
Abstract
Background:
The impact of subclinical hyperthyroidism (sHT) on the cardiovascular system still needs to be elucidated. The aim of the study was to prospectively assess blood pressure (BP), variability in heart rate, and the prevalence of arrhythmias in patients with sHT, both before and after they are restored to the euthyroid state.
Methods:
The study group consisted of 44 normotensive patients (37 women, 7 men), aged 22–65 years (mean±SD: 45.9±11.0) with sHT. Enrolled patients were drawn from 1080 patients referred to our department for treatment of hyperthyroidism. Study patients were treated with radioiodine treatment to restore the euthyroid state. Ambulatory BP monitoring and Holter electrocardiography were performed (i) when sHT was diagnosed and (ii) at least 6 months after they became euthyroid.
Results:
sHT in comparison to the euthyroid state was associated with higher (109.3±7.1 vs. 107.1±7.7 mmHg) nocturnal systolic mean BP (p=0.035) and BP load (14.8 vs. 10.2%, p=0.033), mean diastolic BP (66.4±6.6 vs. 64.8±6.6 mmHg, p=0.047), and mean arterial pressure (80.8±43.1 vs. 79.3±43.6 mmHg, p=0.049). Moreover, significant changes in both the time and frequency domain measures of heart rate variability (HRV) were observed: decrease of the square root of the mean squared differences of successive NN intervals (rMSSD) (45.68±34.1 vs. 65.09±50.6 ms, p=0.03) and the low frequency power (LF) (5.71±0.99 vs. 6.0±1.01 ms2, p=0.049) as well as increase of QT interval dispersion (58.25±28.5 vs. 46.90±12.1 ms, p=0.020). This was accompanied by a clinically insignificant increase in the frequency of ventricular extrasystoles (VES) (3.1±7.4 vs. 0.6±1.2 per hour, p=0.048) and increased mean heart rate (78.4±6.8 vs. 76.0±8.0 beats/min, p=0.004). Some of the parameters correlated positively with thyroid hormones: nocturnal diastolic BP with free triiodothyronine (FT3) (r=0.397, p=0.008), rMSSD with free thyroxine (FT4) (r=0.389, p=0.013), and QT interval dispersion with FT4 (r=0.450, p=0.004).
Conclusions:
The study suggests that sHT in comparison to euthyroid status may be associated with a statistically significant but probably clinically insignificant increase of QT interval dispersion, prevalence of VES, elevated nocturnal arterial BP, and changes in HRV. These findings broaden our understanding of the cardiovascular effects of sHT.
Introduction
The aim of the present study was to prospectively assess BP, heart rate variability (HRV), and the prevalence of arrhythmia in patients with sHT, before and after they were treated to restore the euthyroid state.
Methods
The study group consisted of 44 patients who were diagnosed with endogenous sHT on the basis of (i) a serum TSH concentration below the assay normal range (<0.36 mIU/L) in at least two measurements, performed at the interval of 6 weeks to exclude subjects with temporary TSH suppression and (ii) free thyroid hormones within the normal range, for free triiodothyronine (FT3), this being 3.5–7.9 pmol/L, and for free thyroxine (FT4), this being 7.64–19.7 pmol/L in at least two measurements performed at an interval of 6 weeks. In addition, the study was confined to patients with negative anti-thyroid peroxidase, anti-thyroglobulin, and anti-TSH receptor autoantibodies. Therefore, we attempted to exclude patients with autoimmune thyroid disease. In our study, sHT was caused by toxic multinodular goiter, diffuse thyroid autonomy, and autonomous nodules. All study patients had a negative history of other diseases and were taking no medications.
After the diagnosis of sHT, the patients were treated with radioiodine. The dose of 131I was calculated according to the following formula (7), where A is activity in mCi, m is mass of thyroid tissue in grams, and RAIU24 is the fractional 24 hour radioactive iodine uptake.
The protocol of the study was in accordance with the Declaration of Helsinki, and was approved by the local ethics committee, with all patients giving informed consent to participate. In all the subjects, concentrations of TSH and free thyroid hormones were assessed on admission, as well as during follow-up visits every 3 months subsequent to radioiodine therapy, using commercially available AutoDELFIA kits. Additionally, each patient underwent thyroid Tc-99m scintiscan and RAIU24 assessment as well as thyroid ultrasound examination, performed by the same experienced sonographer with a 7.5 MHz linear probe (GE; VingMed System Five). Tc-99m and 131I were obtained from POLATOM. Thyroid volume was measured by the means of elliptical shape volume formula (π/6×length×width×depth).
Hypertension was excluded on the basis of their medical history and standard BP measurements in study subjects. Noninvasive ABPM was performed in all the patients by the oscillometric method (Spacelabs 90217). BP measurement was performed at intervals of 20 minutes during the day (from 7 am to 11 pm) and of 30 minutes at night (from 11 pm to 7 am). Median time of a single evaluation was 23.6±1.4 hours and included 56±3.4 measurements. During ABPM, median systolic blood pressure (SBP) and diastolic blood pressure (DBP) were assessed for the day and night time, separately as well as for the whole 24 hours. The following upper BP limits were assumed as normal values: <135/85 mmHg during the day, <120/75 mmHg at night, and <130/80 mmHg for the whole 24 hours. Subjects being considered for inclusion in the study group were not included if their BP exceeded the reference range.
Mean arterial pressure (MAP) was calculated with the use of the following formula: MAP=(2×DBP+SBP)/3, while the pulse pressure (PP) was calculated as PP=SBP−DBP. Additionally, the analysis involved an assessment of 24-hour, as well as short-term BP variability. The former, defined as a nocturnal SBP, or DBP fall (%), was calculated by 100× [1−(night BP/day BP)]. The latter was expressed as a standard deviation of median SBP and DBP during ABPM; BP load was expressed as a percentage of values above a given reference limit (8).
All the patients underwent 24-hour 12-lead electrocardiographic monitoring with the simultaneous assessment of HRV using a H12 24hECG digital recorder by Mortara Instrument (Milwaukee). For data analysis, original Mortara Instrument software was used (HScribe v.3.40). Evaluation of ST-segment was performed to detect ischemia. The sinus rhythm HRV was assessed on the basis of (i) the time domain measures • SDNN (ms): standard deviation of all normal RR intervals, measured between consecutive sinus beats • SDANN (ms): standard deviation of all the 5-minute intervals normal RR interval means • rMSSD (ms): the square root of the mean of the squared differences between successive NN intervals over 24 hours • pNN50 (%): the difference (expressed as a percentage) between successive NN intervals over 24 hours greater than 50 ms (ii) the frequency domain measures performed with the use of the method of fast Fourier transform • TP (ms2): total power • LF (0.04–0.15 Hz) (ms2): low frequency power • HF (0.15–0.4 Hz) (ms2): high frequency power • LF/HF ratio
Nocturnal 5-minute electrocardiograms assessed during sleep were subject to frequency analysis of HRV, containing 2.5 minutes before and 2.5 minutes after the moment of registration of the lowest MAP in 24 hours, and characterized by the most stable ECG recording. The lowest nocturnal mean BP was chosen as a reference time point for the HRV analysis according to the results from the previous studies, demonstrating a significant negative correlation of spectral power components with the night BP level and their positive correlation with the magnitude of a night fall in systolic and DBP (9). Apart from these measurements, the lowest BP values were applied to assure even more reproducible conditions for consecutive follow-up evaluations, that is, assessment in a “window” on the highest circadian values of both spectral components.
Additionally, in 24hECG, the following parameters were assessed: • heart rate: median, maximal, and minimal • QT interval dispersion—with manual method, as the difference between the longest and the shortest QT interval from all leads • the type and severity of arrhythmia
The assessment of patients was performed twice—at the moment of diagnosis of sHT and 6 months after restoring euthyroidism, confirmed by complete TSH normalization. Repeated TSH tests performed every 3 months during the follow-up after radioiodine treatment allowed us to precisely detect the moment of transition from sHT to normal thyroid function, and to confirm that all patients during the second evaluation were euthyroid for at least 6 months.
In the statistical analysis, Student's t-test for dependent and normally distributed variables was used for comparisons of thyroid hormone concentrations, thyroid volume, the parameters measured during ABPM, and the 24 hours ECG. Due to their skewed distributions, spectral components of HRV were transformed by calculating their natural logarithm. All transformed parameters showed a normal distribution that was tested with the Kolmogorov–Smirnov and Shapiro–Wilks tests. The correlation between hormone concentrations and parameters measured during ABPM as well as 24hECG was calculated and presented with the use of linear regression (Pearson's test). All calculations were performed with STATISTICA version 8.0. Assumed significance level was set at 0.05.
Results
In all, 44 patients (37 women and 7 men), aged 22–65 years (mean 45.9±11.0) were enrolled to the study. Toxic multinodular goiter was diagnosed in 38 patients, diffuse thyroid autonomy in four patients, and a autonomous thyroid nodule in two patients. The mean TSH, FT3, and FT4 values differed significantly in measurements performed when patients were in the sHT state and the euthyroid state. Serum TSH concentrations before radioiodine treatment were 0.16±0.1 mIU/L and were 1.32±0.75 mIU/L when the euthyroid state was restored, indicating that serum TSH increased and free thyroid hormones declined after radioiodine treatment (Table 1). In 30 of the study patients, serum TSH was partially suppressed (0.1–0.36 mIU/L) at enrolment into the study and in the remaining 14 patients, serum TSH was <0.1 mIU/L. The median time between establishing the diagnosis of sHT and administrating radioiodine treatment was 12.7 months. This included the waiting period for admission to hospital, repeat hormonal assessment, and evaluation of indications and contraindications for radioiodine treatment (e.g., confirmation of a permanent form of nonautoimmune sHT, exclusion of malignancy on the basis of cytological examination from fine-needle aspiration biopsy). The mean period between the administration of radioiodine and restoration of the euthyroid state was about 6.9 months.
Statistically significant differences are shown in bold.
sHT, subclinical hyperthyroidism; SD, standard deviation, FT4, free thyroxine, FT3, free triiodothyronine; TSH, thyrotropin.
The mean thyroid volume was 33.4±18.8 mL before and 22.4±14.6 mL after radioiodine therapy (p<0.001). The RAIU24 ranged from 19% to 81%, with a median value of 30%. The radioiodine doses given were within a range of 185 MBq (5 mCi) and 1125 MBq (30 mCi), while the median dose given was 448 MBq (12 mCi).
As a result of radioiodine treatment, all the patients eventually achieved the euthyroid state during as long as a 36-month follow-up period. Three patients had transient exacerbation of hyperthyroidism 3 months after radioiodine administration, requiring a short period of methimazole treatment. After cessation of the drug, two patients were consistently euthyroid, and one patient developed subclinical hypothyroidism, requiring levothyroxine (LT4) substitution. Another two patients developed hypothyroidism in the 21 months after radioiodine administration. In all hypothyroid patients, LT4 treatment restored the euthyroid state.
The median time between the two ABPM sessions was 12.5 months. The obtained during these sessions is presented in Table 2. There was a significant decrease in median and load of nocturnal SBP, median DBP, and MAP after the radioiodine treatment. The other parameters that were measured were not significantly different before, compared with after, radioactive iodine treatment.
Statistically significant differences are shown in bold.
SD, standard deviation; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; NS, not significant; PP, pulse pressure.
A significant positive correlation (Fig. 1) was found between FT3 concentration before radioactive iodine treatment and the following parameters: nocturnal SBP (r=0.322, p=0.047), nocturnal DBP (r=0.397, p=0.008), and nocturnal MAP (r=0.334, p=0.027). Correlations between other parameters were not significant (Table 3).
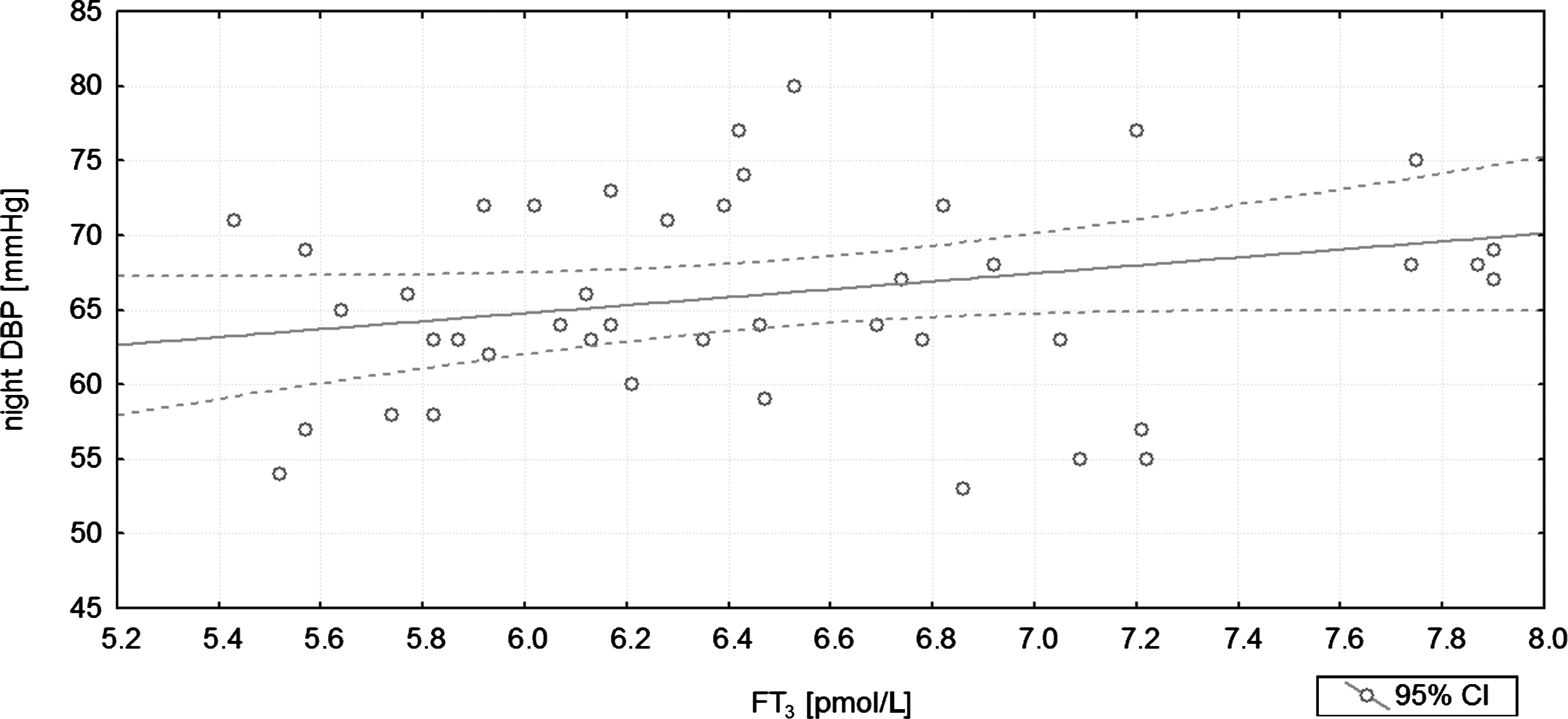
The positive correlation between the nocturnal diastolic blood pressure (night DBP) and free triiodothyronine (FT3) concentration (r=0.397; p=0.008; R 2=0.083) before treatment. The variance of night DBP is explained by the variance of FT3 in the degree equal to R 2.
Significant correlations are shown in bold.
The analysis of 24hECG revealed significantly decreased rMSSD, decreased LF of HRV, and increased QT interval dispersion in sHT in comparison to euthyroidism. Moreover, the mean heart rate was significantly higher, and ventricular extrasystoles (VES) occurred significantly more frequently in patients when they were initially studied compared with after they became euthyroid (Table 4). There were no significant differences in standard deviation of all NN intervals (SDNN), standard deviation of the averages of NN intervals in all 5-minute segments (SDANN), the TP, the HF, the LF/HF ratio, incidence of supraventricular extrasystoles, as well as minimal and maximal heart rate before and after radioactive iodine treatment. There was a significant positive correlation between rMSSD and FT4 (r=0.389, p=0.013, Fig. 2). In addition, there was a significant positive correlation between QT interval dispersion and serum TSH (r=−0.316, p=0.048), FT4 (r=0.45, p=0.004, Fig. 3) and FT3 (r=0.377, p=0.017). There was no correlation between thyroid function test results and the prevalence of supraventricular extrasystoles, heart rate, LF and HF.
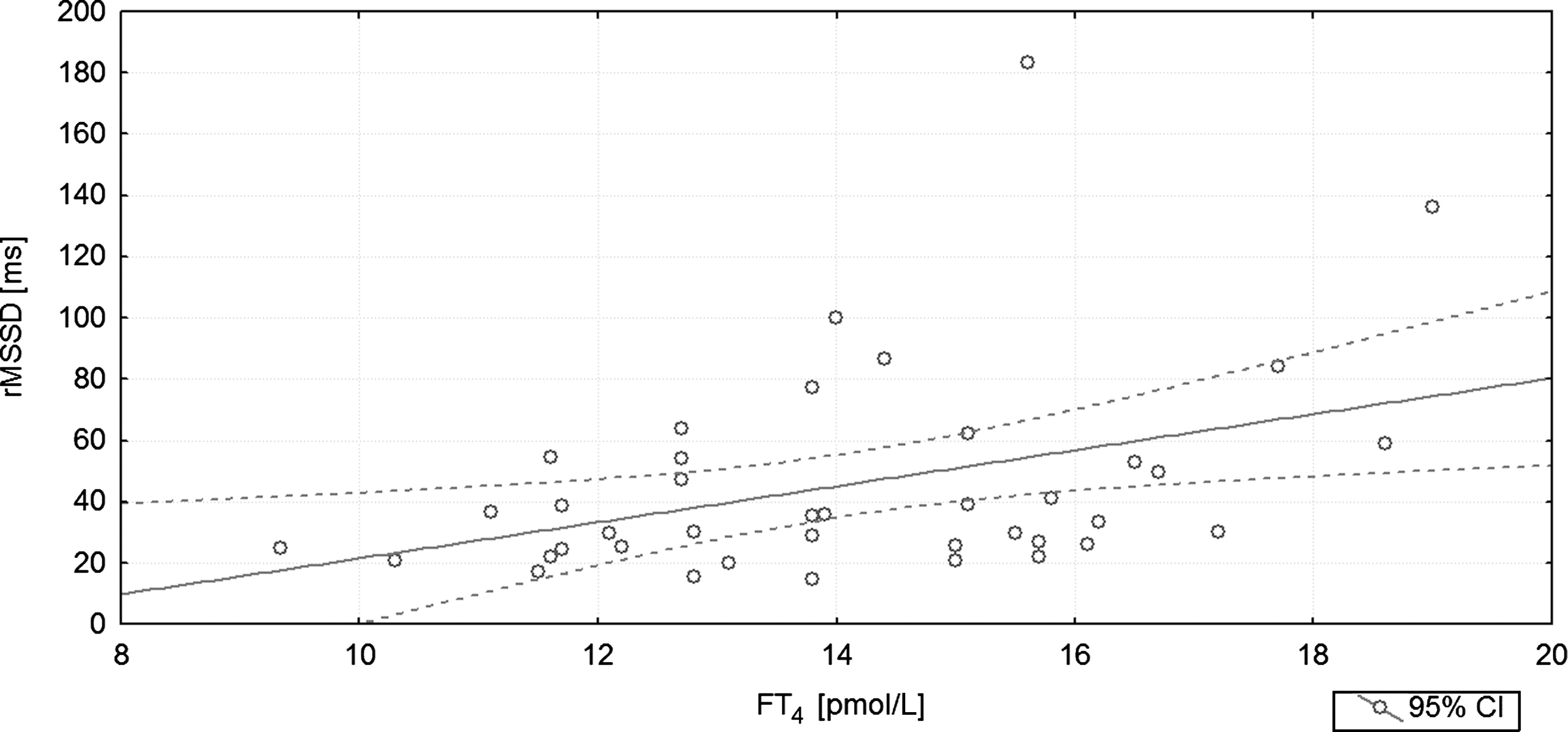
The graph illustrates the positive correlation between rMSSD and free thyroxine (FT4) concentration (r=0.389; p=0.013; R 2=0.212) before treatment. The variance of rMSSD is explained by the variance of FT4 in the degree equal to R 2.
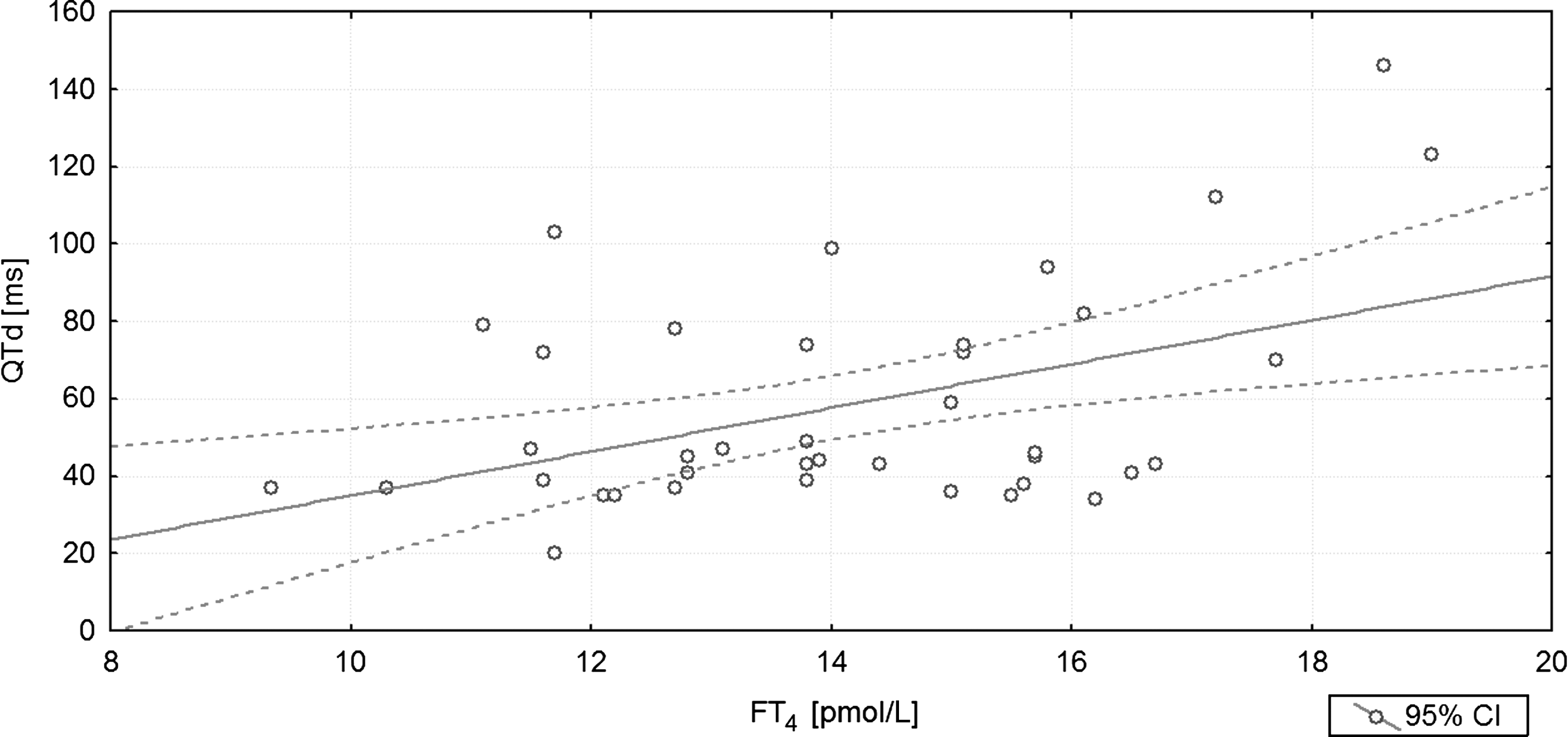
The graph illustrates the positive correlation between QT interval dispersion (QTd) and FT4 concentration (r=0.450; p=0.004; R 2=0.363) before treatment. The variance of QTd is explained by the variance of FT4 in the degree equal to R 2.
The presentation is limited to data for which differences between the sHT and euthyroid state were noted. The frequency domain measures are presented in a logarithmic scale.
rMSSD, root mean successive square difference; lnLF, natural logarithm of low frequency component; QTd, QT interval dispersion; VES, ventricular extrasystoles; HR, heart rate.
A separate analysis was performed in the subgroup of patients whose initial serum TSH was <0.1 mIU/L. In this analysis, there were significant differences between the initial data and the data when the euthyroid state was restored in the parameters LF/HF (p<0.005) and QT interval dispersion (p=0.0412).
Discussion
Most studies on the cardiovascular system and sHT provide information on patients receiving excessive doses of thyroid hormone, referred to here as exogenous sHT (2,4,10 –12). There are probably important differences in the duration and degree of thyrotoxicosis in exogenous sHT and sHT that are due to endogenous causes such as toxic multinodular goiter. Therefore, it may not be accurate to draw conclusions about endogenous sHT from studies of exogenous sHT.
Our studies of endogenous sHT indicate that it is characterized by an increased median and nocturnal SBP load, median DBP, and MAP. Additionally, there is a positive correlation between median and nocturnal SBP load, median DBP and MAP, and serum FT3 concentrations. There are numerous reports that there is a positive correlation between the systolic or DBP and the risk of cardiovascular incidents (8,13,14). Sesso et al., in a large population-based study in which 11,150 subjects without a history of hypertension or any other cardiovascular disease were observed, reported a positive correlation between SBP, DBP, and MAP and the risk of cardiovascular disease, especially in subjects over 60 years old (15).
We are not aware of any other study that employs ABPM to assess the impact of endogenous sHT on the cardiovascular system; there are studies of relatively small groups of subjects with exogenous sHT. Casu et al., in a group of 12 patients treated with LT4 to achieve TSH suppression after thyroidectomy due to thyroid cancer, observed increased systolic and MAP in comparison to 24 healthy controls (16). However, Ching et al., who studied in 11 subjects with exogenous sHT, did not observe differences in ABPM parameters between these and control subjects (10).
The increase within the normal range in the systolic, diastolic, and MAPs observed here was observed in nocturnal BP measurements. In the nocturnal period, the parasympathetic nervous system predominates (17), and external stimuli are less influential than during daily activity. The correlation found between the nocturnal SBP, DBP, MAP, and the severity of hyperthyroidism suggests a particular influence of FT3 concentration on BP values in sHT.
In the study by Faber et al., there was a significant decrease of 11% in the heart rate of six women who transitioned from endogenous hyperthyroidism to euthyroidism after radioiodine treatment (18). This is consistent with our observations in sHT. Biondi et al. compared the 24 hours ECGs in 23 patients with sHT with that in healthy age-, gender-, and lifestyle-matched controls (3). The patients in this study were comparable to those in the present study with regard to age and serum TSH levels. In patients with sHT, Biondi et al. noted a greater mean heart rate compared with controls, findings that correspond to ours. In contrast to our results, these authors found an insignificant increase in the incidence of supraventricular extrasystoles in these patients. Sgarbi et al. compared data from 10 subjects with sHT (median age 59 years, mean TSH<0.05 mIU/L) with data in the same subjects after their TSH had been normalized by methimazole treatment. This study also included a control group of 10 healthy subjects, matched for age, gender, and body mass index with the patients with sHT (6). In this study the mean heart rate was higher and the number of supraventricular and VES was greater in the patients with sHT before they were treated compared with after they were treated and also in comparison to the healthy control subjects. This was similar to our findings. A significant negative correlation was additionally observed between TSH concentration and prevalence of extrasystoles, and also a positive correlation between FT4 concentration and mean heart rate, or occurrence of extrasystoles was observed. In the present study, however, there was no significant relationship between the thyroid hormone levels and prevalence of extrasystoles. The present study noted a significant increase of QT interval dispersion, yet in normal ranges, in patients with sHT. This may be particularly important for subjects with ischemic heart disease, in whom even mild excesses of thyroid hormones might upset the electrical balance in ischemic heart muscle. It is assumed that both heterogeneous repolarization in ventricles (being a substrate for re-entry circuits) and VES (initiating arrhythmias) have a role in the development of life-threatening ventricular arrhythmias (19).
In the present study, among the time domain measures, a relatively low value for rMSSD was noted in sHT. The rMSSD reflects vagal nerve activity (20). If frequency domain measures were concerned, then the LF of HRV was decreased in sHT. A study performed on disparate population showed a significant decrease in both the LF and HF of HRV in survivors of sudden cardiac arrest. There was a negative correlation between the LF component value and one-year mortality (21). In patients with chronic heart failure, decreased short-term LF acquired from 5-min ECG sections in standardized conditions, that is, in a supine position during controlled breathing, was a powerful predictor of sudden death independent of many other variables (22). The increase in the LF observed after restoring euthyroidism may be indicative of a decreased risk of ventricular arrhythmia and elevated threshold for ventricular tachycardia (23).
There are only two reports of HRV in sHT in the literature (24,25). Petretta et al., studied HRV in 30 patients with endogenous sHT and 20 healthy controls; in this study, the parameters reflecting the activity of parasympathetic nervous system were significantly lower in patients with sHT than in the control patients (25). Osman et al. compared time domain measures of HRV in 259 patients with overt hyperthyroidism. There were 110 patients in whom free thyroid hormone concentrations normalized but TSH was still suppressed during treatment and 219 patients in whom both free thyroid hormone and TSH concentrations normalized (24). The study also included 440 euthyroid controls. In patients with clinically evident and subclinical hyperthyroidism, concordant results were obtained, indicating attenuation of cardiac vagal modulation. In our study, similarly, a significant and concordant change in both time and frequency domains of HRV occurred as a result of treating sHT with radioactive iodine.
There is no information in the literature regarding QT interval dispersion and time and frequency domain measures of HRV, as these relate to the severity of endogenous sHT. The present study suggests that excess thyroid hormones in sHT have a slight effect on the increase in QT interval dispersion and the decrease in HRV.
To maintain homogeneity of the studied group and to eliminate the variable character of thyroid function in autoimmune thyroid disease, patients with hyperthyroidism due to autoimmunity were largely excluded from this study. Most patients had toxic nodular thyroid disease. The four patients diagnosed with diffuse thyroid autonomy had thyroid ultrasounds that were not characteristic for either Graves disease or thyroid nodules (or the lesions were smaller than 1 cm), negative anti-TSH receptor autoantibodies, and diffusely increased radioisotope uptake on thyroid scintiscan.
With the applied methodology, we were also unable to exclude possible undesirable effects of automatic BP measurements on autonomic activity, or to distinguish respective sleep phases that can also influence autonomic balance. Nevertheless, the information from the patients' diaries concerning the periods of sleep and its discontinuity was evaluated meticulously, and for analysis, we selected only 5-minute ECG sections free from artefacts and marked abrupt changes in RR interval.
The main advantages of our study are that the research was prospective and that ABPM and the 24-hour ECG were evaluated, and obtaining measurements after the euthyroid state was restored had allowed, in the same patient, the measurements when the patient was euthyroid to serve as the control for the period of subclinical thyrotoxicosis. Additionally, a relatively large group of patients were studied, and they had endogenous sHT, which is generally more pertinent than exogenous sHT. We conclude that sHT may be associated with a small, though not necessarily clinically important, increase of QT interval dispersion, incidence of VES, elevated nocturnal arterial BP, and changes in HRV. These findings should be taken into consideration in future studies of the overall impact of varying degrees of thyrotoxicosis on the cardiovascular system.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.