
Abstract
Background:
The cardiovascular effects of transitions from exogenous subclinical hyperthyroidism to short-term overt hypothyroidism in patients treated for differentiated thyroid carcinoma remain unclear. The present study aims at evaluating the changes in multidirectional myocardial strain using two-dimensional (2D) speckle tracking during this controlled transition from exogenous subclinical hyperthyroidism to overt hypothyroidism.
Methods:
The study included 14 patients with differentiated thyroid carcinoma on thyrotropin suppressive thyroxine substitution who were subsequently withdrawn from thyroxine for 4 weeks. Cardiac function was assessed by 2D speckle tracking echocardiography before and 1 and 4 weeks after withdrawal and compared with values obtained in a control group of 24 individuals.
Results:
At baseline, the left ventricular dimensions were significantly higher in patients as compared with controls. Using 2D speckle tracking imaging, the patients had significantly impaired baseline myocardial systolic function in the circumferential (−16.0% ± 2.1% vs. −19.2% ± 3.0%, p = 0.001) and longitudinal (−17.1% ± 2.5% vs. −19.7% ± 3.0%, p = 0.001) directions as compared with controls. Withdrawal of thyroid hormone did not induce significant changes in left ventricular dimensions or systolic function. During the transition from exogenous subclinical hyperthyroidism to overt hypothyroidism, a significant improvement in circumferential and longitudinal systolic shortening was observed and returned to abnormal values when the patients were overt hypothyroid (circumferential strain: from −16.0% ± 2.1% to −18.6% ± 1.9% and −14.7% ± 2.8%, p < 0.005; longitudinal strain: from −17.1% ± 2.5% to −18.8% ± 1.4% and −16.3% ± 1.3%, p < 0.005).
Conclusions:
A U-shaped relationship between a range of thyroid hormone levels (from hyper- to hypothyroid concentrations) and myocardial strains was observed. The clinical consequences of these findings remain to be determined but may point out an increased myocardial vulnerability even in states of moderate subclinical hyperthyroidism and short-term hypothyroidism.
Introduction
Currently, two-dimensional (2D) speckle tracking echocardiography permits the multidirectional evaluation of the mechanical properties of the myocardial tissue (16 –18). Importantly, active myocardial deformation can be evaluated by providing information on myocardial contractility. Therefore, this novel technique may permit the detection of subtle effects of thyroid hormone at the myocardial level. Accordingly, we re-analyzed data from the aforementioned study (13), to comprehensively evaluate LV performance in relation to a wide spectrum of plasma thyroid hormone levels in patients with DTC in transition from subclinical hyperthyroidism, through euthyroidism to hypothyroidism, and to detect changes in LV function using 2D speckle tracking echocardiography.
Methods
Patient population and study design
The patient population consisted of 14 patients in whom DTC was diagnosed and who were subsequently treated with total thyroidectomy and radioiodine ablative therapy. The patient characteristics and the study design have been previously reported (13). In brief, after ablative therapy, the patients received TSH-suppressive thyroxine replacement therapy, aiming at TSH levels <0.1 mU/L (normal reference values 0.4–4.4 mU/L). The patients were scheduled for TSH stimulated diagnostic studies (including thyroglobulin measurements and iodine-131 whole-body scanning to evaluate the effect of earlier radioiodine therapy). Patients were routinely withdrawn from thyroxine therapy for approximately 28 days. On the last day of thyroxine therapy (visit 1) and at days 7 (visit 2) and 28 (visit 3) after thyroid hormone withdrawal, biochemical and hormonal parameters were evaluated; and 2D transthoracic echocardiography was performed. The changes in biochemical, hormonal, and conventional echocardiographic parameters have been previously reported (13). Additionally, LV strain was evaluated with 2D speckle tracking imaging in order to characterize the mechanical properties of the myocardial tissue. As previously described, none of the patients had previous myocardial infarction, rheumatic fever, endocarditis, diabetes mellitus, or connective tissue disorders (13). In addition, the patients were hemodynamically stable during the study period; and any treatment that could influence cardiovascular parameters was not used.
The study was approved by the local ethics committee, and written informed consent was obtained from all patients.
Finally, 24 individuals matched by age, gender, body surface area, and LV ejection fraction (LVEF) were included in the present study and formed the control group. All controls were clinically referred to evaluate atypical complaints and rule out structural heart disease. Individuals referred for echocardiographic evaluation of known valvular heart disease, murmur, congestive heart failure, and cardiac transplantation were excluded. In addition, those individuals with any cardiovascular co-morbidity were excluded. Therefore, the controls had normal echocardiographic studies and provided the normal reference values for the evaluated echocardiographic parameters (19).
Echocardiography
Echocardiography was performed with the patients in the left lateral decubitus position and using a commercially available system equipped with a 3.5-MHz transducer (Vingmed Vivid-7; General Electric Vingmed, Horten, Norway). Standard M-mode, 2D, and color-Doppler data were acquired, triggered to the QRS complex, and saved in cine-loop format for off-line analysis (EchoPac 108.1.5; General Electric/Vingmed Ultrasound). From the M-mode recordings obtained at the parasternal long-axis views, LV dimensions (end-diastolic and end-systolic diameters, end-diastolic interventricular septum thickness, and posterior wall thickness), fractional shortening, and LVEF were measured, according to current guidelines (19). LV mass was calculated by Devereux's formula and indexed to body surface area (20).
2D speckle tracking echocardiography analysis
2D speckle tracking echocardiography permits the angle-independent, multidirectional assessment of LV myocardial strain and strain rate (16). As previously described, the left ventricle deforms in three orthogonal directions (radial, circumferential, and longitudinal) (16). Strain imaging characterizes the LV tissue mechanical properties and differentiate the active myocardial contraction from the passive motion. Strain is a measure of myocardial deformation and is expressed as percentage (%).
From the LV mid-ventricular short-axis images, radial and circumferential strains are assessed. Radial strain measures the thickening/thinning of the myocardial wall, whereas circumferential strain measures the myocardial shortening/lengthening along the curvature of the LV. The average of the six segmental peak systolic strain values provides the global values of radial and circumferential strain (Fig. 1A, B).

Two-dimensional speckle tracking analysis. Radial
Longitudinal strain is measured at the apical 2-, 4-chamber, and long-axis views. Longitudinal strain evaluates the shortening/lengthening of the myocardial wall, resulting from the movement of the mitral annulus plane upward/downward the LV apex. The average of the 18 segmental peak systolic strain values provides the global longitudinal strain value (Fig. 1C) (17).
Therefore, in the present study, LV mechanical properties were evaluated through three systolic parameters (global radial, circumferential, and longitudinal strains), all of them derived with 2D speckle tracking strain imaging.
Statistical analysis
Continuous data are presented as mean ± standard deviation, whereas categorical data are presented as number and frequencies. Baseline echocardiographic characteristics were compared between the patients and the controls using Kruskal-Wallis test. A p-value <0.05 was considered statistically significant. Changes in clinical and echocardiographic parameters within the three different time points (baseline [visit 1], 7 days [visit 2] and 28 days [visit 3]) were compared with the Friedman test and to adjust for inflation of the type I error with multiple tests, a posthoc correction was applied; consequently, a p-value <0.017 was considered significant (0.05 divided by three different stages). All statistical analyses were performed with SPSS software (version 16.0; SPSS, Chicago, IL).
Results
Patient characteristics
This study included 14 patients with DTC (3 men and 11 women), age 51.6 ± 14.5 years, without distant metastases. Median time of TSH suppressive levothyroxine therapy was 1 year. L-thyroxine dose before the withdrawal was 162.5 ±41.6 μg/day. As previously described, at visit 1, serum-free thyroxine concentrations were above the upper limit of the normal range (reference range 10–24 pmol/L); TSH (reference range 0.4–4.8 mU/L) levels were below normal range; and triiodothyronine (reference range 1.1–3.6 nmol/L) levels were within normal range (13). After 7 days of thyroxine withdrawal, free thyroxine levels were already slightly below the lower limit of the reference values, and TSH levels had increased significantly, whereas triiodothyronine levels were still within normal range. During the transition period from hyper- to hypothyroidism, the patients showed a significant increase in body mass index and the diastolic blood pressure (Table 1).
p < 0.017 compared with visit 1.
p < 0.017 compared with visit 2.
p ≤ 0.05 compared with controls.
NA, not available; 2D, two-dimensional; IVST, interventricular septum thickness; LV, left ventricular; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; LVFS, left ventricular fractional shortening; PWT, posterior wall thickness; ref, reference ranges used in the Leiden University Medical Center.
The control group included 24 individuals (45.4 ± 8.5 years, 3 men). By design, there were no differences between controls and patients for age, gender, and body surface area. In addition, there were no significant differences in systolic and diastolic blood pressure and heart rate between healthy controls and patients (Table 1).
LV dimensions and function as assessed with conventional echocardiographic parameters
As previously reported, at baseline the LV dimensions were significantly higher in patients in comparison to controls (Table 1). However, none of the patients met the criteria for LV hypertrophy (13). As previously reported, the acute withdrawal of thyroid hormone (visit 2) did not induce significant changes in LV dimensions or systolic function (Table 1). In addition, these conventional echocardiographic parameters remained unchanged after 28 days (visit 3) of thyroid hormone withdrawal (Table 1).
Changes in LV myocardial tissue mechanical properties as assessed with 2D speckle tracking echocardiography
At baseline, the evaluation of the myocardial tissue properties with 2D speckle tracking imaging demonstrated that the group of patients had significantly impaired myocardial systolic function in the circumferential and longitudinal directions as compared with the group of controls (Table 1). In contrast, radial strain was preserved.
Remarkably, after short-term withdrawal of thyroid hormone, when the patients had the hormone levels within the euthyroid range (visit 2), a significant improvement in circumferential and longitudinal systolic shortening was observed (Fig. 2). However, after 28 days of thyroid hormone withdrawal, when the patients were in an overt hypothyroid state (visit 3), circumferential and longitudinal strains were significantly impaired (Fig. 2). Radial strain values remained unchanged during the study, as they reflect the mid-wall myocardial layer, which is only affected at late stages of cardiac dyfunction. Therefore, 2D speckle tracking permitted the detection of subtle changes in myocardial tissue mechanical properties during the acute induction of hypothyroidism.
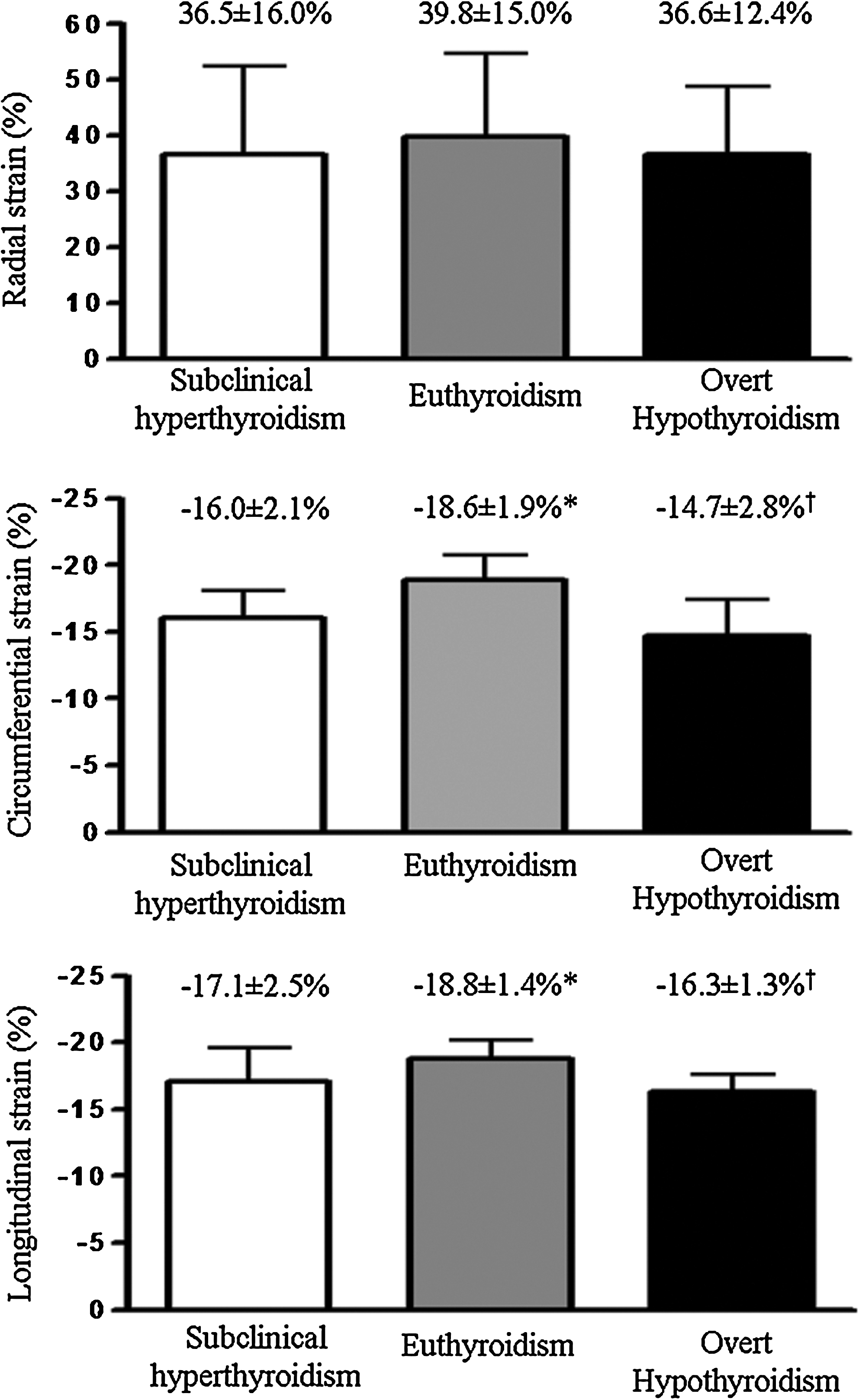
Changes in multidirectional LV myocardial functions during thyroid hormone withdrawal. Baseline values of LV multidirectional strain are presented for patients at baseline (visit 1), 7 (visit 2), and 28 (visit 3) days after thyroid hormone withdrawal. After 7 days of thyroid hormone withdrawal (visit 2, euthyroid to hypothyroid status), a significant improvement was observed in circumferential and longitudinal strains. However, after 28 days of thyroid hormone withdrawal (visit 3, overt hypothyroidism), circumferential and longitudinal strains were significantly impaired. Radial strain remained unchanged during the follow-up. *p < 0.017 versus visit 1; † p < 0.017 versus visit 2.
Discussion
The current study evaluated subtle changes in LV function using 2D speckle tracking echocardiography in relation to a wide spectrum of plasma thyroid hormone levels in patients with DTC in transition from exogenous subclinical hyperthyroidism via euthyroidism to overt hypothyroidism. Exogenous subclinical hyperthyroid status was associated with impaired myocardial deformation in the circumferential and longitudinal directions. Restoration of euthyroidism induced an improvement in myocardial deformation in these two directions, whereas overt hypothyroidism was accompanied by impairment in myocardial deformation properties. In contrast, radial strain was preserved along the follow-up. As previously described (21), the LV myocardial architecture is a complex array of longitudinally and circumferentially orientated fibers located at the subepi/subendocardium and mid-wall, respectively. The subendocardial fibers are more vulnerable to ischemia, hemodynamic overload, or age-related changes and, therefore, longitudinal strain is commonly impaired at an early stage of the disease. In contrast, radial strain, derived from mid-wall fibers, is preserved.
Patients with DTC, who until recently were substituted with TSH suppressing dosages of levothyroxine and routinely withdrawn from thyroid hormone substitution for diagnostic studies, offer an attractive group to perform this type of studies. Particularly, the design of the present study permitted us to evaluate subtle changes in LV myocardial performance, thus providing a reliable and sensitive evaluation of the effects of thyroid hormone at the myocardial level. Earlier studies have been performed using conventional echocardiographic strategies, which may not be sensitive enough to detect subtle abnormalities at the myocardial level. Indeed, in those studies, no clear conclusions on the cardiac consequences of acute hypothyroidism in patients with exogenous subclinical hyperthyroidism were reached (7 –15). None of those studies focused on the direct effect of thyroid hormone on myocardial contractility and deformation. 2D speckle tracking strain imaging enables assessment of systolic and diastolic myocardial deformation properties in the three orthogonal spatial directions. Unlike tissue Doppler imaging, 2D speckle tracking imaging provides angle-independent measurements of myocardial strain. Although conventional echocardiography did not show any significant changes, 2D speckle tracking strain imaging showed remarkable results, with significantly decreased circumferential and longitudinal strain as compared with controls during subclinical hyperthyroidism, a significant improvement during euthyroidism, and a significant deterioration again during profound hypothyroidism. Therefore, a remarkable U-shaped relationship between thyroid hormone concentrations and myocardial strain was observed, with hyper- and hypothyroidism equally affecting myocardial mechanical properties. As such, this study demonstrates the myocardial effects of a wide spectrum of thyroid hormone levels independently of LV mass. Indeed, it has been previously demonstrated that thyroid hormone exerts direct effects on myocardial diastolic relaxation independent of protein synthesis and cardiac growth (5,22). Therefore, the changes observed in myocardial strain may reflect the direct biochemical effects of thyroid hormone on the myocardium that lead to activation of local signal transduction pathways rather than changes in LV hypertrophy (23). In addition, changes in hemodynamic conditions that take place during transition from exogenous subclinical hyperthyroidism to euthyroidism and overt hypothyroidism may also influence myocardial strain (24). Whether these changes in multidirectional myocardial strain influence the TSH suppressive treatment and, subsequently, the long-term outcome remain unknown. Additional studies are needed to elucidate the effects on long-term outcome of a tailored TSH suppressing therapy based on 2D speckle tracking strain imaging.
Some study limitations should be acknowledged. Circulating levels of TSH and free thyroxine were not systematically determined in all controls. Therefore, the controls were considered euthyroid based on clinical history and complete physical examination.
In conclusion, this study demonstrates the subtle effects of profound short-term changes of thyroid hormone levels on the myocardium, likely reflecting direct biochemical effects of thyroid hormone on myocardial metabolism, rather than structural changes. A U-shaped relationship between the spectrum of thyroid hormone levels from hyper- to hypothyroid concentrations and myocardial strain is observed. The clinical consequences of these findings remain to be determined, but they may point to an increased myocardial vulnerability even in states of moderate subclinical hyperthyroidism and short-term hypothyroidism.
Disclosure Statement
J.J.B. receives grants from Biotronik, Medtronic, Boston Scientific, BMS medical imaging, St. Jude Medical, Edwards Lifesciences, and GE Healthcare. The remaining authors have no conflicts of interest to disclose.