
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) is a malignancy with one of the highest fatality rates. Here we report a retrospective study of the treatment and other factors associated with its outcomes.
Materials and Methods:
The medical records of 100 patients diagnosed with ATC at Ito Hospital between 1993 and 2009 were reviewed and pertinent information was extracted and analyzed.
Results:
There were 80 women and 20 men, and their median age at diagnosis was 68 years (range, 41–90 years). Thirteen patients had a history of well-differentiated thyroid carcinoma. Six patients had a small ATC focus within a differentiated carcinoma. All cases were retrospectively staged according to the Union for International Cancer Control classification system, and the results were stage IVA in 11 cases, stage IVB in 31 cases, and stage IVC in 58 cases. Seventy patients underwent surgical treatment, and complete resection was performed in 24 of them. Seventy-eight patients received radiotherapy, and 58 of them received a total dose of ≥40 Gy. Twenty-seven patients received chemotherapy. Only 15 patients received multimodal therapy (surgery, radiotherapy, and chemotherapy). The 1-year survival rates according to stage were as follows: stage IVA, 72.7%; stage IVB, 24.8%; and stage IVC, 8.2%. Multivariate analysis identified age ≥70 years, white blood cell ≥10,000 mm3, extrathyroidal invasion, and distant metastasis at the time of diagnosis as prognostic factors. Survival after complete resection was significantly better than after incomplete resection or no resection. The results also suggested that radiation doses of ≥40 Gy were associated with significantly longer survival.
Conclusion:
Although the prognosis of most patients with ATC continues to be poor, surgery, radiotherapy, and a combination of both improved the survival of patients with ATC.
Introduction
Several recent studies have reported that a number of factors, including age, gender, tumor size, leukocytosis, the presence of acute symptoms, distant metastasis, coexistence of well-differentiated thyroid carcinoma, surgical resection, and multimodal therapy, affect the prognosis of ATC patients (8 –12).
In this retrospective study, we reviewed the medical records of ATC patients treated in our hospital to determine which treatments improved the outcome ATC patients and to select patients who would benefit from such treatment.
Materials and Methods
We reviewed the medical records of 100 patients with ATC diagnosed at Ito Hospital in Tokyo between January 1993 and December 2009. The diagnosis of ATC was based on a combination of the results of the clinical findings and fine-needle aspiration (FNA) biopsy findings. Open biopsy was performed when the FNA biopsy was inadequate in terms of making a diagnosis.
Several treatment protocols consisting of surgery followed by external radiotherapy and/or chemotherapy have been conducted at our institution. Radiation was delivered to the neck or mediastinum, or both, at doses ranging from 40 to 80 Gy. Various chemotherapy protocols were tried: between 1993 and 1995, 4 patients were treated with a combination of cisplatin, adriamycin, etoposide, and peplomycin; between 1996 and 2003, 14 patients were treated with a combination of cisplatin, doxorubicin, and etoposide; and after 2004, 9 patients were treated with a combination of paclitaxel and carboplatin or with paclitaxel alone.
The survival rates were calculated and compared according to several factors. The Kaplan–Meier method was used to calculate the cumulative survival rate of patients from the date of diagnosis to the date of death or the most recent follow-up examination. The impact of various factors on survival was analyzed by means of the log-rank test. Multivariate analyses of prognostic factors were based on the Cox proportional hazards model. A p-value less than 0.05 was considered statistically significant. All data were calculated with computer software (JMP version 8.0; SAS Institute Inc., Cary, NC).
Results
The characteristics of all 100 ATC patients are shown in Table 1. There were 80 women and 20 men, and their median age at diagnosis was 68 years (range, 41–90 years). The most initial manifestations were a mass in the neck (93%), hoarseness (24%), pain (19%), and dyspnea (4%). The diagnosis of ATC was confirmed histopathologically in 91 patients and cytopathologically in 9 patients. Thirteen patients had a history of well-differentiated thyroid carcinoma. Six patients with a small focus of ATC underwent surgery for a preoperative diagnosis of differentiated thyroid carcinoma, and a small focus of ATC was identified as an incidental finding during histological examination of the surgical specimen in all six cases. All cases were retrospectively staged according to the Union for International Cancer Control classification system, and the results were stage IVA in 11 cases, stage IVB in 31 cases, and stage IVC in 58 cases. Seventy patients underwent surgery: total thyroidectomy in 35, subtotal thyroidectomy in 11, lobectomy in 23, and partial lobectomy in 1. In 24 of them the resection was complete (R0), and surgical debulking (R1/R2), which was indicated if reduction of more than 90% of the tumor volume was expected, was performed in the other 46. Nine patients underwent extensive surgery: partial resection of the trachea in 5, partial resection of the esophagus in 5, and a combination of both in 1. Some patients had no surgery because of the extent of extrathyroidal invasion such as that involving the esophagus and the carotid artery. Patients with a preoperative diagnosis of papillary thyroid carcinoma underwent lymph node dissection.
UICC, Union for International Cancer Control; WBC, white blood cell.
Seventy-eight patients received radiotherapy, and in 58 of them the dose was ≥40 Gy. Sixty patients received radiotherapy as postoperative adjuvant therapy, 5 received a combination of radiotherapy and chemotherapy, and 10 received radiotherapy alone. In 20 of the 78 patients, radiotherapy was discontinued because of side effects, including pharyngoesophagitis, tracheitis, and bleeding into the airway. A partial response (PR) was achieved in 10 patients, and 10 patients treated with radiotherapy after a curative operation survived more than 1 year without local recurrence.
Chemotherapy was used to treat 28 patients, 25 of whom received chemotherapy as adjuvant therapy after surgery, and 4 of whom received weekly paclitaxel as neoadjuvant therapy. Only 15 patients were treated with multimodal therapy consisting of surgery, radiotherapy, and chemotherapy. Bone-marrow depression and renal failure developed in 1 patient who had been treated with combination chemotherapy consisting of cisplatin, doxorubicin, and etoposide.
The median overall survival time was 3.9 months (range, 0.06–151.3). The overall 6-month, 1-year, and 2-year survival rates were 40.4%, 21.3%, and 12.3%, respectively. The clinical characteristics and treatments of the 19 patients who survived for more than 1 year after their diagnosis, 7 of whom are alive and free of disease, are shown in Table 2. The 6-month, 1-year, and 2-year survival rates were 100%, 72.7%, and 62.3%, respectively, in the stage IVA cases, 49.6%, 24.8%, and 10.6%, respectively, in the stage IVB cases, and 22.4%, 8.2%, and 0%, respectively, in the stage IVC cases (Fig. 1). The median survival time was 33.5 months in stage IVA, 6.1 months in stage IVB, and 2.5 months in stage IVC. The six patients with an incidentally detected small focus of ATC had a significantly better outcome than the other ATA patients with ordinary ATC (p<0.0001) (data not shown). All of these were alive after more than 1 year and only one of them had died (with lung metastasis at 9 years after their diagnosis). The 6-month, 1-year, and 2-year survival rates were 67.8%, 53.2%, and 42.6%, respectively, after complete resection; similarly they were 44.9%, 16.5%, and 3.9%, respectively, after debulking and 10.9%, 3.6%, and 0%, respectively, after no resection (Fig. 2). The survival rate was significantly higher after complete resection than after incomplete resection (debulking) or no resection (p<0.0001). Further, as shown in Figure 3, the group of patients irradiated with a dose of ≥40 Gy had a higher survival rate than the group irradiated with a dose <40 Gy (p<0.0001). The results of this study showed no statistically significant difference in survival rate between the patients with primary ATC and the patients with anaplastic transformation in metastatic lymph nodes. Death was related to the ATC in 81 patients (to local progression in 21, to distant metastasis in 55, and to both in 3). The relationship of death to ATC was unknown in two patients and it was related to other diseases in three patients.
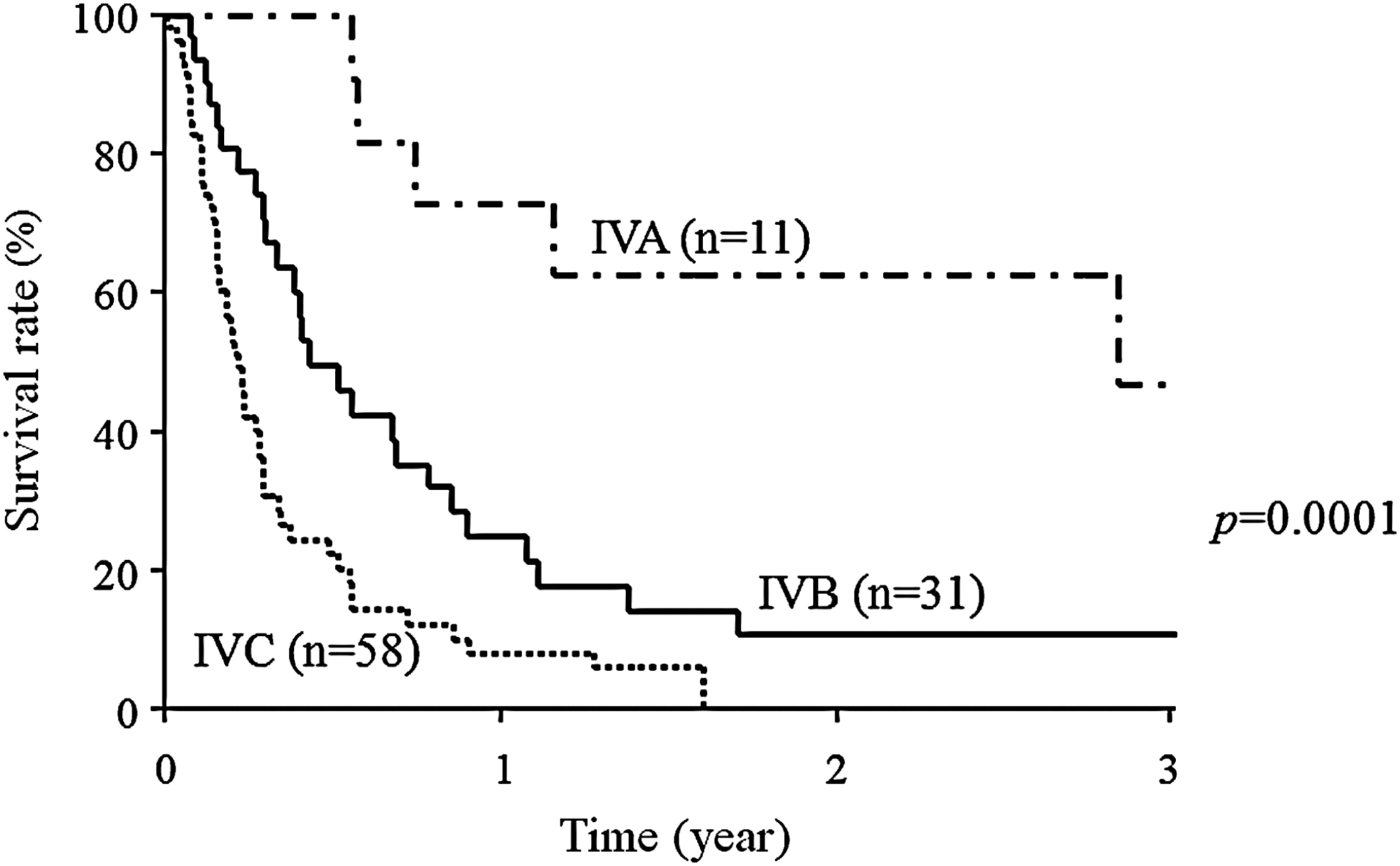
Survival curves of three groups (stages IVA, IVB, and IVC) of cases. There was a significant difference between the groups (p<0.0001, log-rank test).
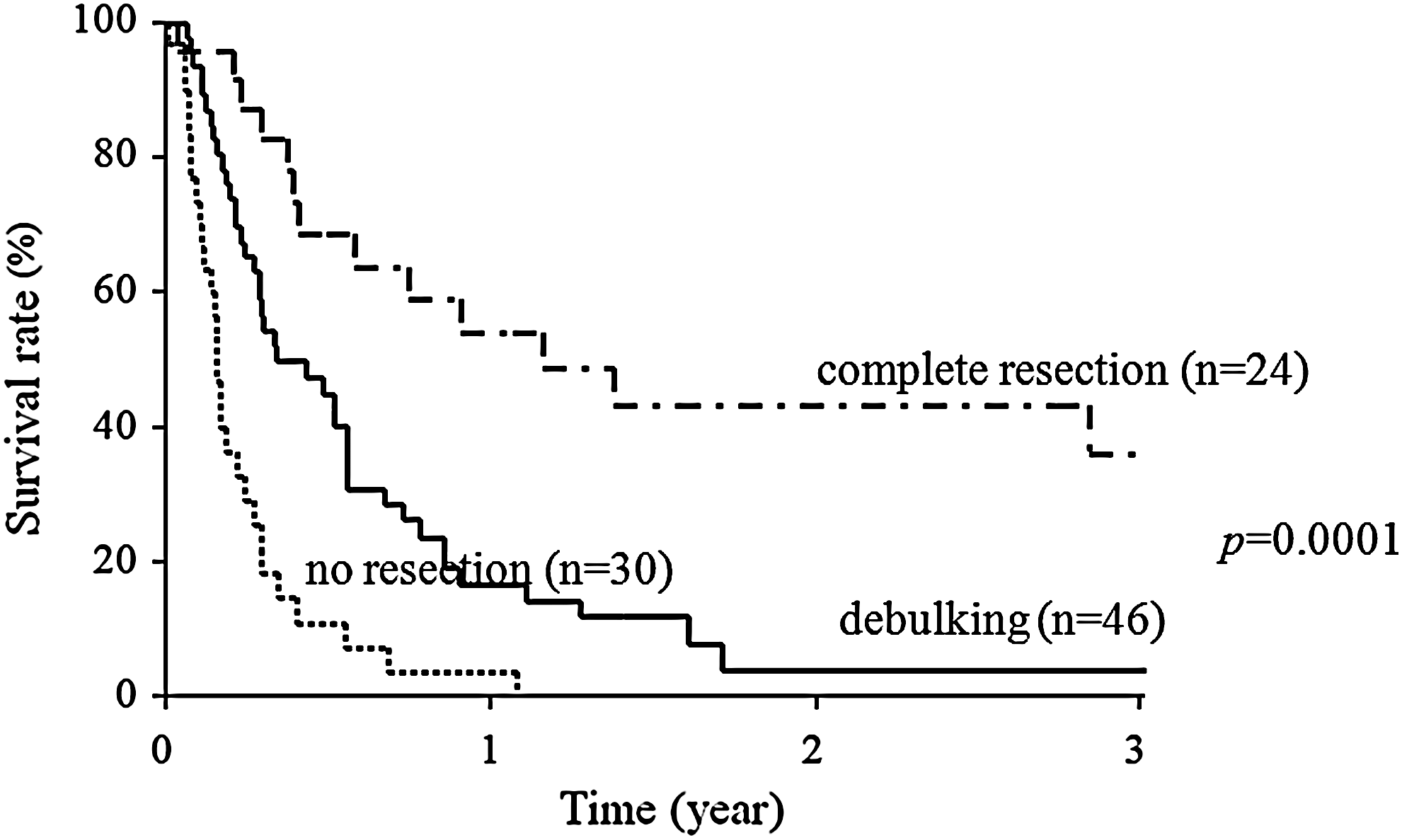
Comparison between the survival rates of patients treated with complete resection, incomplete resection (debulking), or without resection. Survival was significantly better after complete resection than after incomplete resection (debulking) or no resection (p<0.0001, log-rank test).
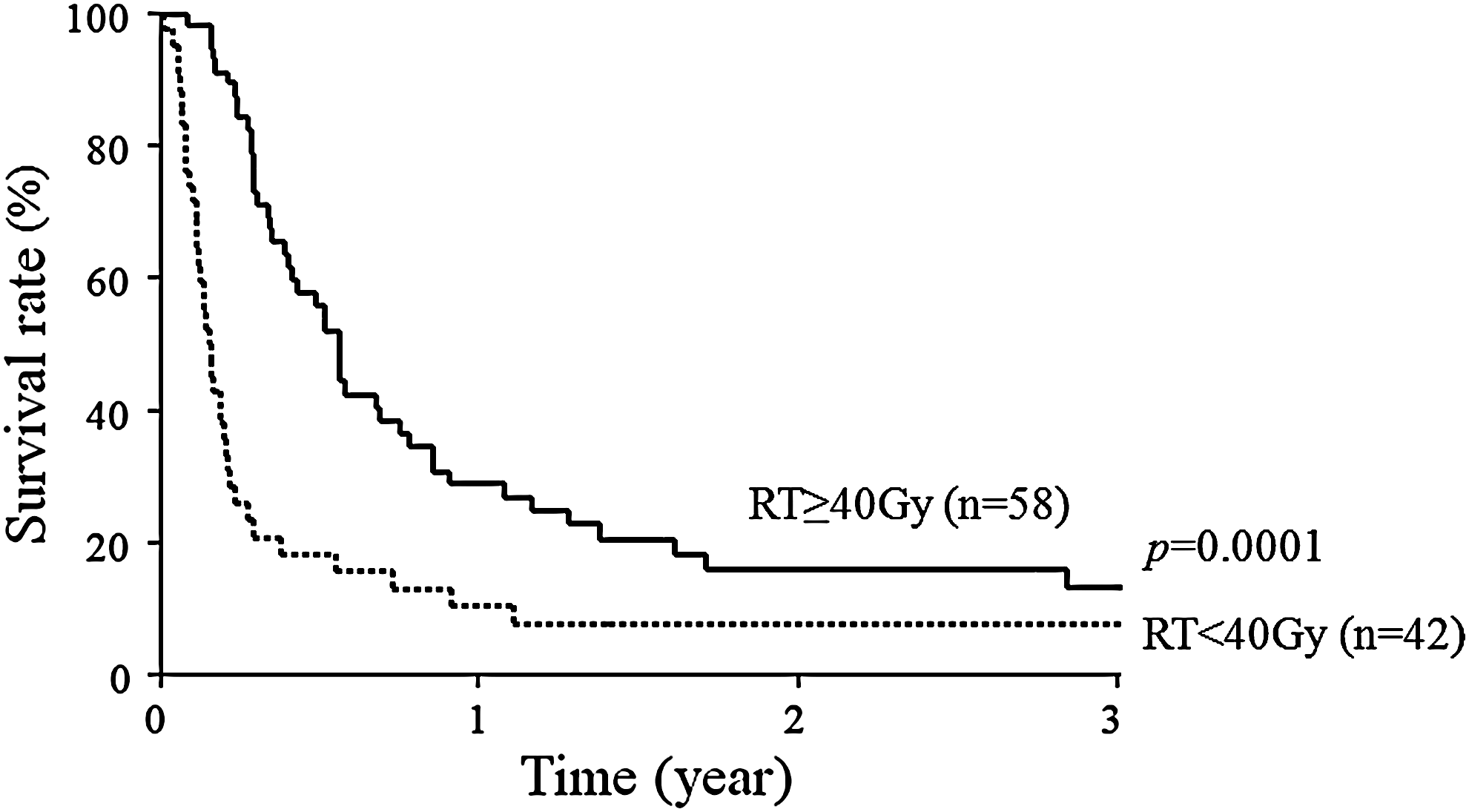
Comparison between the survival rates of the group of patients irradiated with a dose of ≥40 Gy and the group irradiated with a dose <40 Gy. The group of patients irradiated with a dose of ≥40 Gy had a better survival than those the group irradiated with a dose of <40 Gy (p<0.0001, log-rank test).
Ex, extrathyroidal invasion; RT, radiotherapy; CR, complete remission evaluated by CT, ultrasonography, and fine needle aspiration biopsy cytology.
Univariate analysis showed that a patient age of ≥70 years, male gender, a white blood cell (WBC) count of ≥10,000 mm3, a tumor size of ≥5 cm, extrathyroidal invasion (extension beyond the thyroid capsule), and distant metastasis at diagnosis were associated with significantly shorter survival (Table 3). Surgery, radiation, and multimodal therapy were associated with significantly longer survival, but chemotherapy was not. Multivariate analysis demonstrated that age ≥70 years, WBC ≥10,000 mm3, extrathyroidal invasion, distant metastases, not having had a surgical resection of the tumor, and radiation therapy with a dose of <40 Gy were risk factors for poorer survival (Table 4). We also studied outcomes in the group of 16 metastases-free patients who had complete tumor resection (Group MF-CTR), the group of 26 metastases-free patients who had incomplete tumor resection (Group MF-ITR), and the group of 58 patients with metastases (Group M). In the MF-CTR and MF-ITR groups, adjuvant radiotherapy was associated with significant longer survival, but chemotherapy was not. In the Group M, surgery and radiotherapy were associated with prolonged survival.
CI, confidence interval.
Discussion
It is well known that some ATCs arise as a result of anaplastic transformation of differentiated thyroid carcinoma (1,13 –19). In our series, 19% of the 100 patients had evidence of differentiated thyroid cancer. Six of the patients had a small focus of anaplastic transformation in a papillary carcinoma, and 13 patients had a history of previous surgery. This was for papillary carcinoma in 12 patients and for follicular carcinoma in 1 patient. The results of molecular biological studies have suggested that mutations of the genes encoding p53, beta-catenin, RAS, BRAF, and MIB-1 may be associated with anaplastic transformation (20 –25). It would be potentially beneficial if it were possible to use molecular target markers to predict the differentiated thyroid carcinomas that are most likely to undergo anaplastic transformation.
In contrast to differentiated thyroid carcinoma, the prognosis of ATC is poor. There is no standardized treatment protocol for ATC. Several studies have shown that complete resection prolonged the survival of ATC patients (7,9,10,26 –32). Pierre et al. treated 44 of 67 patients surgically over a 31-year period and reported 6-month, 1-year, and 3-year survival rates of 92%, 92%, and 83%, respectively, after complete resection; 53%, 35%, and 0%, respectively, after debulking; and 22%, 4%, and 0%, respectively, after no resection (6). Haigh et al. reported a median survival time of 43 months in patients treated by potentially curative resection when compared with 3 months in patients treated by palliative resection (p=0.002), and a multivariate analysis revealed that potentially curative surgery was the only discriminating variable that retained a significant association with prolonged survival (4). In contrast, neither extent of the operation nor complete resection was found to have improved the survival of 96 of the 134 ATC patients treated surgically at the Mayo Clinic during a 50-year period (5). In the recent study of 25 ATC patients at Mayo Clinic, it was reported that an aggressive approach combining intensity-modulated radiation therapy and radiosensitizing plus adjuvant chemotherapy appears to improve outcomes, including survival in stages IVA and IVB (33). In the present study, survival was found to be significantly better after surgical resection than after incomplete resection or no resection. Surgical treatment, including debulking neck tumors, is a better approach in terms of both local control and improvement of survival.
Postoperative radiotherapy has been recommended to achieve complete and partial remission (4,6,27 –30,33 –35). Our results suggested that significantly prolonged survival was associated with radiation doses of ≥40 Gy. Radiotherapy seems to be warranted to control local disease and improve quality of life.
Evaluating the efficacy of chemotherapy was even more difficult. The doses of the drugs given and the timing of their administration varied from patient to patient. In 2000, Ain et al. reported that paclitaxel appeared to be the only agent with significant systematic clinical activity against ATC in a phase 2 trial of administration by 96-hour infusion (36), and Higashiyama et al. reported better overall survival of stage IVB patients who underwent induction chemotherapy with weekly paclitaxel and in a group that received chemotherapy with a different drug than in a group that did not receive any chemotherapy (37). Although a PR was achieved in one patient who was treated with paclitaxel in our study, there was no significant difference in survival rate between the 9 patients in our study who received paclitaxel and the 91 who did not.
Multimodal therapy with a combination of surgery, radiation, and chemotherapy has been reported to improve outcome (3,28,29,34,36,38 –42). Tennvall et al. treated 55 patients with one of three protocols that combined doxorubicin, hyperfractionated radiotherapy, and surgery between 1984 and 1999 and found a strong correlation between local tumor control and acceleration of radiotherapy (39).
Nineteen patients survived for more than 1 year after diagnosis in our study. Six of these 19 patients had a small focus of ATC, 6 were treated with multimodal therapy consisting of surgery, radiotherapy, and chemotherapy, 12 were treated with surgery and radiotherapy, and the only 1 was treated with radiotherapy and chemotherapy alone, and not surgically because of local spread of the disease.
Sugitani et al. found that the presence of acute symptoms, a large tumor (>5 cm), distant metastasis, and WBC >10,000 mm3 were significant risk factors in a multimodal analysis and that these factors (prognostic index) were useful as a means of selecting patients for aggressive multimodal therapy (8). Smallridge et al. reported that in clinical studies of 1771 patients, the variables associated with survival in some series included age, tumor size, extent of surgery, higher dose radiotherapy, absence of distant metastases at presentation, coexistence of differentiated thyroid cancer, and multimodality therapy (43). In our study, multivariate analysis demonstrated that older age, high WBC, extrathyroidal invasion, distant metastasis at diagnosis, incomplete resection, and radiation therapy with a dose of <40 Gy were risk factors for poorer survival. The results of our study were similar to those of previous studies; however, leukocytosis was found to be associated with reduced survival, and tumor size was not. It is thought that ATC produces various growth factors, and multiple cytokines contribute to the neutrophilia associated with ATC. Sato et al. have implicated granulocyte colony-stimulating factor (CSF), interleukin 6, and macrophage CSF as possible causes of high neutrophil counts in ATC (44).
In this retrospective study, selection bias existed in determining the effect of treatment on outcome, because most of the patients who received surgery, radiotherapy, and chemotherapy had less extensive disease. We therefore studied outcomes in small groups: a group of patients without metastasis in whom complete surgical resection was possible, a group of patients in whom surgery was incomplete, and a group of patients with metastasis. In the group of patients without metastasis, adjuvant radiotherapy was associated with significant longer survival, but chemotherapy was not. In the group of patients with metastasis, surgery and radiotherapy were associated with prolonged survival.
We devised a treatment strategy in which patients without distant metastasis (stage IVA and IVB) are treated with multimodal therapy (surgery, radiotherapy, and chemotherapy), and patients with distant metastasis (stage IVC) are treated with radiotherapy and chemotherapy as neoadjuvant therapy before surgery. It seems that surgery should be performed as soon as possible to prevent death from asphyxiation in patients with distant metastases.
Conclusions
Although the prognosis of most patients with ATC continues to be poor, treatment at an early stage with combination of surgery, radiation, and chemotherapy is the only current way to improve the outcome. Further multicenter prospective studies are required to determine appropriate treatment for patients with ATC.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.