
Abstract
Background:
Pituitary metastases are found in about 1% of all pituitary resections. They often derive from breast, lung, and gastroenteric tract adenocarcinomas, very rarely from thyroid carcinoma. Presenting symptoms of thyroid carcinoma metastatic to the pituitary gland are usually chiasmatic with central neurological impairment due to space-occupying expansion in the parasellar region. Hypopituitarism is more often associated with papillary and medullary rather than follicular thyroid carcinoma (FTC). Here we describe a patient with pituitary metastasis from FTC who had hypopituitarism with thyrotropin (TSH) deficiency.
Summary:
A 61-year-old woman, who presented with visual deficits and pain to the right orbit, was found on magnetic resonance imaging to have a large mass involving the pituitary gland. She was found to have pituitary insufficiency based on corticotropin-releasing hormone and TSH-releasing hormone testing. Transnasopharyngeal biopsy of the mass revealed metastases from FTC. After total thyroidectomy, which confirmed widely invasive FTC, the patient underwent external beam radiation therapy of the metastases for progressive neurological symptoms and an increase in orbit pain. Since endogenous TSH production was insufficient, we used recombinant human TSH (rhTSH) as preparation for a series of radioiodine treatments. rhTSH administration, followed by 7.4 GBq of 131I, was repeated seven times over a 10-year period. This was associated with a marked decrease in serum thyroglobulin levels accompanied by substantial clinical improvement, but after 7 years disease progression occurred.
Conclusions:
Seven patients with pituitary metastases from FTC have been reported. In all cases, some neurological signs and symptoms related to mass effect were reported, but no pituitary insufficiency was described. This may be the first case of FTC with metastases to the pituitary causing hypopituitarism. It seems likely that management of such cases could be limited to biopsy to confirm thyroid carcinoma, rather than more extensive surgery, and that this could be followed by multiple treatments with rhTSH followed by 131I.
Introduction
Distant metastases, usually to lung and bone, occur in 10–15% of patients with differentiated thyroid carcinoma (DTC). In these cases, radioiodine treatment is associated with a clinical improvement and a reduced recurrence rate if the 131I accumulates well in the lesion (19), but this requires serum thyrotropin (TSH) concentrations to be elevated, either as a result of hypersecretion of endogenous TSH or administration of recombinant human TSH (rhTSH). rhTSH is required in patients with pituitary insufficiency. In 1997, Rudavsky and Freeman published the first report of the off-label use of rhTSH as a substitute for thyroid hormone withdrawal to prepare patients with metastatic thyroid cancer for therapeutic 131I (20). In 2006, Robbins reported on 115 patients treated with rhTSH to prepare them for 131I therapy of metastatic DTC (21). Here we describe a patient with PM from FTC who presented with hypopituitarism. This may be the first time that a patient with sella metastases from FTC has been reported to present with pituitary insufficiency.
Patient
In March 2001, a 61-year-old woman presented with visual field deficits and pain to the right orbit. She was found on magnetic resonance imaging (MRI) to have a large mass involving the pituitary gland (Fig. 1). Anterior pituitary function tests showed pituitary insufficiency. There was no adrenocorticotropic (ACTH) and cortisol response, or TSH response, after corticotropin-releasing hormone and TSH-releasing hormone administration, respectively (Table 1). She did not have polyuria or polydipsia.

Large metastatic lesion of the base of the skull involving the pituitary gland on magnetic resonance imaging. The white arrow indicates the lesion.
ACTH, adrenocorticotropic hormone; CRH, corticotropin-releasing hormone; FSH, follicle-stimulating hormone; FT3, free triiodothyronine; FT4, free thyroxine; LH, luteinizing hormone; TRH, thyrotropin-releasing hormone; TSH, thyrotropin; PRL, prolactin.
A transnasopharyngeal biopsy of the sella lesion was performed to obtain a definitive diagnosis as well as decompression, as clinical signs of neural structure compression were present. A pathological diagnosis of metastatic FTC was made. Subsequently, the patient underwent a total thyroidectomy revealing a widely invasive FTC measuring 3.5 cm. Thereafter, replacement therapy with levothyroxine (100 μg/day) and oral cortisone acetate (25 mg/day) was started.
After thyroid surgery, the patient underwent external beam radiotherapy (40 Gy in 20 fractions) to the sellar region; at this time, she was experiencing progressive neurological symptoms and an increase in orbit pain. In September 2001, the patient was referred to the Radiotherapy and Nuclear Medicine Unit of the Istituto Oncologico Veneto of Padua, where she was treated with 7.4 GBq of 131I after rhTSH preparation. rhTSH was administered on two consecutive days (0.9 mg via i.m. injection, days 1 and 2) followed by oral administration of 7.4 GBq of 131I on day 3. Serum samples for thyroglobulin (Tg), Tg antibodies (Tg-Abs) and TSH measurements were collected on day 1 before the first rhTSH injection. Serum samples for TSH and Tg were repeated on day 3. The post-therapy whole-body scan (WBS), performed on day 6, showed intense 131I uptake in the thyroid bed, base of the skull region, and left lung.
Follow-up was performed by the endocrinology group in Ancona and the radiation-oncology group in Padua. Tg, Tg-Abs and TSH measurements were performed every 6 months and MRI of the brain every year. Computed tomography (CT) or plain radiography of the chest was carried out yearly. During the next six-and-one-half years, radioiodine therapy after rhTSH administration, using the same preparation schedule and the same 131I activity, was repeated six times. The last treatment was administered in February 2008. After this treatment, the post-therapy WBS showed an intense 131I uptake in the base of the skull region and weak uptake in the right lung (Fig. 2).
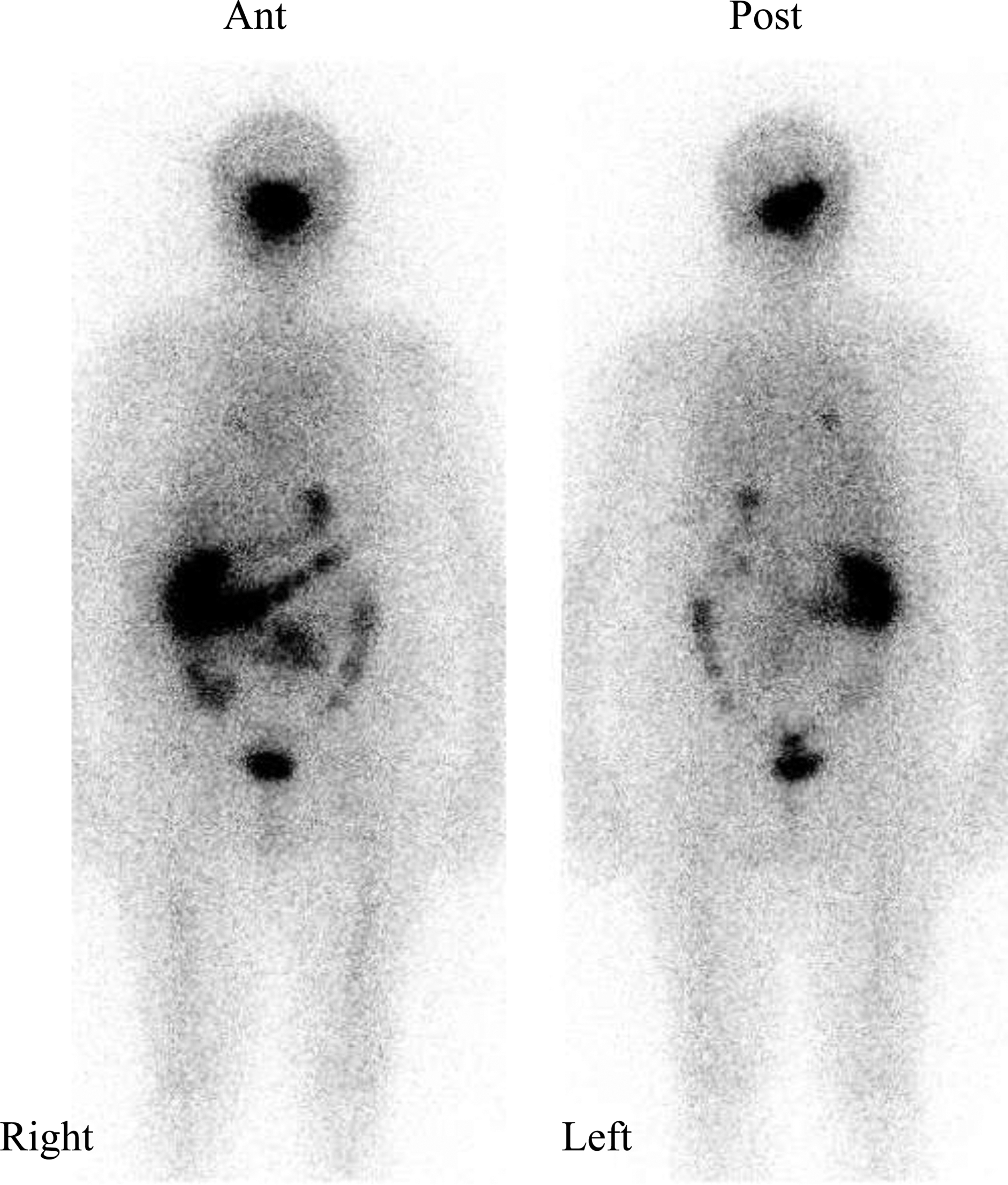
Post-therapy whole-body scan of the last radioiodine treatment showing an intense 131I uptake in the base of the skull region and weak uptake in the right lung.
Table 2 shows data about the 131I treatments and follow-up. Tests for serum Tg-Abs were always negative. During the first 6 years of follow-up, the patient had a partial clinical and radiological response and a good quality of life. We observed a significant drop in the serum Tg level at the time the patient was taking thyroid hormone. The serum Tg decreased from 415 ng/mL to 30 ng/mL during the first 4 years of follow-up and to 50 ng/mL in the next 2 years (Fig. 3). Lung 131I uptake was present but lung CT was negative until July 2009 when small bilateral lung lesions were observed. After October 2007, the serum Tg levels began to increase. In September 2009, a left gluteus metastatic lesion with bone involvement was observed. This lesion was treated with arterial embolization, obtaining a good response. In July 2010, the patient was still alive with disease progression. The brain MRI showed an increase in the pituitary mass and the skull lesion. CT examinations were consistent with stable lung and gluteus disease.
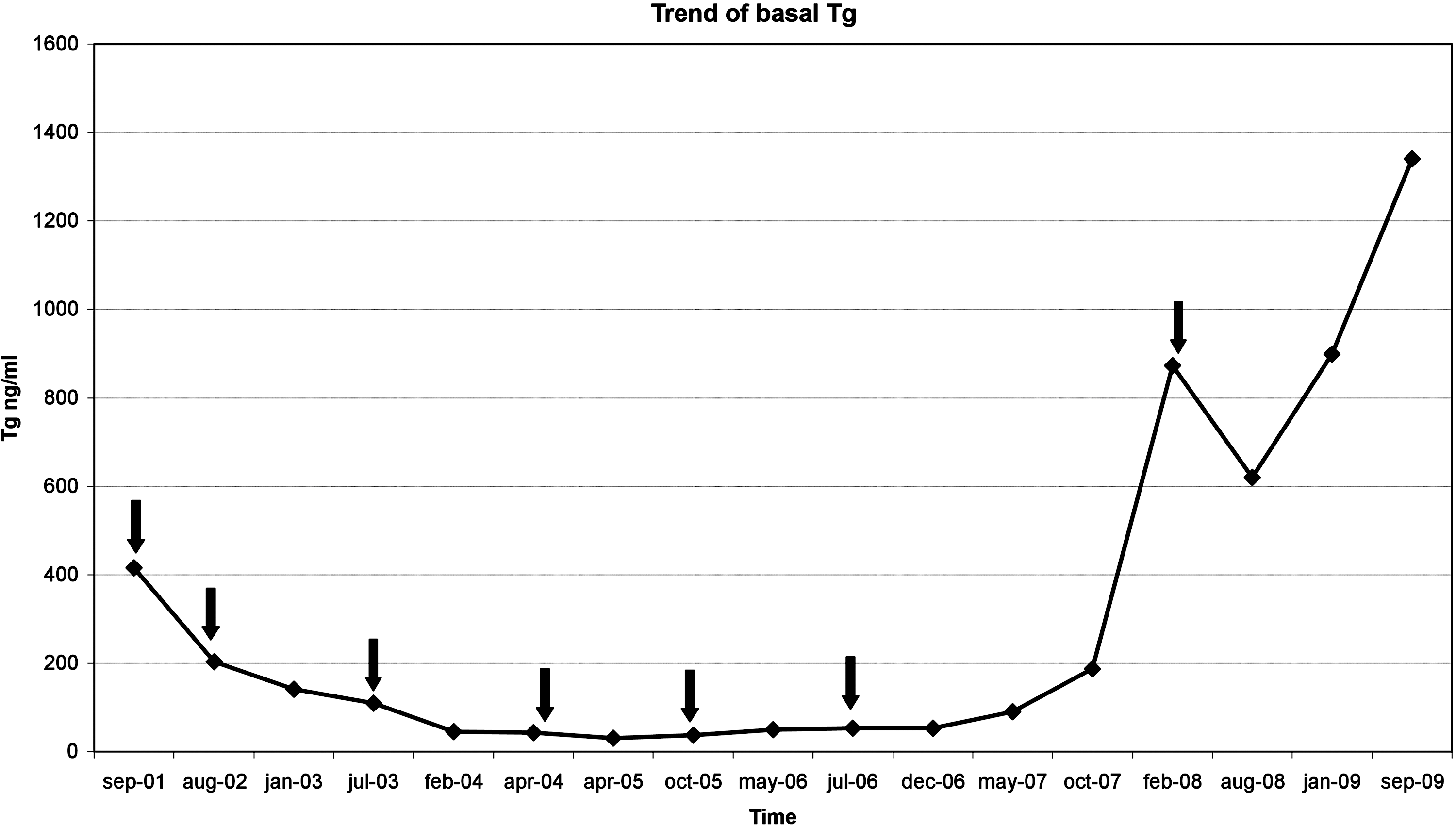
Trend of serum basal thyroglobulin over time. The black arrows indicate the seven 131I treatments.
Tg (mcg/L) and TSH (mL/L) serum measurements are listed in basal conditions and after recombinant human TSH stimulation. Post-therapy WBS, radiological imaging, and clinical status are reported.
Tg, thyroglobulin; MRI, magnetic resonance imaging; WBS, whole-body scan.
Discussion
PM are found in about one percent of all pituitary tumor resections (2). To date, 15 cases of metastatic thyroid carcinomas involving the sella turcica and/or the pituitary gland have been reported. Two of these were medullary thyroid carcinoma, six were PTC, and seven were FTC (5 –18).
Rapidly growing sella masses with a history of cancer elsewhere along with the rapid development of pituitary hormone deficiencies suggest underlying PM. As reported in a recent review by Prodam et al. (17), PM from DTC produces signs and symptoms related to mass effect rather than hypopituitarism. Pituitary insufficiency was observed only in five out of six cases of PM from PTC (6,8,10,11) and was not present in the seven cases of PM from FTC, but neurological signs and symptoms related to mass effect were typical (5,7,9,12 –14,17).
It has been reported that direct soft-tissue metastases to the pituitary gland parenchyma are quite rare, with many of such metastases emanating from neighboring bone deposits that can be microscopic (22). In our patient, it was difficult to determine whether pituitary insufficiency was due to adjacent osseous or hematogenous metastasis; both typical routes of FTC metastases.
Since there have been so few cases, there are no studies comparing different modalities for treating PM from DTC. However, a combined surgical and radiation approach seems rational, the former to obtain definitive diagnosis and relieve acute signs due to mass effect. Radioiodine is highly effective in the treatment of metastatic DTC, and its use in 11 out of 13 cases of PM from DTC has been reported. In these reports, rhTSH was used to prepare patients for radioiodine treatment; two of these patients had PTC and one had FTC (10,12). In our patient, we observed that rhTSH was well tolerated and serum TSH level increased to ≥50 mU/L after each rhTSH treatment, a level that has been considered sufficient to stimulate 131I uptake not only in normal thyroid but also in DTC tissue. This was accompanied by an acute rise of serum Tg 24 hours after the second intramuscular rhTSH injection. After rhTSH stimulation, the patient had 131I uptake in the post-therapy WBS, either in thyroid remnants or in metastatic sites. Interestingly, the FTC continued to respond to rhTSH with an increase in radioiodine uptake for many years, permitting repeated radioiodine treatments.
In summary, we report the very rare occurrence not simply of PM from DTC but also of PM from FTC that was associated with pituitary insufficiency including TSH deficiency. Since it has been employed in other settings, rhTSH administration was of critical importance in facilitating successful radioiodine treatment.
Footnotes
Acknowledgments
The authors thank Denise Kilmartin for editing the manuscript. Patient's data, reported herein, were derived from a follow-up study approved by our Institutional Review Board. Patient's written informed consent was obtained.
Disclosure Statement
The authors declare that no competing financial interests exist.