
Abstract
Background:
Medullary thyroid carcinoma (MTC) is a neuroendocrine tumor (NET) that arises from the parafollicular cells (C-cells) of the thyroid gland which produces calcitonin (CT) and is, therefore, a serum and immunohistochemical biomarker of MTC. Here, we describe a patient with another form of NET arising with the thyroid gland.
Patient Findings:
This is a forty-year-old woman who underwent total thyroidectomy for a thyroid nodule that had features of an NET on fine needle aspiration. Her serum CT and carcinoembryonic antigen were normal. Surgical pathology showed a well-differentiated NET with immunohistochemical stains positive for markers of follicular cells (thyroglobulin and synaptophysin), positive for neuroendocrine markers (neuron specific enolase and chromogranin A), but negative for CT, the defining marker of MTC.
Conclusions:
We describe a rare case of a nonmedullary NET of the thyroid gland arising from thyroid follicular cells, not parafollicular cells. We suggest that calcitonin-negative neuroendocrine tumor of the thyroid gland (CNNETT) may be an entity that has not been recognized in the literature. This distinction between MTC and CNNETT may be important, as the treatment and prognosis may differ.
Introduction
Patient
The patient was healthy, 40-year-old woman who presented with an incidental right thyroid nodule on MRI of the cervical spine for evaluation of neck pain. She denied any history of radiation exposure, hoarseness, dysphagia, weight loss, flushing, or diarrhea. Her medical history as well as that of her family was unremarkable for any endocrine disorders. Her examination did not reveal any palpable thyroid masses or cervical lymphadenopathy. Ultrasound revealed a solitary hypoechoic 2.0 cm right thyroid nodule (Figure 1). Fine needle aspiration (FNA) was performed, which showed findings suspicious for a poorly differentiated carcinoma with neuroendocrine differentiation. A CT of the head, neck, chest, abdomen, and pelvis demonstrated a 1.9 × 1.5 cm right thyroid nodule and neither lymphadenopathy in the six lymph node basins of the neck nor any other pathology. MRI confirmed the 1.6 × 1.3 cm thyroid nodule with no significant cervical lymphadenopathy. Positron emission tomography (PET) scan and Octreotide scan were negative. Her thyroid function levels, urine and plasma metanepharines, parathyroid hormone (PTH), and calcium were all within normal limits, as well as carcinoembryonic antigen (CEA) < 0.5 ng/ml (normal 0.0–2.5 ng/mL) and serum CT being 2.1 pg/mL (normal 0.0–5.0 pg/mL). The patient did not have a preoperative thyroglobulin level. The patient's RET proto-oncogene mutation assay was negative for mutations in exons 10, 11, 13, 14, 15, and 16 (Mayo Medical Laboratories, Rochester, MN). Sequencing of these mutations of the RET gene will detect approximately 88%, 95%, and 98% of mutations causative for familial MTC (FMTC), MEN 2A, and MEN 2B, respectively (4).
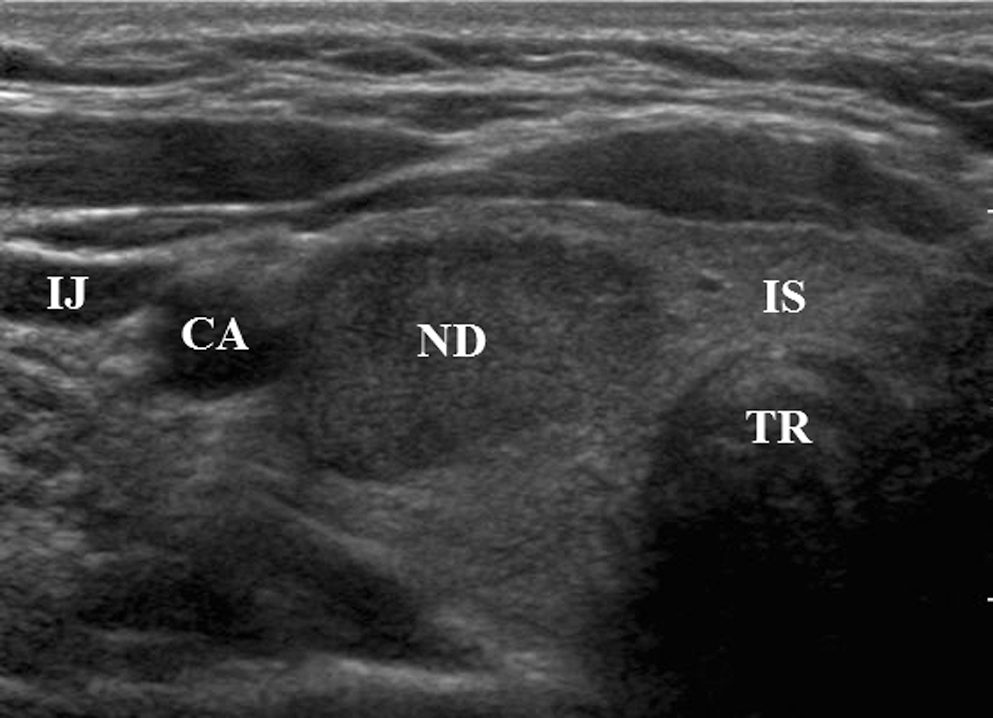
Ultrasound of right thyroid lobe. ND, nodule; TR, trachea; IS, isthmus; IJ, internal jugular; CA, carotid artery.
The patient underwent total thyroidectomy in April 2009. On histopathologic examination, the right thyroid nodule measured 1.5 × 1.5 × 1.2 cm. Hematoxylin and eosin stains demonstrated fairly uniform round and polygonal cells with salt and pepper chromatin with small round nucleoli arranged in trabeculae consistent with a well-differentiated NET. No mitotic activity, vascular invasion, or necrosis was identified. No lymph nodes were included in the specimen. Pathologic and clinical tumor stage was T1N0M0.
Tumor immunohistochemistry is detailed in Table 1. FNA immunohistochemistry was positive for synatophysin, pankeratin, CK8, and CK18 and negative for CT. The surgical pathology immunohistochemistry stained positive for thyroglobulin, NSE, and synaptophysin and weakly for chromogranin A. The staining was negative for CT. The antibody utilized for the CT reaction was a rabbit polyclonal anti-CT antibody, (Ventana Medical Systems Inc., Tucson, AZ), which was accurately tested for both positive and negative controls. The immunohistochemistry slides are in Figs. 2 –6.

Hematoxylin and Eosin 100 ×. The carcinoma consists of uniform round to oval nuclei with finely stippled chromatin (salt and pepper) with occasional nucleoli.
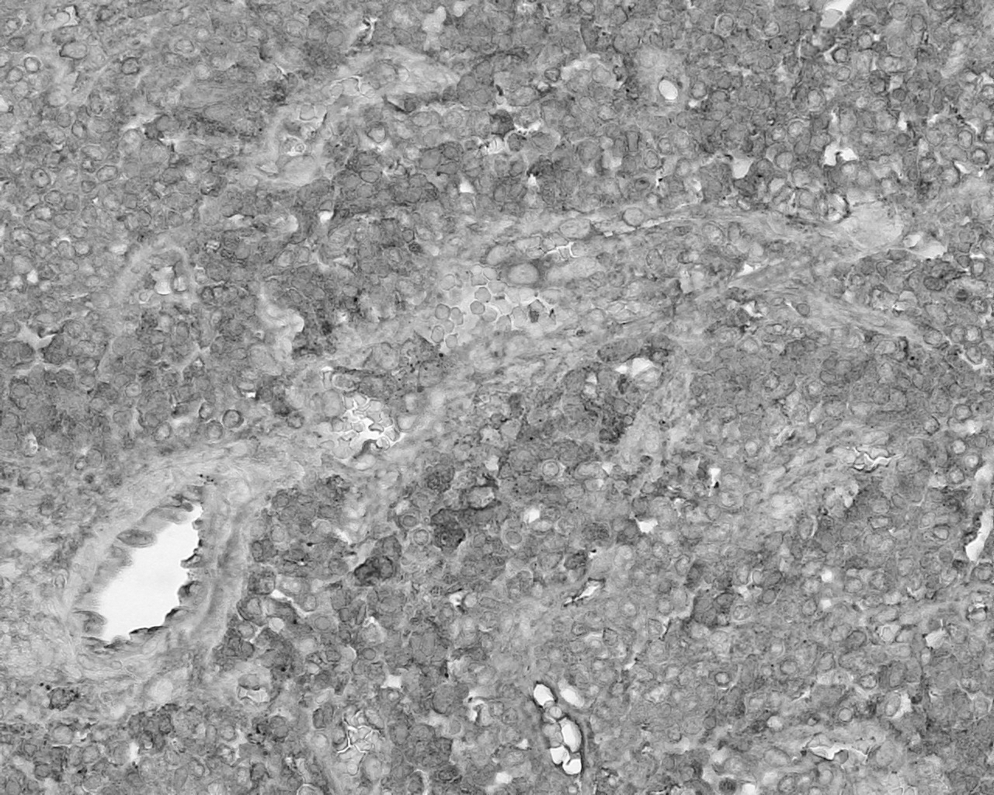
Thyroglobulin 100 ×. Immunohistochemistry (IHC) for thyroglobulin shows strong cytoplasmic staining of the tumor cells.
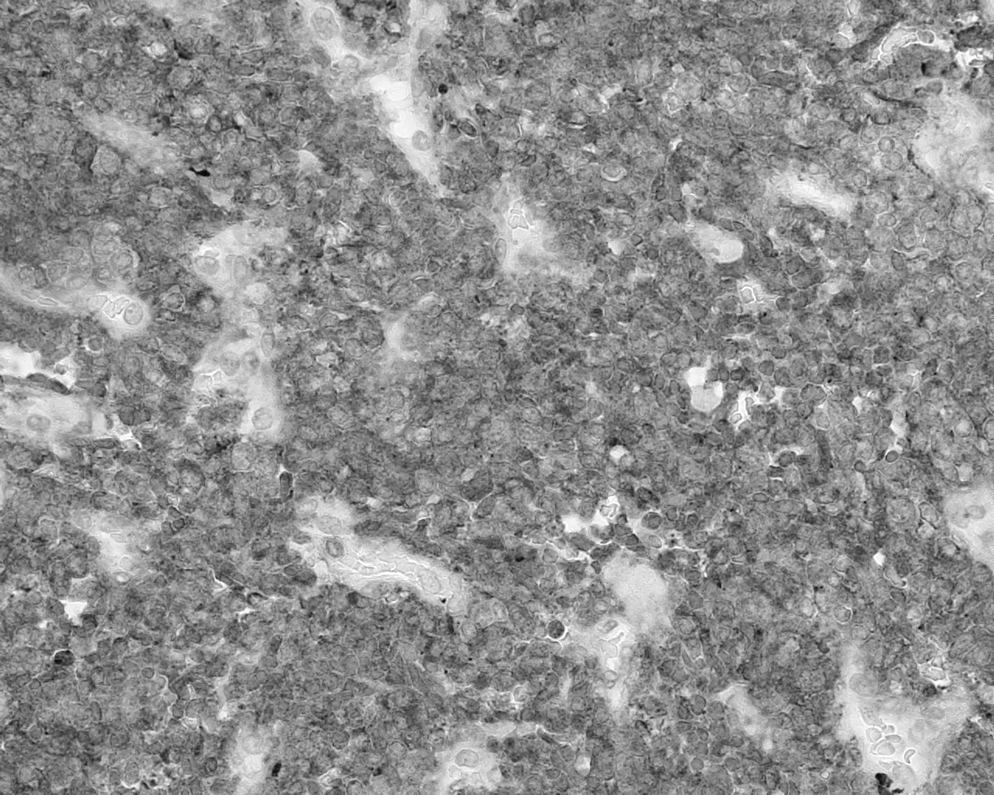
Synaptophysin 100 ×. IHC for synaptophysin has granular cytoplasmic staining of the neurosecratory granules.

Neuron specific enolase 100 ×. IHC for neuron specific enolase has strong cytoplasmic staining.
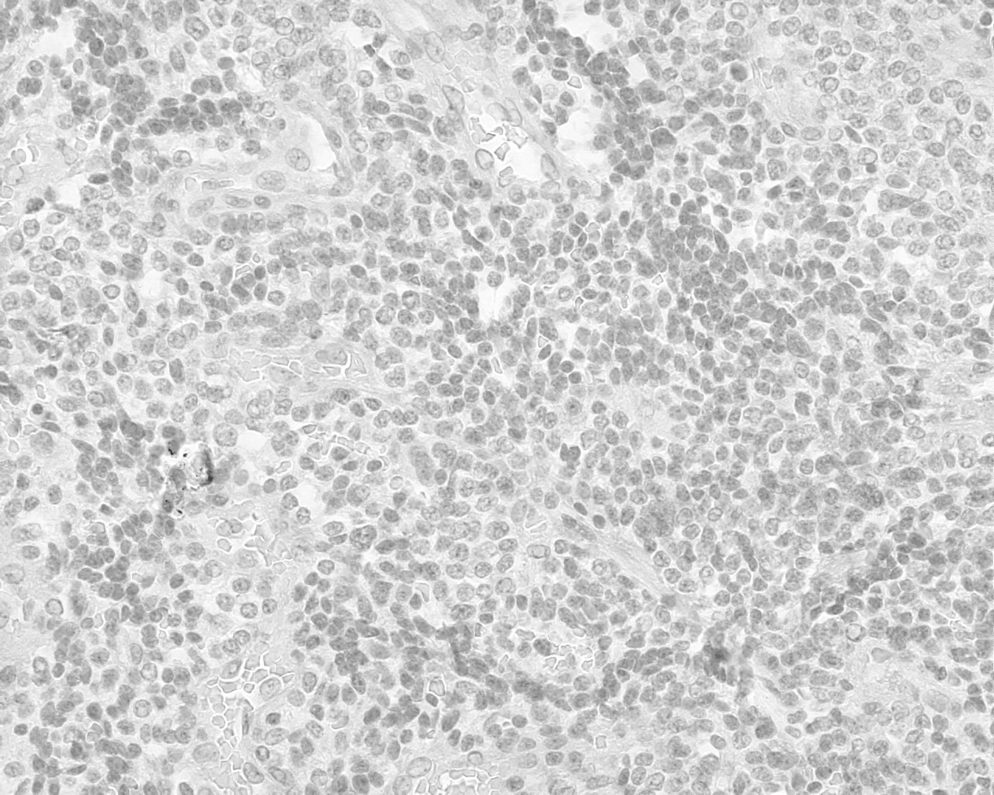
Calcitonin 100 ×. IHC for calcitonin has no cytoplasmic staining.
NET, neuroendocrine tumor.
Post-operatively, the patient did not receive iodine-131 nor any adjuvant treatment. Follow-up serum CT remained undetectable at < 2.0 pg/mL, and serum thyroglobulin was undetectable at < 0.1 μg/L at 4 months postoperatively. She had no clinical evidence of tumor recurrence in the neck at 1 year follow-up exam.
Discussion
Primary thyroid malignancies include papillary, follicular, anaplastic, medullary, and thyroid lymphoma. Metastases to the thyroid from adenocarcinomas, squamous cell carcinomas, and sarcomas have been reported (5 –7).
There have been a few reports of NET metastases to the thyroid from gastroenteropancreatic NET (8,9). Leboulleux et al. reported six patients with thyroid metastases from gastroenteropancreatic-NET where the primary site was from the lung in one case, one from the thymus, one from the pancreas, and the other unknown. All six patients had thyroid tissue that had immunohistochemical stains positive for NSE and chromogranin A, and five had negative staining for CT (8). Similarly, Matias-Guiu et al. reported six cases either carcinoid or NET that metastasized to the thyroid. The primary source was identified in five of the cases, two from bronchial origin, two pulmonary, one intraabdominal, and one undetermined. They concluded that their patients' tumors were metastatic NET to the thyroid based on lack of immunoreactivity for CT and CEA despite morphological characteristics that are consistent with MTC (9). It is conceivable that those patients whose primary tumor was never discovered were, in fact, calcitonin-negative tumors of the thyroid gland.
NET arise from the embryonic neural crest and are present in many organs, especially in the midline organs including the esophagus, stomach, pancreas, intestine, and lung (10). Less common sites of NET include the pituitary, adrenal, cervix, skin, and thyroid. Neural crest tissue form CT-producing C-cells, parafollicular cells, which migrate and fuse with the primordial thyroid gland. These give rise to MTC cells, which secrete CT (11).
The distinction between NET and MTC is challenging, as both have similar morphological features. Morphologically, both cell types can have spindle-shaped and round cells in trabecular arrangements often containing amyloid (12). Both cells stain positive for chromogranin-A, NSE, synaptophysin, and occasionally CEA (13). The diagnosis of NET should be suspected when the cells lack immunoreactivity for CT and are positive for thyroglobulin. In our case, the tumor was an NET of the thyroid, which was CT negative on immunohistochemistry and positive for markers of follicular thyroid cells, arguing for an NET arising from the diffuse neuroendocrine system of thyroid follicular cell origin rather than from true parafollicular cells.
This distinction between MTC and CNNETT is important, as the treatment and prognosis may differ. Currently, CT measurement is utilized as a reliable tumor marker for MTC due to the high (98%) sensitivity compared with FNA cytology sensitivity of 63% (14,15). The lack of tumor marker production from CNNETT makes surveillance for disease recurrence challenging, and further studies are needed to investigate the pathophysiology of these tumors that could potentially aid in determining prognosis and treatment.
Footnotes
Disclosure Statement
The authors of this manuscript have no competing financial interests. They have no commercial associations that might create a conflict of interest in connection with the submitted manuscript.