
Abstract
Background:
Thyrotoxicosis caused by destructive thyroiditis is self-limited and results from the subacute release of preformed thyroid hormone. Common etiologies include painful subacute thyroiditis and silent (painless) subacute thyroiditis (including postpartum thyroiditis, amiodarone-associated destructive thyroiditis, and lithium-associated thyroiditis). Thyrotoxicosis commonly evolves slowly over a matter of weeks.
Patient Findings:
We report a unique case of severe thyrotoxicosis caused by acute- onset painful destructive thyroiditis in a patient who received large amounts of nonionic contrast dye Hexabrix® for cardiac catheterization. The results of thyroid function and physical examination were normal before the catheterization.
Summary:
The acute onset of severe thyroid pain, rapid increase in serum Free Thyroxine Index, and thyroglobulin concentrations with a triiodothyronine to free thyroxine index ratio of <20 to 1 were compatible with an acute onset destructive thyroiditis, likely related to direct toxicity from the iodinated contrast material.
Conclusions:
In light of the large number of patients who receive these contrast agents during cardiac catheterization, clinicians should be advised of this potentially serious complication, particularly in the setting of unstable cardiac disease.
Introduction
The most common variants of destructive thyroiditis are painful subacute thyroiditis (DeQuervain's thyroiditis, granulomatous thyroiditis, and postviral subacute thyroiditis) (2), and painless subacute thyroiditis (3), which includes postpartum thyroiditis (4), lithium-associated thyroiditis (5), and amiodarone-associated destructive thyroiditis (6). Amiodarone-associated destructive thyroiditis is occasionally painful (7). Other causes of destructive thyroiditis are included in Table 1 [modified from refs. (8,9)]. Patients with destructive thyroiditis typically have a ratio of circulating triiodothyronine (T3) (in ng/dL) to thyroxine (T4) (in μg/dL) of <20:1 in contrast to a ratio of >20:1 in Graves' disease or toxic nodular goiter (10).
We report a unique case of acute onset painful destructive thyroiditis in a patient who received large amounts of nonionic contrast dye (Hexabrix®; Guerbet LLC, Bloomington, IN) for cardiac catheterization. The results of his thyroid function tests and physical examination were normal before the catheterization. The acute onset of severe thyroid pain, accompanied by a rapid increase in serum free T4 index (FT4I), and serum (T3) and thyroglobulin concentrations, is compatible with an acute onset destructive process involving the thyroid (11). The serum T3:FT4I ratio was <20:1. The acute destructive thyroiditis was most likely related to a direct toxic effect of iodinated contrast material.
Iodine-induced hyperthyroidism (“Jodbasedow”) (12,13) has been reported in patients with a variety of underlying thyroid diseases, most commonly those with thyroid autonomy due to nodular disease, but occasionally in those with so-called latent Graves' disease (14). Amiodarone destructive thyroiditis often occurs years after initial amiodarone exposure (15). In our patient, thyrotoxicosis developed in an explosive fashion several days after iodinated contrast exposure.
Case Report
A 30-year-old obese Kuwaiti man was admitted to the Massachusetts General Hospital (MGH) for evaluation after an inferior myocardial infarction. At age 26 he had a coronary artery bypass graft for three-vessel coronary artery disease at another institution. Details about that admission and the nature of the contrast agent used during his catheterization were not available. He continued to smoke and was physically inactive.
Six weeks before admission the patient developed severe chest pain and was found to have an acute inferior myocardial infarction. He received thrombolytic therapy with streptokinase and heparin. He did not receive any iodinated contrast materials at that time. On admission to MGH, the patient was asymptomatic.
There was no history of thyroid disease. His family history was negative for thyroid disease and positive for coronary artery disease. On admission, his medications included lovastatin 40 mg p.o. daily, aspirin 81 mg p.o. daily, atenolol 50 mg p.o. daily, and isosorbid 10 mg p.o. three times daily. He had no known allergies. He had never received amiodarone. The only abnormality noted on his admission physical examination was obesity.
On the day of admission (Table 2, day 1), the patient underwent a coronary catheterization. The procedure lasted from 11:50 am to 3:30 pm and was accompanied by an angioplasty and placement of four intra-coronary stents. He received 290 mL of contrast dye (Hexabrix) during the catheterization. That night, he developed crushing substernal chest pain, unrelieved by medication.
Normal range in parentheses.
TSH, thyroid-stimulating hormone; FT4I, Free Thyroxine Index; TT3, total triiodothyronine.
On day 2, he underwent a repeat cardiac catheterization (midnight to 2:30 am) with placement of one additional intra-coronary stent. During that procedure, he received an additional 265 mL of contrast dye (Hexabrix). In addition, he received two 30 mg intravenous doses of solumedrol, heparin, intravenous nitroglycerine, and oral ticlodipine and diphenhydramine. The patient was sedated and remained at bed rest for the remainder of the day.
On the morning of day 3, over a 2-hour period, the patient developed a severe headache and neck pain radiating to his ears. The pain was exacerbated with swallowing. By early afternoon his temperature had risen to 101.1°F. At that time his neck was described as diffusely tender. His pain was very severe but stable over 12 hours and then began to abate. Blood cultures were obtained and he was empirically treated with intravenous cefazolin 1 g every 8 hours.
On day 4, the endocrine service was consulted. At that time he denied recent change in weight, energy level, or bowel movements. There was no recent history of anxiety, perspiration, palpitations, headaches, rhinorrhea, cough, or eye changes. He had no history of head or neck irradiation, or thyroid enlargement and had never been found to have hyperthyroidism or hypothyroidism.
On physical examination, his temperature was 101.2°F, his heart rate was 80 on a beta blocker, and he appeared acutely ill. There was no exophthalmos or conjunctival injection. There was no pharyngeal inflammation. The thyroid was mildly but diffusely enlarged (estimated at 25 g) and exquisitely tender throughout, without overlying skin erythema or induration. No nodules were palpated. There were no cutaneous lesions. The relaxation phase of his deep tendon reflexes was normal.
Laboratory testing included normal renal function and electrolytes. His white blood count was 12,000 and his sedimentation rate was 26 mm per hour (normal range 0–11). Thyroid function tests were obtained on day 4 and were then requested and performed on stored blood samples from days 2 and 3 (Table 2 and Fig. 1). The serum thyroid stimulating hormone (TSH) declined from normal (1.34 mU/L) on day 3 to markedly suppressed on day 5 (0.03 mU/mL). The FT4I rose from mildly elevated (11.7) on day 2 to markedly elevated (30.8) on day 6. The serum T3 concentration rose from normal (139 ng/dL) on day 2 to a markedly elevated peak of 508 ng/dL on day 4. Serum thyroglobulin was elevated at 346 ng/dL on day 2 and rose to an extraordinarily high concentration of 48,049 ng/dL on day 4.
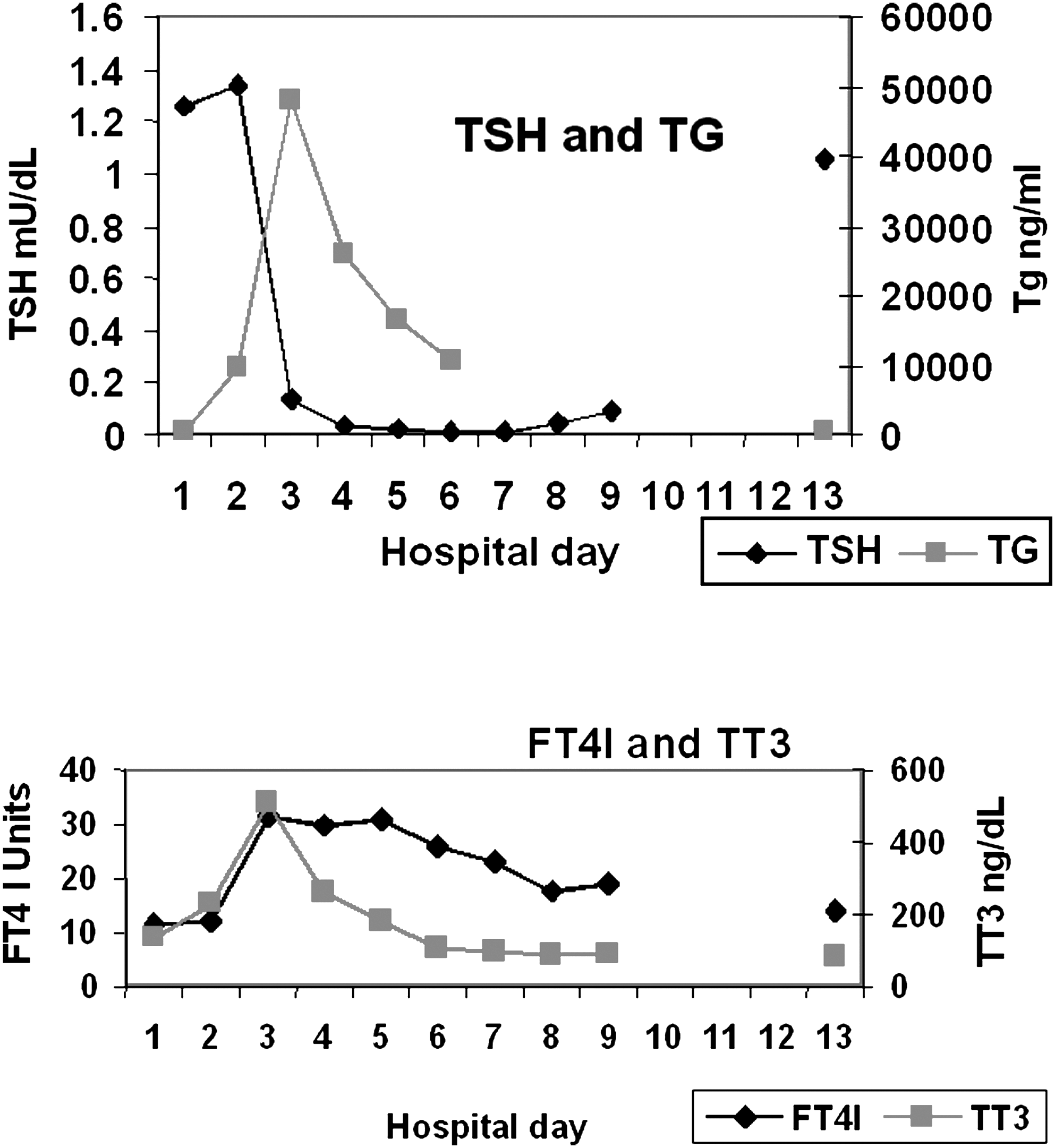
Serial thyroid function tests. Thyroid-stimulating hormone (TSH, in mU/mL, nl 0.5–5.0), thyroglobulin (TG in ng/dL), Free Thyroxine Index (FT4I, nl 4.5–10.9; calculated as the product of the serum T4 and the T3Resin Index), and total triiodothyronine (TT3 in ng/dL, nl 60–181) during the patient's follow-up. The patient received the initial dose of Hexabrix® on day 1 and a second dose on day 2. Symptoms were first recorded on day 3. Thyroid function tests from day 2 and day 3 were down on stored blood samples.
A thyroid ultrasonography showed a normal-sized thyroid with normal echo-texture without nodules or cysts. Color flow Doppler was not performed. The clinical impression was thyrotoxicosis due to destructive thyroiditis, likely related to iodinated contrast material.
Therapy was initiated with prednisone 30 mg PO daily, cholestyramine 100 mg PO every 6 hours, and iopanoic acid 500 mg PO twice daily. His beta blockade was increased.
By day 5, the patient's thyroid pain and tenderness had abated. He appeared to be euthyroid at that time. Prednisone was continued at 30 mg daily for 4 days, and then tapered and discontinued over 4 days. Cholestyramine and iopanoic acid were continued for 10 days. His thyroid function tests are reviewed in Figure 1 and Table 2. The patient continued to note increased perspiration but was otherwise without signs or symptoms of hyperthyroidism.
The persistent elevation of FT4I and thyroglobulin on day 7 reflects the long half-lives of T4 and thyroglobulin.
One year after his catheterization, the patient was clinically euthyroid and had a normal serum TSH (0.55 mU/mL) and serum thyroglobulin (16.7 ng/mL) on no thyroid medication. Thyroid autoantibodies were absent.
Comment
Our patient developed thyrotoxicosis over several days after receiving the iodine-containing contrast agent Hexabrix. The elevated serum thyroglobulin on day 2 suggests that this process began within 24 hours of his second catheterization. The normal serum TSH immediately postcatheterization and the normal thyroid ultrasonography suggest that he did not have underlying thyroid disease.
Hexabrix is a 59.4% solution of meglumine and sodium salts of ioxaglic acid that has 40% of the osmolality of conventional radiocontrast agents. Ioxaglic acid has two benzene rings, each substituted with three iodine atoms. It contains 320 mg of iodine per milliliter (16). Our patient received a total iodine load of 177.6 g over 24 hours. Conventional arteriography with Hexabrix generally administers <90 g of iodine. The amount of free iodine released from ioxaglic acid is unknown. Arteriography with Hexabrix in a group of 22 patients was not associated with change in thyroid function tests (T4, T3Resin Uptake, and Free T4) taken at various intervals up to 56 days after the procedure (15). For comparison, the normal dietary iodine intake in the United States is 150–300 μg daily (17).
Iodine is a necessary substrate for thyroid hormone synthesis but also modulates thyroid function. In the setting of an acute iodine load, the normal thyroid transiently decreases the synthesis of thyroid hormones (due in part to the Wolff-Chaikoff effect) but then recovers due to a decrease in the thyroid sodium/iodide symporter which causes a decrease in iodine transport into the thyroid and resumption of normal thyroid hormone synthesis (18). When individuals with normal thyroid glands are exposed to an iodide load, thyroid function remains in the normal range (19).
In contrast, iodine administration to individuals with thyroid autonomy may lead to hypersecretion of thyroid hormone, known as the Jod-Basedow effect (20). Iodine-induced hyperthyroidism has been reported in patients with a variety of underlying thyroid diseases, but primarily occurs in individuals with nodular thyroid disease (21). Iodine may also precipitate Graves' disease in predisposed individuals (22). The severity and duration of the hyperthyroidism is highly variable and partly depends on the magnitude of iodine exposure and on pre-existing thyroid autonomy (23). Prophylactic use of anti-thyroid drugs has been suggested by some authors for patients who are at risk for developing hyperthyroidism with iodine exposure (24).
Iodine-induced hyperthyroidism is thought to be uncommon after coronary angiography, even in iodine deficient populations, where nodular thyroid disease is more common (25). However, severe cases have been described (26). A variety of contrast agents have been used in these reports. In one prospective study 3% of elderly patients receiving nonionic contrast radiography developed hyperthyroidism (27). The elderly may be particularly vulnerable. Iodine-induced hyperthyroidism typically develops more slowly (usually weeks to months) and persists for a longer period, and is not associated with thyroid pain (28,29). Our patient's onset of thyrotoxicosis was rapid (days) and was accompanied by severe thyroid pain and fever. Furthermore, our patient did not have underlying nodular disease, making Jod-Basedow unlikely.
The time course of thyrotoxicosis in our patient is most consistent with acute release of pre-formed thyroid hormone, an example of so-called destructive thyroiditis. The differential diagnosis of destructive thyroiditis is summarized in Table 1 (7,8,30,31).
The most common cause of painful destructive thyroiditis is postviral subacute thyroiditis (2). In this disorder, thyrotoxicosis typically develops over weeks, often after a prodromal viral syndrome. The 24-hour radioiodine uptake is nil, the sedimentation rate is markedly elevated, transient hypothyroidism often occurs, and persistent thyroid function abnormalities are rare. Fever is common. We cannot exclude an atypical rapid onset of painful subacute thyroiditis in our patient. However, the rapid onset of severe neck symptoms after two cardiac catheterizations, the absence of a viral prodrome, the extremely rapid onset of thyrotoxicosis, and the near-normal sedimentation rate all argue strongly against postviral painful subacute thyroiditis. Because of the high iodine content of the Hexabrix a 24-hour radioactive iodine uptake was not performed and would likely have been nil regardless of the etiology of the thyrotoxicosis (32).
The thyroid in Graves' disease may be painful and tender (33) and have associated painful thyroiditis (34). Fukata et al. (35) described four patients with painful Graves' disease who went on to spontaneous permanent hypothyroidism, but this evolution took 2–3 months. The rapid resolution of thyrotoxicosis in our patient is not consistent with either painful Graves' disease or its variant that proceeds to hypothyroidism.
Painful radiation thyroiditis may also follow radioactive iodine therapy for Graves' disease (36,37). Radiation thyroiditis related to external beam therapy is generally not painful (38).
Other causes of painful destructive thyroiditis are rare and include malignant pseudothyroiditis due to primary thyroid malignancies or malignancies metastastic to the thyroid (39), pneumocystis and other infectious causes of acute suppurative thyroiditis (40,41), amiodarone destructive thyroiditis (6), and painful autoimmune subacute thyroiditis, which develops spontaneously (42 –44) or after antithyroid drug administration (45) and rarely postpartum thyroiditis (46). Amyloid goiter is extremely rare and may be associated with painful destructive thyroiditis. Amyloid goiter has a persistently abnormal enlarged thyroid with diffuse hyperechogenicity on ultrasonography and is usually a manifestation of systemic amyloidosis (47 –49). Our patient did not have a thyroid malignancy, evidence of infection, treatment with amiodarone or radioactive iodine, an abnormal thyroid ultrasound, or positive antithyroid antibodies, thus effectively excluding these diagnoses.
Silent (painless) subacute thyroiditis is a form of painless destructive thyroiditis, whose time course otherwise mimics that of painful subacute thyroiditis. Acute thyrotoxicosis may occur after thyroid manipulation during parathyroid or other neck surgery (palpation thyroiditis), but pain is generally not present (50).
Destructive thyroiditis, which is usually painless, may occur in normal thyroid glands after exposure to iodinated agents. Almost all reported cases are related to amiodarone administration (5). Amiodarone destructive thyroiditis correlates best with the long-term cumulative amiodarone dosage (14). It may occur after long-term persistent or intermittent exposure or up to 1 year after the drug has been discontinued (51). Amiodarone destructive thyroiditis is thought to represent a direct toxic effect of the drug or its metabolites. Amiodarone destructive thyroiditis is rarely tender (6). Painless destructive thyroiditis has also been reported with the long-acting radiocontrast agent lipiodol and the amebicide iodoquinol (48). Transient painless thyrotoxicosis has also been reported in two individuals after long-term kelp administration (52). Whether these cases represent destructive thyroiditis or another form of thyrotoxicosis is uncertain. Edmunds described four patients with severe acute thyroid pain related to potassium iodide administration, which responded to potassium iodide withdrawal (53). Unfortunately, no thyroid blood tests were reported because thyroid function tests were not available except for the protein bound iodine (PBI) in the early 1950s.
The sudden onset of severe thyroid pain, fever, and thyrotoxicosis required urgent therapy in a patient with a recent myocardial infarction. We instituted therapy with prednisone, iopanoic acid, and cholestyramine on day 4. Glucocorticoids, such as prednisone, effectively treat the pain of postviral subacute thyroiditis and lead to a rapid decline in serum thyroglobulin (54). Prednisone shortens the time to euthyroidism in thyrotoxic individuals with painless subacute thyroiditis (55) and partially blocks T4 to T3 conversion (56). Thyrotoxicosis caused by amiodarone-associated destructive thyroiditis is rapidly and effectively treated with prednisone (5,57). Iopanoic acid inhibits the peripheral conversion of T4 to T3 and has been effective in the treatment of painful subacute thyroiditis (58) as well as amiodarone-induced destructive thyroiditis (54). Unfortunately, it is no longer readily available in the United States of America. Although iopanoic acid contains iodine, we do not believe that the thyrotoxicosis in this case was a direct consequence of iodine per se but rather due to the organic iodine containing molecule (Hexabrix) similar to the situation with amiodarone destructive thyroiditis. Hence, we were not concerned about the safety of iopanoic acid for our patient. Cholestyramine has also been shown to accelerate thyroid hormone clearance by the entero-hepatic circulation (59,60). With this regimen, serum T3 returned to normal by day 7 and serum TSH was within normal limits on day 14 although serumT4 and serum thyroglobulin remained elevated for a longer period due to their longer half-lives.
Serum TSH concentration is accepted as the most sensitive test for the early detection of thyrotoxicosis (61). The patient presented here highlights one of the potential pit-falls of its use. When hyperthyroidism develops abruptly, as was noted in our patient, the fall in serum TSH concentration lags behind the rise in thyroid hormone, although only by a few days in this case. Nonetheless, if serum TSH alone were measured on days 2 or 3, or if a typical TSH-based thyroid function testing algorithm was employed (e.g., measure serum TSH, if within normal limits no other thyroid tests are obtained), the clinician would have been falsely reassured. This case also helps answer the question: How long does it take serum TSH to become suppressed in hyperthyroidism? In this patient, the TSH was below normal within 48 hours of the second cardiac catheterization, and fully suppressed at 0.03 mU/mL within 72 hours. Although serum TSH may remain suppressed for longer periods when hyperthyroidism has been persistent (62), with acute hyperthyroidism as in this case, the TSH returned to normal within 2 weeks.
We believe that the most likely explanation for the thyrotoxicosis in this patient is destructive thyroiditis due to a direct toxic effect of the ioxaglic acid component of the Hexabrix. The need for a second catheterization, with higher than usual amounts of contrast agent, may have contributed to this toxicity. Allergic reactions to Hexabrix have been reported but none have involved the thyroid gland (63,64). Although an allergic reactions to this agent cannot be excluded, this seems less likely. We did not think it was either wise or ethical to re-challenge with Hexabrix. Although Hexabrix-related destructive thyroiditis is likely to be a rare phenomenon, the high frequency of cardiac catheterizations and the potential severe complications of thyrotoxicosis in this setting prompted us to report this event. Prompt and aggressive treatment of thyrotoxicosis in the setting of acute coronary syndromes may be critically important. Clinicians managing patients receiving large doses of iodine-containing contrast agents (particularly Hexabrix) should be aware of this rare but potentially harmful complication of contrast administration.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.