
Abstract
Background:
The diffuse sclerosing variant of papillary thyroid carcinoma (DSPC) is a relatively rare variant of papillary thyroid cancer. Large studies of patients with DSPC have been infrequently performed, and controversy still exists concerning some DSPC features and outcomes. The aim of the present study was to retrospectively evaluate the clinicopathologic features and outcomes in a series of 34 consecutive patients with DSPC and to compare them with a larger group of 245 consecutive patients with the classic variant of papillary thyroid carcinoma (cPTC) that were evaluated in the same period.
Patients and Methods:
Clinical and histological features (sex, age, tumor size, multifocality, bilaterality, extrathyroid extension, and local and distant metastases) were recorded in all patients, as well as any persistent or recurrent disease and the patients' disease status at last observation. Patients with cPTC were classified as either low (122) or high risk (123). DSPC and high-risk patients were all treated with the same protocol, including 131I treatment. All patients were included in a Cox regression model analysis to investigate the effect of each variable on the hazard ratio.
Results:
As expected, multifocality, bilaterality, and extrathyroid extension were more frequently noted at presentation, and the pT1 category of TNM classification was less frequently noted in DSPC and high-risk patients with cPTC compared with low-risk patients with cPTC. No significant difference was found between patients with DSPC and those with high-risk cPTC, except that extrathyroid extension was found more frequently in the patients with DSPC. Using multivariate analysis, diffuse sclerosing variant was an independent variable for predicting a high risk of persistent and recurrent disease during initial follow-up. However, at a later time, and after further treatment, the disease status was not different between patients with DSPC and those with high-risk cPTC, and only the presence of distant metastases affected the final outcome.
Conclusions:
DSPC is a thyroid papillary carcinoma variant characterized by high aggressiveness. In patients with DSPC, the outcome is worse than in patients with low-risk cPTC; and, at presentation, characteristics are somewhat worse than for patients with high-risk cPTC. At medium term, the outcome is similar to that observed in patients with high-risk cPTC, provided aggressive treatment is used (additional surgical intervention, when required, and/or 131I radiotherapy).
Introduction
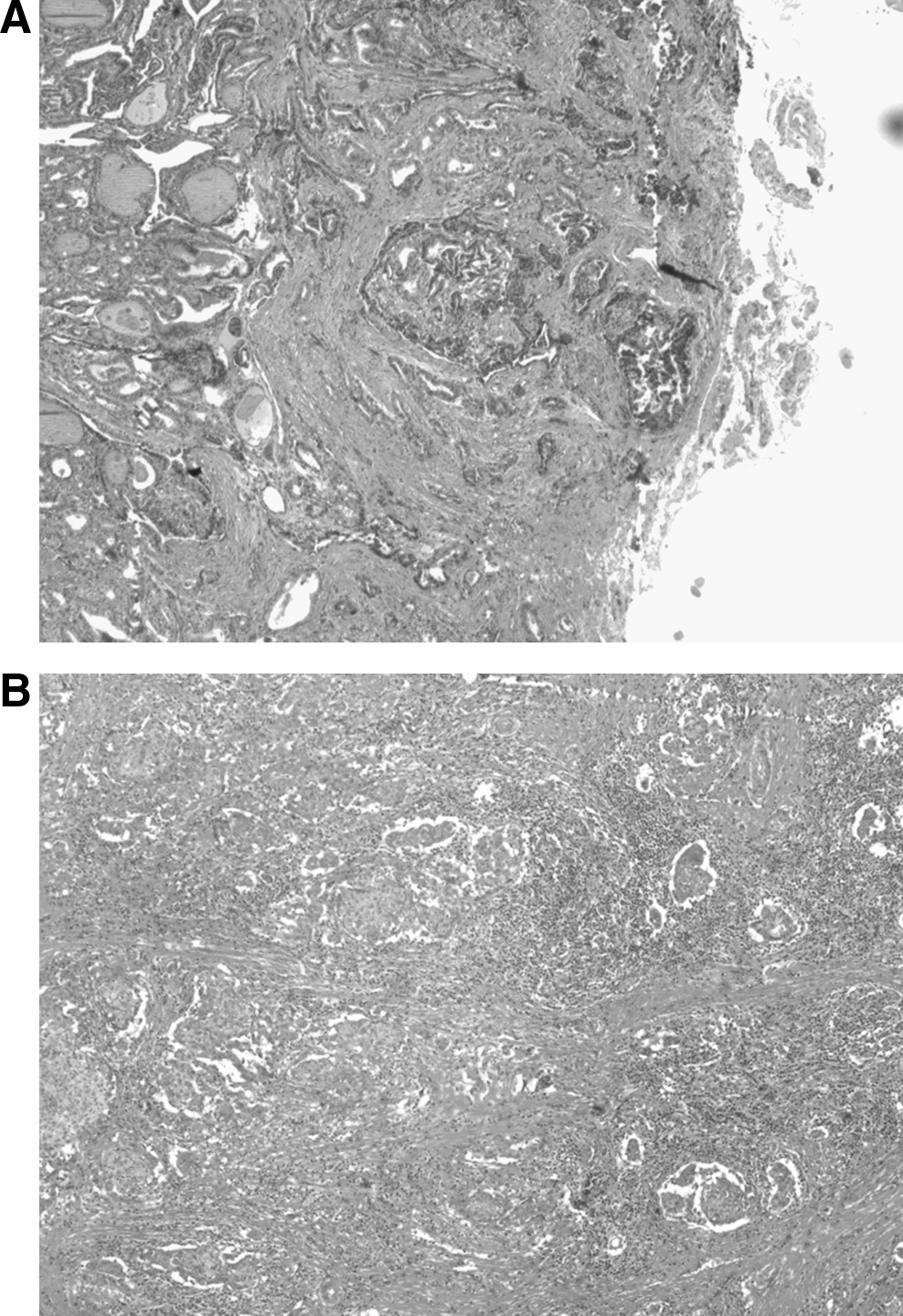
The diffuse sclerosing variant of PTC (DSPC) was first described in 1985 (3) and is characterized by extensive (frequently bilateral) lymph-vascular invasion, prominent squamous metaplasia, numerous psammoma bodies, and dense sclerosis in a background of lymphocytic thyroiditis. This cancer was recognized as one histological variant of PTC in 1988 (4) and is classified by a less favorable prognosis among the PTC variants (4). DSPC is an uncommon pathologic entity, and its prevalence among patients with PTC ranges from 0.7% to 5.3% (5 –13), except in the case of one study that indicated a 20.9% prevalence (8). Approximately 250 cases have been described, and there have been no studies representing more than 35 patients, except for Falvo et al. (8), who described 83 cases in a 9-year period. The diffuse thyroid gland involvement can mimic chronic thyroiditis in ultrasound scans, presenting an atypical pattern showing diffuse scattered microcalcifications (“snowstorm appearance”) (14). Figure 1 shows an example of diffuse sclerosing variant of papillary thyroid carcinoma (Fig. 1A) and classical papillary thyroid carcinoma, with signs of sclerosis (Fig. 1B).
Due to the limited number of cases and the heterogeneity of the tumor's clinical behavior, there is no consensus for DSPC's optimal treatment and post-operative follow-up. This is also due to the fact that different studies have shown controversial findings regarding DSPC's prognosis and outcome. Some studies report a high incidence of lymph node involvement and lung metastases, resulting in a less favorable prognosis (6,8,10,12); others observe that DSPC's prognosis is not different from that of classic papillary carcinoma (5,7,9,11,13).
To address these questions, we carried out a retrospective study on 34 consecutive patients with DSPC who were referred to our thyroid clinic. We compared the outcomes of patients with this cancer to those of a group of 245 patients with papillary thyroid cancer (classical variant) who were examined during the same time period. Considering the heterogeneity of thyroid papillary cancer and many tumors showing a small size (microcarcinomas), limited diffusion, and indolent evolution, the PTC comparison group was selected as a continuous series of patients with either low-risk or high-risk classic variant of PTC (cPTC). This choice was also made to avoid possible bias due to different follow-up procedures.
Patients and Methods
We retrospectively reviewed 34 consecutive patients in whom DSPC was first observed between 1999 and 2009. All patients are presently in active follow-up at our thyroid clinic in the Division of Endocrinology (University of Catania, Italy). Patients underwent total thyroidectomy with central-compartment lymph node dissection and latero-cervical lymph node dissection only when this involvement was documented by pre-surgery ultrasound examination. All histological specimens were analyzed by the same expert pathologist, and, according to WHO classification criteria (2), the samples were evaluated for the presence of numerous psammoma bodies, squamous metaplasia, and marked and diffused sclerosis. These criteria were used to distinguish DSPC from sclerotic PTC, which is associated with sclerosis but not to the same degree as DSPC. Cases classified as “sclerotic” papillary carcinoma during the pathology examination were excluded, because this indicated fibrosis rather than the specific sclerosing PTC variant.
Data recorded for each patient included the following: age, gender, information regarding the surgical treatment, tumor localization and size (greatest diameter), TNM stage (15), and follow-up for TNM staging. The extent of the primary tumor (T) and the regional lymph node metastases (N) were determined on the basis of pathological data, and the evidence of distant metastases (M) was based on the findings of the first postsurgical 131I whole body scan. After surgery, all patients with DSPC were considered high-risk and treated with 131I (1110–3700 MBq) after L-thyroxine withdrawal (serum TSH level >30 mU/L). Follow-up was based on serum thyroglobulin (Tg) and antithyroglobulin antibody (ATA) measurements and neck ultrasonography. Persistent or recurrent disease was diagnosed when the following were present: Tg levels >1.0 ng/mL under suppressive L-thyroxine therapy; Tg levels >2.0 ng/mL after recombinant human TSH (rhTSH) stimulation; or Tg levels >5.0 ng/mL after L-thyroxine withdrawal. This disease was also diagnosed with or without the previous criteria and when the whole body scan was positive, or when suspicious lymph nodes were present and, at fine needle biopsy, were proved positive for Tg measurement in washout specimens. Tg and antithyroglobulin antibody were measured by immunoradiometric assays using commercial kits.
Disease-free interval (DFI) is the time (months) between the diagnosis date and the last observation where there is absence of persistent or recurrent disease. In patients with persistent or recurrent disease, other imaging procedures (computed tomography, magnetic resonance imaging, and bone scan), in addition to other treatments (radioiodine or surgery, as appropriate), were performed when required.
Data from patients with DSPC were compared with those obtained from 245 consecutive patients in whom cPTC was diagnosed during the same period. These patients were classified as low- (122 patients) or high-risk (123 patients), and they were monitored in the same thyroid clinic. High-risk patients with cPTC had at least one of the following characteristics: tumor size ≥4 cm, advanced grading (G2–G4), bilaterality, extrathyroid extension, or locoregional or distant metastases. Patients with DSPC and high-risk cPTC were treated with similar procedures including 131I postsurgical treatment (1110–3700 MBq).
Data from our patients with DSPC were also compared with those obtained in a Medline search (years 1989–2009) for cases specifically reported as DSPC.
Statistical analysis
Quantitative data are depicted as mean and standard deviation, and numbers and percentages are presented for qualitative data. Continuous variables were compared using the t-test, whereas the Chi-squared test was used for percentages. The mean DFI and 95% confidence interval (CI) were calculated using the Kaplan–Meier method, and the Logrank test was used for comparing DFI between two groups. The impact of clinical and histopathological data on the risk of either persistent or recurrent disease after surgery or persistent disease at the time of the last visit was analyzed through the logistic regression model. The results were reported with an odds ratio (OR) and a 95% CI. All tests were two-sided, and a p-value <0.05 was considered statistically significant.
Results
Clinical data at presentation
Before surgery, all but two patients with DSPC had a uninodular or multinodular goiter and were euthyroid. Of these two patients, one showed a normal thyroid volume, no thyroid nodule, and severe hypothyroidism (16), and the second patient had subclinical hypothyroidism. A high number of women were observed in both groups (7.5/1 in patients with DSPC and 4.1/1 in patients with cPTC).
Total thyroidectomy, together with central neck lymph-node dissection (pretracheal, paratracheal, and prelaryngeal), was carried out in 18 out of the 34 patients with DSPC. In six out of the 18 patients, lateral-cervical lymph nodes were also dissected, because pre-operative neck ultrasonography was suspicious, or because central nodes were extensively invaded. The remaining 16 patients with DSPC underwent total thyroidectomy without lymph-node dissection.
Although the average tumor diameter was similar in the patients with DSPC and cPTC, the prevalence of multifocality, bilaterality, and extrathyroid extension was higher in the patients with DSPC and high-risk cPTC compared with the patients with low-risk cPTC (p < 0.0001) (Table 1). Differences between patients with DSPC and those with high-risk cPTC were statistically significant only for the prevalence of extrathyroid extension (61.8% and 40.7%, respectively) (p < 0.05). There was no significant difference between patients with DSPC and those with high-risk cPTC based on the prevalence of TNM categories; at presentation; however, in both groups, the TNM pT1 category was less frequent than in the patients with low-risk cPTC (Table 2).
p < 0.001 versus low-risk cPTC.
p < 0.0001 versus low-risk cPTC.
p < 0.05 versus high-risk cPTC.
DSPC, diffuse sclerosing variant of papillary thyroid carcinoma; cPTC, classic papillary thyroid cancer.
p < 0.0001 versus low-risk cPTC.
Post-operative follow-up
The median follow-up was 50 months (range 12–127 months) in patients with DSPC and 69 months (range 32–93 months) in patients with cPTC. At the first post-surgery follow-up, persistent or recurrent disease was detected in 15 (44.1%) of the patients with DSPC and 29 (23.6%) of the patients with high-risk cPTC (p < 0.05). Of the 15 patients with DSPC, one had distant metastases (lymph-node metastases in the middle-lower mediastinum), seven had neck lymph-node involvement, and the remaining seven patients had elevated Tg levels after either L-T4 treatment withdrawal or rhTSH stimulation (range 2.1–32.5 ng/mL), indicating persistent disease. Among the 29 patients with cPTC, five had distant metastases, five had neck lymph-node involvement, and the remaining 19 had detectable Tg levels (range 2.2–21.7 ng/mL) after either L-T4 treatment withdrawal or rhTSH stimulation without identified disease localization.
Univariate regression analysis showed a significant impact of both lymph-node metastases (OR = 1.91; 95% CI = 1.05–3.46) and DSPC histology (OR = 2.65; 95% CI = 1.41–4.96; p < 0.05 for both) on predicting a high risk for persistent or recurrent disease after initial surgery and postoperative 131I treatment. Multivariate analysis confirmed only the DSPC histological variant as an independent variable (OR = 2.46; 95% CI = 1.31–4.64; p = 0.005) (Table 3). DFI was significantly influenced by both the presence of lymph-node involvement and the DSPC variant. The mean DFI was 62.9 months (95% CI = 52.9–72.8) when lymph-node involvement was present and 95.6 months (95% CI = 82.2–108.9) when it was absent (p < 0.05). Moreover, the mean DFI was 59.3 months (95% CI = 37.6–81.1) in patients with DSPC and 69.5 months (95% CI = 63.7–75.3) in patients with high-risk cPTC (p < 0.005).
OR, odds ratio; CI, confidence interval.
At subsequent follow-up, 12 out of the 15 patients with DSPC with persistent or recurrent disease underwent further treatment (five had lymph-node neck dissections plus 131I therapy, and seven had 131I therapy only), whereas all 29 patients with high-risk cPTC with persistent or recurrent disease underwent further treatment (10 had lymph-node neck dissections plus 131I therapy, 18 had 131I therapy only, and one had external radiotherapy).
Disease status at the last observation
At the last visit, 33 patients with DSPC were alive, and one male patient had died from a myocardial infarction. Among these patients, seven (21.2%) had persistent or recurrent disease, as documented by detectable Tg levels after either L-T4 treatment withdrawal or rhTSH stimulation (range 2.2–23.0 ng/mL), but only one of them had tumor tissue identified (distant lymph-node metastases in the mediastinum).
All of the 123 patients with high-risk cPTC were alive at the last visit; twenty-four patients (19.5%) had persistent or recurrent disease, however (p = 0.15 vs. DSPC), with detectable Tg levels. Of these latter, five patients had lung metastases, one had lung and bone metastases, four had neck lymph-node involvement, and fourteen had only detectable Tg levels (range 2.1–53.4 ng/mL) after either LT4 treatment withdrawal or rhTSH stimulation.
Using both univariate and multivariate analyses at the end of our observation period, a high risk of persistent disease was significantly predicted only by the presence of distant metastases (OR = 13.9; 95% CI = 5.4–35.5 using univariate, and OR = 12.3, 95% CI = 4.8–31.5 using multivariate analyses) (p < 0.0001) (Table 4). The mean DFI was 49.7 months (95% CI = 33.8–65.7) for patients with distant metastases and 101.1 months (95% CI = 90.9–111.3) for patients without distant metastases (p < 0.0001). In these 156 total patients, the mean DFI was shorter in men (76.4 months, 95% CI = 69.5–83.2) than in women (100.8 months, 95% CI = 90.4–111.3; p = 0.059), a difference that was nearly significant using multivariate regression analysis (OR = 2.12; 95% CI = 0.91–4.74; p = 0.07).
Review of the literature
Table 5 summarizes the data from 10 studies (243 patients with the DSPC). Only studies reporting more than five cases are included. Data from different studies appear somewhat heterogeneous, probably due to slight differences in diagnostic and therapeutic procedures. It is noteworthy that in our large DSPC study, the age at diagnosis was older than in previous studies but not younger than in patients with cPTC (5 –13). Additionally, the female-to-male ratio in our study was higher than in most of the previous studies.
AWD, alive with disease.
Discussion
PTC represents 80%–90% of primary thyroid malignancies, and it occurs more frequently in middle age (among the fifth and sixth decades of life) with a female-to-male ratio of about 3–4:1 (1). Tumors are often multifocal and bilateral (about 40%). About 25% of these patients have recurrent disease, and 8% die from this type of cancer, even if their survival after diagnosis is long in the great majority of cases, despite the prediction of unfavorable outcome. Cervical lymph-node involvement is associated with increased recurrences but not with increased deaths. Extrathyroid invasion carries an increased risk of death (5–6-fold), and distant metastases increase this risk by 47-fold (17).
In 1988, Hedinger and other pathologists at the WHO Collaborating Center for the Histological Classification of Thyroid Tumors (4) defined DSPC as a histological variant of PTC and suggested that it has a less favorable prognosis than papillary carcinoma as a whole. Different studies in small series (5 –13) and case reports (18 –28) have shown controversial findings about the initial presentation, recurrence, and prognosis of DSPC. These studies conclude that either the prognosis does not differ from that of conventional classic papillary carcinoma or that DSPC is more aggressive, with a higher incidence of locoregional and distant metastases.
Patients with DSPC are frequently reported to be younger than patients with cPTC, and Koo et al. observed that the diffuse sclerosing variant is the major subtype of papillary thyroid cancer in the young (29). In most studies, the mean age at presentation ranged from 18 to 35 years for patients with DSPC, which is about 10–20 years younger than patients with cPTC. In our study, the mean age was 43.2 years (range 15–78), similar to that of our cPTC group. We also observed a higher female preponderance than has been previously reported (7.5:1, female-to-male ratio). We have no explanation for these differences.
At clinical presentation, the first sign for most patients with DSPC is a mass lesion in the neck. Approximately 30% of patients with DSPC have positive antithyroid antibodies as part of Hashimoto's thyroiditis (13), but these antibodies rarely interfere with thyroid gland function. The diffuse thyroid involvement can mimic chronic thyroiditis in ultrasound examinations. For this reason, some patients with DSPC can be treated for years for Hashimoto's thyroiditis, which is suggested by diffuse enlargement of one or both thyroid lobes with no clear evidence of nodules, and the presence of antithyroid autoantibodies, thus delaying the diagnosis of thyroid cancer. The key for the correct diagnosis is the detection of widely distributed psammoma bodies. In patients with an atypical ultrasound pattern showing diffuse scattered microcalcifications (“snowstorm appearance”), the possibility of DSPC should always be considered, and fine needle aspiration should be carried out to obtain the diagnosis of DSPC (16,30 –32).
In our study, at the time of presentation, DSPC was associated with unfavorable histological characteristics in most cases (multifocality, bilaterality, extrathyroid extension, the presence of lymph-node metastases, and pT3 or pT4 TNM categories; all typical of high-risk PTC cancers). Also, distant metastases occurred in only one case at presentation and in no cases during follow-up, which is lower than the average incidence reported in DSPC (14.9%, lung and bone being the most frequent sites) (7,33,34). Due to the frequent delay for the correct diagnosis, increased lymph-node metastases, and higher percentages of pT3 and pT4, DSPC has been considered as having a more aggressive behavior and a worse prognosis (6,8,10,12), with a higher disease-specific death rate, compared with that for cPTC (3.6% and 0.6%, respectively) (8). Other studies, however, report 5- and 10-year DSPC survival rates equal to 95% (13) and 93% (11), respectively, similar to those reported for cPTC.
In our study, after total thyroidectomy and 131I treatment, the multivariate analysis indicated that only the diffuse sclerosing histological variant was an independent factor associated with a higher risk of persistent or recurrent disease. However, an aggressive treatment protocol (total thyroidectomy with lymph-node dissection and radioiodine treatment) allowed for a medium-term outcome similar to that of patients with high-risk cPTC in spite of the more unfavorable pathologic features at presentation in patients with DSPC.
The survival rate depends not only on the cancer and host characteristics but also on the treatment. After a median follow-up of 50 months, all of our patients with DSPC were alive (except one who had died due to a myocardial infarction), and only 20% showed signs of persistent or recurrent local disease. Only one patient had distant metastases, and these were already present at diagnosis. These data are similar to those observed in the 123 patients with high-risk cPTC followed and treated with similar procedures. Comparative data from different studies illustrated in Table 5 show heterogeneity among different observations in terms of patient and cancer characteristics and evolution. Differences in diagnostic, therapeutic, and follow-up procedures and in the limited number of cases in some studies may account for these discrepancies.
In conclusion, the prognosis of patients with DSPC is worse than in patients with low-risk cPTC and can be assimilated to that of patients with high-risk cPTC. The frequent, massive neoplastic involvement of the thyroid gland, the high prevalence of lymph-node metastases, and the frequent extrathyroid extension in this type of cancer require aggressive treatment (total thyroidectomy with lymph-node dissection and radioiodine ablation of residual tissue) and strict follow-up to obtain early diagnosis of frequent recurrences. This strategy may reduce the recurrence rate and allow a medium-term outcome to be achieved and is similar to the strategy employed with regard to patients with high-risk cPTC, despite the frequent, unfavorable signs at presentation in these patients with DSPC.
Footnotes
Disclosure Statement
No competing financial interests exist.