
Abstract
Background:
Subclinical hypothyroidism (SCH) has been associated with atherosclerosis, but the abnormalities in plasma lipids that can contribute to atherogenesis are not prominent. The aim of this study was to test the hypothesis that patients with normocholesterolemic, normotriglyceridemic SCH display abnormalities in plasma lipid metabolism not detected in routine laboratory tests including abnormalities in the intravascular metabolism of triglyceride-rich lipoproteins, lipid transfers to high-density lipoprotein (HDL), and paraoxonase 1 activity. The impact of levothyroxine (LT4) treatment and euthyroidism in these parameters was also tested.
Methods:
The study included 12 SCH women and 10 matched controls. Plasma kinetics of an artificial triglyceride-rich emulsion labeled with radioactive triglycerides and cholesteryl esters as well as in vitro transfer of four lipids from an artificial donor nanoemulsion to HDL were determined at baseline in both groups and after 4 months of euthyroidism in the SCH group.
Results:
Fractional clearance rates of triglycerides (SCH 0.035 ± 0.016 min−1, controls 0.029 ± 0.013 min−1, p = 0.336) and cholesteryl esters (SCH 0.009 ± 0.007 min−1, controls 0.009 ± 0.009 min−1, p = 0.906) were equal in SCH and controls and were unchanged by LT4 treatment and euthyroidism in patients with SCH, suggesting that lipolysis and remnant removal of triglyceride-rich lipoproteins were normal. Transfer of triglycerides to HDL (SCH 3.6 ± 0.48%, controls 4.7 ± 0.63%, p = 0.001) and phospholipids (SCH 16.2 ± 3.58%, controls 21.2 ± 3.32%, p = 0.004) was reduced when compared with controls. After LT4 treatment, transfers increased and achieved normal values. Transfer of free and esterified cholesterol to HDL, HDL particle size, and paraoxonase 1 activity were similar to controls and were unchanged by treatment.
Conclusions:
Although intravascular metabolism of triglyceride-rich lipoproteins was normal, patients with SCH showed abnormalities in HDL metabolism that were reversed by LT4 treatment and achievement of euthyroidism.
Introduction
Elevated low-density lipoprotein (LDL)-cholesterol, the landmark of lipidic change associated with thyroid hormone deficiency, has been consistently documented in patients with SCH and TSH >10 uU/mL (3,7,8), a population that accounts for only 25% of SCH cases. In patients with TSH <10 uU/mL, however, dyslipidemia is not a characteristic finding (7).
LDL and chylomicron remnants are the final catabolic products of the metabolism of triglyceride-rich lipoproteins synthesized in the liver such as very low-density lipoprotein (VLDL) and of chylomicrons produced in the intestine after absorption of dietary fats. In the plasma, these lipoproteins undergo lipolysis in the endothelial surface of the vessels by the action of the enzyme lipoprotein lipase. This enzymatic action is stimulated by apo CII, present on the surface of VLDL, and chylomicron particles, which bind the lipoproteins to the enzyme. This mechanism allows the absorption of the hydrolyzed fats by tissues such as adipose and muscle, in which fats are re-esterified and stored. The triglyceride-depleted remnants, intermediate density lipoprotein (IDL) and LDL, and the chylomicron remnants are finally taken up by different cell membrane receptors that recognize apo B or apo E and internalize the degraded lipoproteins which are chiefly taken up by the liver (9).
The metabolic pathway of triglyceride-rich lipoproteins can be tested in vivo using double-labeled triglyceride-rich emulsions (10). These emulsions are prepared without proteins and after injection in the blood stream, acquire circulating exchangeable apolipoproteins, such as apo CII, which modulates lipolysis, and apo E, which modulates removal of the resulting cellular remnants. The plasma kinetics of the triglyceride-labeled moiety of the emulsion tests the lipolysis process whereas the emulsion cholesteryl ester tests the remnant removal. Although the kinetic behavior of the emulsions resemble that of chylomicrons, since the metabolic pathway is similar to that of VLDL, defects in the VLDL metabolism can also be detected by this method. Delayed lipolysis or removal of remnants from the circulation has been related to the presence of coronary artery disease (CAD) (10,11), intensity of the lesions, and to worse evolution of the disease (10,11).
The metabolism of triglyceride-rich lipoproteins is also related to the metabolism of high-density lipoprotein (HDL). Nascent HDL is produced by the liver and intestine, although it has been postulated that it can also be generated from phospholipids and free cholesterol resulting from lipolysis of triglyceride-rich lipoproteins which aggregate to apo A1, the main apolipoprotein present in HDL. Transfer of lipids occurs between triglyceride-rich lipoproteins and HDL, which results in loss of cholesteryl esters by the HDL and enrichment of triglycerides. Consequently, when triglycerides accumulate in the plasma, the clearance of triglyceride-enriched HDL is increased and HDL levels tend to decrease. These lipid transfers are mediated by transfer proteins, such as cholesteryl ester transfer protein and phospholipid transfer protein. Lipid transfers are, therefore, very important in HDL intravascular metabolism and are determinants in HDL function in reverse cholesterol transport. Since they affect HDL composition, other important antiatherogenic functions of this lipoprotein may also be affected, such as antioxidant, anti-inflammatory, antithrombotic, and vasodilation actions.
The aims of this study were threefold. The first was to assess the intravascular metabolism of triglyceride-rich lipoproteins and the transfer of lipids to HDL in women with SCH and age-paired controls in order to investigate metabolic disturbances with atherogenic potential that may be undetected in routine laboratorial evaluation. The second was to determine in both groups the HDL size and the activity of paraoxonase 1 (PON1), an antioxidant enzyme associated with HDL. The third was to assess the effect of levo T4 (LT4) replacement and achievement of euthyroidism on all these parameters.
Material and Methods
Patients
Twelve consecutive women with newly diagnosed SCH attending the Outpatient Clinic of the Endocrinology Service of the University of São Paulo Medical School Hospital were enrolled. The control group consisted of 10 age-matched women. The diagnosis of SCH was established by at least two consecutive plasma TSH values above 4.20 uU/mL and free T4 levels within the normal range for at least 6 months before enrollment. In eight patients, TSH levels were between 4.21 and 10.0 uU/mL and in four, levels were above 10.0 uU/mL. None of the subjects were pregnant, smokers, had acute illness, or were taking any drug that could interfere with thyroid function, plasma lipids, or with hepatic or renal metabolism pathways, such as lipid-lowering agents or thiazidic diuretics. Clinical parameters of both groups are shown in Table 1.
Data expressed as mean ± standard deviation.
p-Values for comparison between control subjects and SCH subjects before treatment.
p-Values for comparison between SCH subjects before and after treatment.
p-Values for comparison between control subjects and SCH subjects after treatment.
Normal TSH and free T4 range: 0.50–4.20 uU/mL and 0.60–1.54 ng/dL, respectively.
SCH, subclinical hypothyroidism; BMI, body mass index; TSH, thyrotropin; T4, thyroxine; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Exclusion criteria included serum LDL-cholesterol >160 mg/dL, triglycerides >200 mg/dL, body mass index above 30 kg/m2, diabetes mellitus, systemic lupus erythematosus, cancer, anemia, pancreatitis, renal or liver disease, hypoalbuminemia, or other systemic diseases.
Blood was collected from all subjects at 8:00 a.m. after a 12-hour overnight fast for assessment of TSH, free T4, PON 1 activity, HDL size, and assessment of lipid transfers to HDL. After blood collection, the emulsion plasma kinetic study was performed as described next.
Triglyceride-rich emulsion preparation and plasma kinetics
Preparation of triglyceride-rich emulsions labeled with 14 C-cholesteryl oleate (CE) and 3 H-triolein (TG) (Amersham) was performed as previously described (10).
Patients received a bolus injection (200–300 μL) of radiolabeled emulsion containing 14 C-CE 74 kBq (2 μCi) and 3 H-TG 148 kBq (4.0 μCi) in the antecubital vein. The contralateral antecubital vein was cannulated, and a slow infusion of saline solution without heparin was started to maintain catheter patency for blood collection for radioactivity measurement. The total saline volume infused did not exceed 100 mL. Blood samples were collected at 2, 4, 6, 10, 15, 20, 30, 45, and 60 minutes after injection of the emulsion. Plasma was separated by centrifugation, and an aliquot of 1 mL was transferred to counting vials containing 7 mL of a scintillation solution (Ultima Gold XR-Perkin Elmer). Radioactivity in the samples was determined using a Packard 1660 TR spectrometer (Packard). The estimation of the in vivo time course of the metabolism of the chylomicron-like emulsion was evaluated by compartmental analysis as previously described (10).
Treatment with LT4
On the day after blood collection, patients with SCH were started on LT4 25 μg a day. Plasma TSH levels were measured at 6-week intervals for dose adjustment until plasma TSH reached a level between 0.4 and 4.0 uU/mL. The dose of LT4 was then maintained to keep plasma TSH levels within this proposed range for 4 months.
Plasma kinetic study, lipid transfer assay, and the other assessments were repeated in the SCH group after 4 months of euthyroidism, as just described. Baseline and post-treatment results were compared.
All patients were advised to maintain their dietary habits during the study period.
Radiological safety and ethics
The assessment of the radiological dose injected as emulsion label was performed according to the guidelines of the International Commission on Radiological Protection and was below the Annual Limit for Intake of Radionuclide (50 mSv) as previously discussed (10). For each emulsion kinetic study, the radioactive dose for 14 C-CE and 3 H-TG was 0.02 and 0.0012 mSV, respectively.
All the procedures in this study were in accordance with the guidelines of the Helsinki Declaration on human experimentation. The study protocol was approved by the Ethical Committee of the Medical Hospital of the University of São Paulo, and written informed consent was obtained from all participants.
Serum biochemical determinations
Blood samples were collected on ethylenediaminetetraacetic acid and centrifuged at 1500 g for 10 min at 4°C for plasma separation. Plasma lipids, apo A1, and apo B were measured by standard commercial kits (Roche).
Serum TSH and free T4 were assayed by fluoroimmunoassay (AutoDELFIA equipment, AutoDELFIA Ultrakit, Wallac Oy) ≤4.4% and 3.4% for free T4, respectively.
PON1 activity was measured by adding serum to 1 mL Tris-HCl buffer (100 mmol/L, pH 8.0) containing 2 mmol/L CaCl2 and 5.5 mmol/L paraoxon (Sigma Chemical Company). The generation of p-nitrophenol was measured at 405 nm, at 37°C in a microplate reader (Bio-Rad, Benchmark) (12).
HDL particle size and assay of lipid transfer to HDL
The diameters of HDL particles were determined by ZetaPALS Zeta Potential Analyzer (Brookhaven Instruments Corporation) as described elsewhere (13).
The in vitro assay of the simultaneous transfer of radioactively labeled phospholipids, triglycerides, and free and esterified cholesterol lipids from an artificial nanoemulsion to the HDL plasma fraction was performed as described by Lo Prete et al. (14). In brief, the donor lipidic nanoemulsion containing the labeled lipids was incubated during 1 hour with whole plasma. After chemical precipitation of the nanoemulsion and the apo B lipoprotein fractions, the supernatant containing the HDL fraction was counted for radioactivity in a scintillation solution, and the percentage radioactivity of each lipid that transferred from the nanoemulsion to HDL was then estimated.
Statistical methods
Results were presented as means ± standard deviation. For fractional clearance rate (FCR), variables transformation - log10(X) was applied. Associations between the transfer of lipids from the artificial nanoemulsion to HDL and other variables were determined by using Pearson's correlation coefficient. Differences in results between SCH and controls were assessed by Student's t-test. Data from the SCH group before and after treatment were analyzed by paired Student's t-test. p-Values <0.05 were considered statistically significant.
Results
After treatment with LT4, serum TSH levels normalized in all patients in the SCH group. As expected, free T4 values were normal before and after treatment (Table 1). As shown in Table 1, baseline serum levels of LDL-cholesterol, HDL-cholesterol, triglycerides, apo A1, and apo B were similar in patients with SCH and in controls. In the SCH group, these values remained unchanged after LT4 treatment (p = non significant for all).
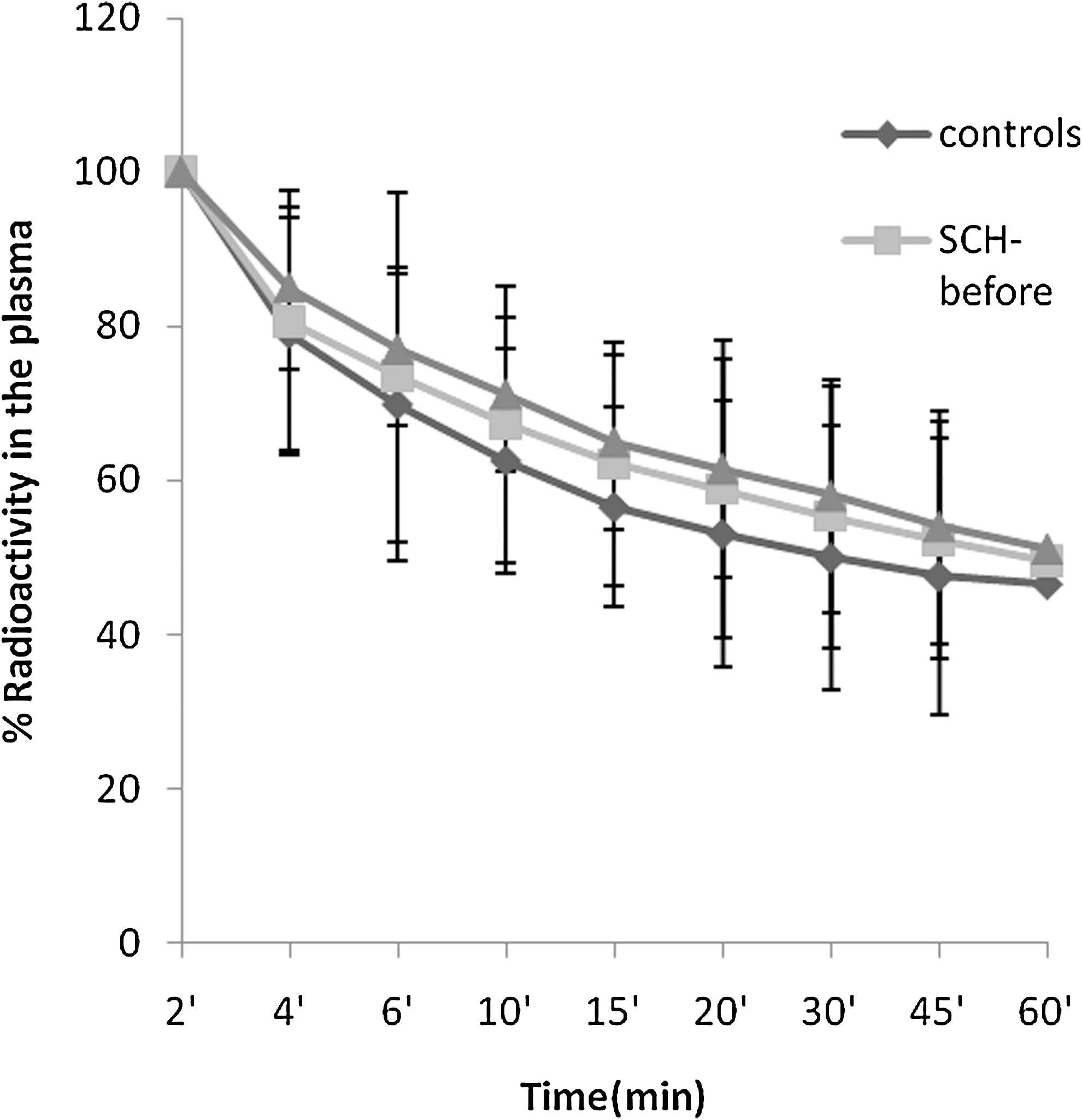
Plasma decay curves for emulsion triglycerides and cholesteryl esters were similar in patients with SCH and in controls at baseline and did not differ when analyzed before and after LT4 treatment (Figs. 1 and 2). As shown in Table 2, FCR of radioactive-labeled triglycerides and cholesteryl esters were similar in patients with SCH and in controls. After treatment with LT4 and achievement of euthyroidism, FCR of both emulsion labels remained unchanged.

Plasma decay curves of the emulsion 3H-triglycerides in the control group and in patients with SCH before and after levothyroxine treatment. SCH, subclinical hypothyroidism.
Plasma decay curves of the emulsion 14C-cholesteryl esters in the control group and in patients with SCH before and after levothyroxine treatment.
Data expressed as mean ± standard deviation.
p-Values for comparison between controls and SCH subjects before treatment.
p-Values for comparison between SCH subjects before and after treatment.
p-Values for comparison between control subjects and SCH subjects after treatment.
FCR, fractional clearance rate; PON1, paraoxonase 1.
Table 2 also shows the percentage of transfer of the four labeled lipids—free cholesterol, phospholipids, cholesteryl esters, and triglycerides—from the artificial donor nanoemulsion to the HDL fraction after incubation of the labeled nanoemulsion for 1 hour with whole plasma. The transfer of both phospholipids and triglycerides was lower in patients with SCH than in controls. However, after LT4 treatment, transfer of both lipids increased in the SCH group and reached similar levels as in controls. Transfer of free cholesterol and cholesteryl esters was similar in both groups and remained unchanged in the SCH group after LT4 treatment.
Size of HDL particles was equal in both groups. Similarly, no differences were seen in PON1 activity between patients with SCH and in controls as well as between pre- and post-treatment values in the SCH group.
Discussion
Several studies have evaluated plasma lipids in patients with SCH with conflicting results. Some have shown a positive correlation between TSH and LDL-C values that has not been confirmed by others. These discrepancies may be attributed to differences among the studies in age, gender, body mass index, and drug use in the patient population (4). Although some authors have found decreased HDL-cholesterol levels in patients with SCH, others have reported normal ones. There is also controversy on the impact of LT4 treatment in HDL-cholesterol levels with some, but not all studies reporting improvement after treatment (15).
Even in the presence of normal plasma lipids, decreased plasmatic clearance of emulsion cholesteryl esters and triglycerides has been associated with CAD (10,16). In studies in which other methodological approaches were used to asses lipoprotein metabolism, accumulation of postprandial remnants and deficient lipolysis were also linked to CAD (17). Sposito et al. have shown that the severity of the CAD, quantified by the Gensini score, was also inversely correlated with clearance of both cholesteryl esters and triglycerides (17). In their study, clearance of cholesteryl ester was the only independent predictor of the presence of CAD. In another study from our laboratory (18), a slower remnant removal was associated with worse clinical outcome after a myocardial infarction episode in patients followed for an average of 4.5 years. Since VLDL and chylomicron remnants can permeate the endothelial wall, be taken up by macrophages, and lead to foam-cell formation (18), these particles carry an atherogenic potential. A delay in their removal from the bloodstream may facilitate both remnant exposure to oxidation in the subendothelial space and deviation from the physiologic prompt removal by the liver, thus causing deleterious effects to the arterial wall (19).
The plasma kinetics of triglyceride-rich emulsions has previously been tested in rats with hypothyroidism induced by propylthiouracil. In this experiment, the clearance of the triglyceride emulsions was normal, but the clearance of the cholesteryl ester was reduced (20). This suggests that, although the lipolysis of the triglyceride emulsions by lipoprotein lipase was not affected by the hormonal deficiency, the resulting remnants were not efficiently cleared from the circulation. Redgrave and Snibson (21) have previously shown similar results after injecting lymph chylomicrons labeled with both triglycerides and cholesteryl esters in thiouracil-treated rats. This remnant-accumulation effect can be attributed to a deficiency in the activity of hepatic lipase, a predominant phospholipase that depends on thyroid hormone for full activity. The partial breakdown of phospholipids that constitute the surface monolayer of the particles of the triglyceride-rich emulsions or lipoproteins is required for the uptake of the remnants by the liver (21). Remnant accumulation in hypothyroidism could also be accounted for the diminished expression in this disease of hepatic LDL receptors (22,23). These receptors take up not only LDL but also IDL and chylomicrons remnants by apo E mediated binding. In nine patients with hypothyroidism, Weintraub et al. showed that LT4 replacement increased removal of postprandial triglyceride-rich lipoprotein remnants after ingestion of a test meal with added retinyl palmitate for chylomicron labeling (24). Although LT4 treatment also decreased postprandial triglycerides, this cannot be necessarily attributed to increased lipolysis. In another study by Tanaci et al. (25), after ingestion of a test meal, triglyceridemia was higher in patients with hypothyroidism than in controls, whereas the triglyceridemia curve of patients with SCH was apparently intermediate and not statistically different from that of controls and from that of patients with hypothyroidism.
In the current study, the kinetics of the emulsion 3 H-triglycerides and 14 C-cholesteryl esters were normal in patients with SCH compared with controls. In addition, LT4 replacement did not result in any further change in the FCR of both triglycerides and cholesteryl esters emulsions. This suggests that the process of lipolysis, which the triglyceride-rich lipoproteins undergo on the capillary endothelium, and the final removal of the resulting remnants by the body tissues, mainly the liver, are unchanged in patients with SCH. In view of these findings, it can be assumed that the mild deficiency in thyroid hormone is not sufficient to allow metabolic changes in triglyceride-rich lipoproteins seen in patients with overt hypothyroidism. This assumption is further supported by the observation that the emulsion metabolism remained unchanged after LT4 treatment.
In contrast, lipid transfers to HDL were compromised in patients with SCH and, after achievement and maintenance of euthyroidism for 4 months, these abnormalities were corrected.
The abnormalities observed in lipid transfers to HDL in patients with SCH may cause disturbances in the metabolism of the lipoprotein that could affect the dynamics of HDL composition and, consequently, the processes of cholesterol esterification and reverse cholesterol transport. In our patients, the transfer of both phospholipids and triglycerides was diminished in comparison with controls. It has been recently shown that enrichment of the HDL fraction with phospholipids increases HDL action in the reverse cholesterol transport (26). Since our study showed reduced phospholipid transfer to the HDL fraction, it is possible that HDL in SCH may be deficient in promoting removal of cholesterol from peripheral tissues, with possible atherogenic consequences. The consequences of reduced triglyceride transfer to HDL are less prone to be predicted in the light of the current data from the literature. The evidence that these findings are associated with hormonal deficiency in patients with SCH was reinforced by reversal of these abnormalities after LT4 treatment and achievement of euthyroidism.
In our study, the average size of the HDL particles was similar in the SCH and control groups, indicating that the reduced transfer of triglycerides and phospholipids to HDL did not reflect on the size of the particles. It is noteworthy that these lipid transfers are bidirectional, and the lipid transfer from HDL to the other lipoprotein classes that are also determinant of lipoprotein size was not evaluated and could also be reduced, compensating for the reduced transfer of lipids to HDL. Similar to findings reported by Kebapcilar et al. (27), the activity of PON1, an antioxidant enzyme associated with HDL, was not compromised in patients with SCH compared with controls and was also unchanged by LT4 treatment. As seen in other studies, levels of PON1 activity varied widely in our patients.
In summary, the metabolism of triglyceride-rich lipoproteins was not affected in patients with SCH. Regarding HDL metabolic aspects, although the size of the lipoprotein and the associated antioxidant PON1 were unchanged, there were disturbances in lipid transfer to the lipoprotein in SCH that were corrected by LT4 treatment and achievement of euthyroidism. Due to the important functions of HDL in cholesterol homeostasis which are dependent on lipid transfers, our results suggest that LT4 replacement in patients with SCH may favor the antiatherogenic properties of the lipoprotein.
Footnotes
Acknowledgments
This study was supported by Fundação do Amparo à Pesquisa do Estado de São Paulo (FAPESP, São Paulo, Brazil, Grant 06/58917-3). Dr. Maranhão is a Research Awardee from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (Brasilia, Brazil). The authors are thankful to Dr. Angela M. Fonseca for her support in patient enrollment.
Disclosure Statement
The authors declare that no competing financial interests exist.