15, 95% CI: [1.36, 3.38]; HR = 2.96, 95% CI: [1.70, 5.17], respectively). Adjusting for the variables resulting from the bootstrap analysis (are age [per 10 years], current smokers, primary versus secondary prevention categorization, history of cerebrovascular disease, history of hypertension, waist circumference [cm], body mass index, diastolic blood pressure, glucose and the log transformation of homocysteine and triglycerides), the SCH-moderate and hypothyroid groups remained statistically significant compared with the euthyroid group (HR = 1.61, 95% CI: [1.02, 2.55], p = 0.04; HR = 2.34, 95% CI: [1.33, 4.10], p = 0.003, respectively). However, there was no difference in the SCH-mild group compared with the euthyroid group (HR = 1.19, 95% CI: [0.93, 1.53], p = 0.17).
Discussion
The data from this study demonstrate clearly that hypothyroidism and moderate SCH are both associated with increased risk for mortality in high-risk population. This observation of increased mortality in patients with TSH values >6 μU/mL is true for both genders and for patients under and over the age of 65 years. The PreCIS database cohort is characterized by patients at high risk for coronary disease (7 –10). Further, the patients seen in the Preventive Cardiology Clinic—the source for this database—are well characterized in terms of their CHD risk factors. Even at entry to the clinic, patients as a group are already pretty aggressively treated. Thus, this study cohort is typical of patients seen in many clinics and the results from this study cohort are applicable to many patients seen in clinics and offices who treat high-risk patients. Finally, this is one of the largest observational datasets in a well-characterized patient population.
Although a number of studies in hypothyroid patients have shown its association with cardiovascular risk factors such as lipid profile, homocysteine level, and arterial stiffness, the association of SCH with increased risk for atherosclerotic disease and increased mortality is less clear (2,3,11 –46). Further, uncertainty exists about whether these risks exist only in moderate SCH, that is, patients with values above the upper limits of normal (typically in the 5–6 μU/mL range) and below the generally accepted values for hypothyroidism (typically > 10 μU/mL) or whether risks exist with TSH values > 3 μU/mL. Our data confirm increased risk for mortality in the hypothyroid range (>10 μU/mL) and support the concept that increased risk exists in the moderate subclinical hypothyroid range (6.1–10 μU/mL). Our data do not confirm the data that suggest increased risk in the mild subclinical hypothyroid range (defined in the present study as 3.1–6 μU/mL).
Several meta-analyses and reviews have been recently published that have analyzed whether SCH is associated with an increased risk for CHD events, CHD mortality, and all-cause mortality (13 –15,18,40,44,45,47). Four recent meta-analyses (14,18,45,47), a systemic review (44), and summary of cohort studies (13) include a number of the same studies yet differ somewhat in their conclusions. Our study confirms several conclusions from these reports. Our data confirm the observations of increased mortality risk with hypothyroidism in subjects <65 years noted by Razvi et al. (47) and Ochs et al. (14). Our study population is a high-risk population and thus generally confirms the observation noted by Haentjens of increased mortality risk in cohorts with comorbidities (risk ratio [RR]: 1.76, 95% CI: [1.36–2.3]) compared with the community cohorts in his report (RR: 1.03, 95% CI: [0.78–1/35]) (13). Volzke et al. perhaps captures the essence of the difficulty by noting in his review that results among studies are “highly” discrepant (44). However, he further notes “High-quality observational studies on the relation between thyroid dysfunction and mortality that particularly attempt to reduce selection as well as misclassification bias and control for important confounders are needed.” This observation supports the importance of large studies like ours in which all patients seen in the clinic are entered into our analyses and risk factors are well characterized, by which the generalizability to similar populations may be easier to address.
The recent carefully performed meta-analysis reported by Ochs et al. include six studies included in the analyses of SCH and all-cause mortality (14). These studies included 9220 subjects, and four of these studies had >1000 subjects. Three of these studies included community samples and only one study was from a cardiology cohort. The reported relative risk for all-cause mortality in the meta-analysis was 1.12 (95% CI: [0.99–1.26]).
The results of five large studies (>1000 subjects)—several of which were included in Ochs et al. and the other meta-analysis—will serve as useful comparisons for the result in the present report (2,3,23,43,46). Cappola et al. studied 3233 community-dwelling subjects aged >65 years from the Cardiovascular Health Study (2). In this study group, 82% were euthyroid, 15% had SCH, and 1.6% were overtly hypothyroid. Cappola et al. could not demonstrate any association of SCH or hypothyroidism for cardiovascular outcomes or mortality. The distribution of euthyroid and hypothyroid subjects was not markedly different than ours (euthyroid 76.4%, SCH 22.4%, and hypothyroid 1.3%) and there was no association in subjects >65 years. We have seen association even in this subgroup of patients but association was weaker than in younger patients. Walsh studied 2108 subjects in the Australia-based Busselton Health Study, who had thyroid function tests run on archived blood samples from 1981. In a 20-year follow-up (excluding subjects who had known CHD at baseline), they reported a modest increase in CHD mortality (RR: 1.5, 95% CI: [1.0–2.4], p = 0.08) (23). Rodondi studied 2730 subjects aged 70–79 and noted increased risk for heart failure with TSH >7 mIU/L, but no increase in cardiovascular or all-cause mortality (3). The absence of observed increase in mortality in these latter two studies may be explained by the fact that they included community cohorts and older-aged subjects. Iervasi et al. analyzed 3121 “cardiac patients” and reported that SCH (defined as TSH between 4.5–10 μU/mL and free thyroxine/T3 in the reference ranges) was associated with more than twofold increased risk in cardiovascular disease mortality (RR = 2.40, 95% CI: [1.36–4.21], p = 0.02) (43). As the Iervasi study included subjects with cardiovascular disease, the CHD risk profile is more likely to be consistent with our own patients. The reported mortality is comparable. Imaizumi et al. analyzed 2856 Japanese subjects (mean age: 58.5 years) not on thyroid replacement and demonstrated a twofold increase in all-cause mortality in men (not in women) who had TSH >5 mU/L after 10 years of follow-up (46). As in our study, they adjusted mortality outcomes for several CHD risk factors. The fact that women, in general, are at lower risk for CHD and the smaller study size may explain the differences between this study and our observation of increased mortality risk in both men and women.
Limitations
Despite the fact that the present study has more than twice as many subjects as the studies cited earlier, some limitations do need to be acknowledged. We cannot characterize mortality by cause, because not all subjects are followed in our clinic after their initial visit and our institutional review board approval is limited to information contained in our database. Similarly, we do risk adjustments on the basis of baseline variables and cannot assess the effects of interventions that may modify risk as a result of our treatment strategies. Finally, we have made the assessment of thyroid status on the basis of a single TSH value. The assay is a robust third-generation method, but biologic variation might result in assignment of some patients to another thyroid status had we done multiple determinations. It is uncertain whether the addition of thyroxine measures to our classification scheme would have affected our classification. Patients with a low free thyroxine and elevated TSH values would have likely been reclassified as hypothyroid; it is unlikely that this would have affected the results in a study of >6000 patients.
Summary
The results of this study support existing data that hypothyroidism and moderate SCH are associated with increased mortality. Consistent with other reports, our observations are most robust in patients under the age of 65 years and in patients at high risk for CHD. Our data do not confirm mortality risk for patients with mild SCH (TSH: 3.1–6.0 μU/mL) and thus do not support recommendations to treat patients with such values with thyroid replacement therapy.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.